
Reconstruction of Segmental Bone Defect in Canine Tibia Model Utilizing Bi-Phasic Scaffold: Pilot Study
 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Scaffold Characterization
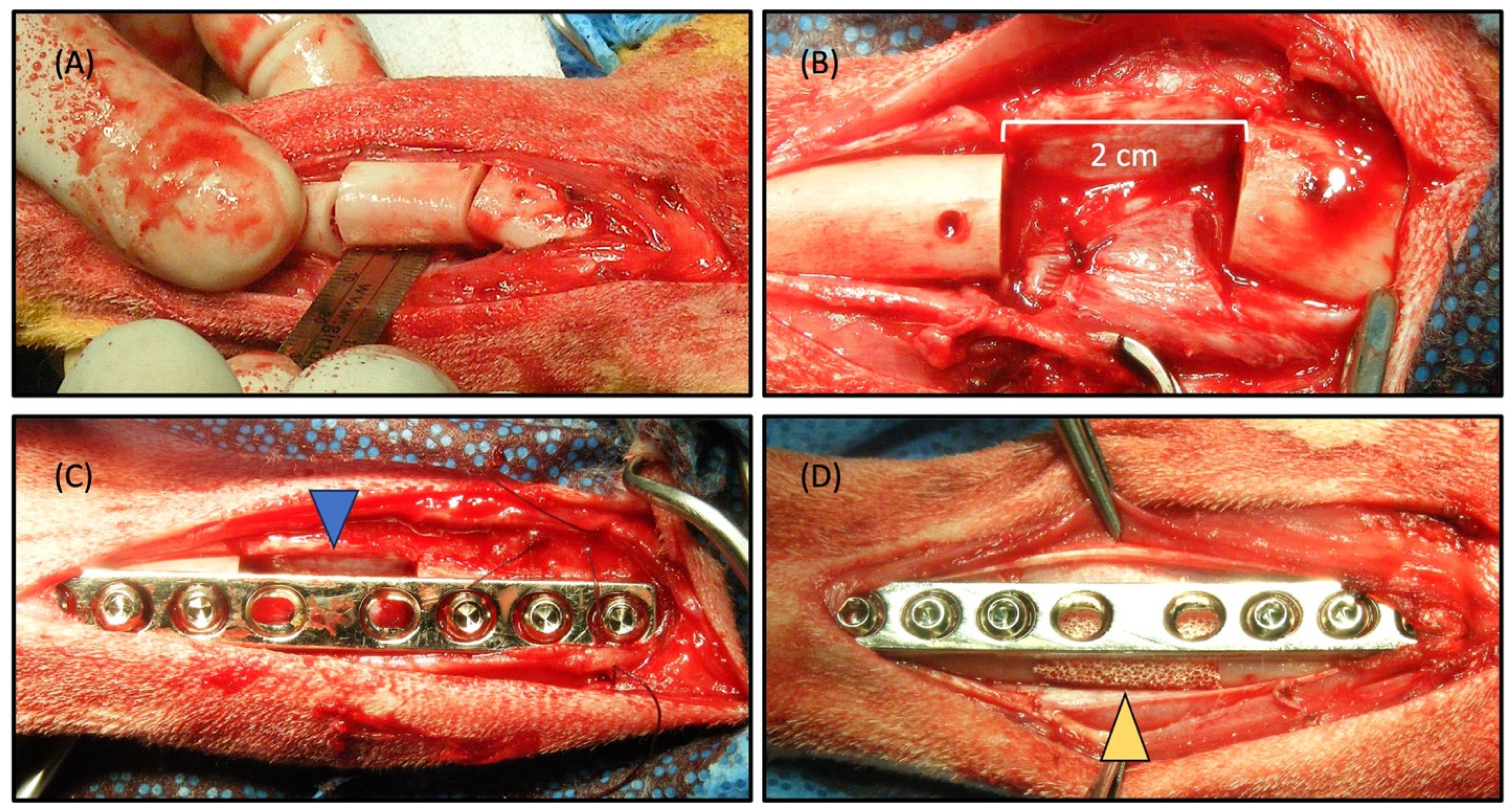
2.2. Surgical Procedure and Radiographic Observation
2.3. Scintigraphic Evaluation
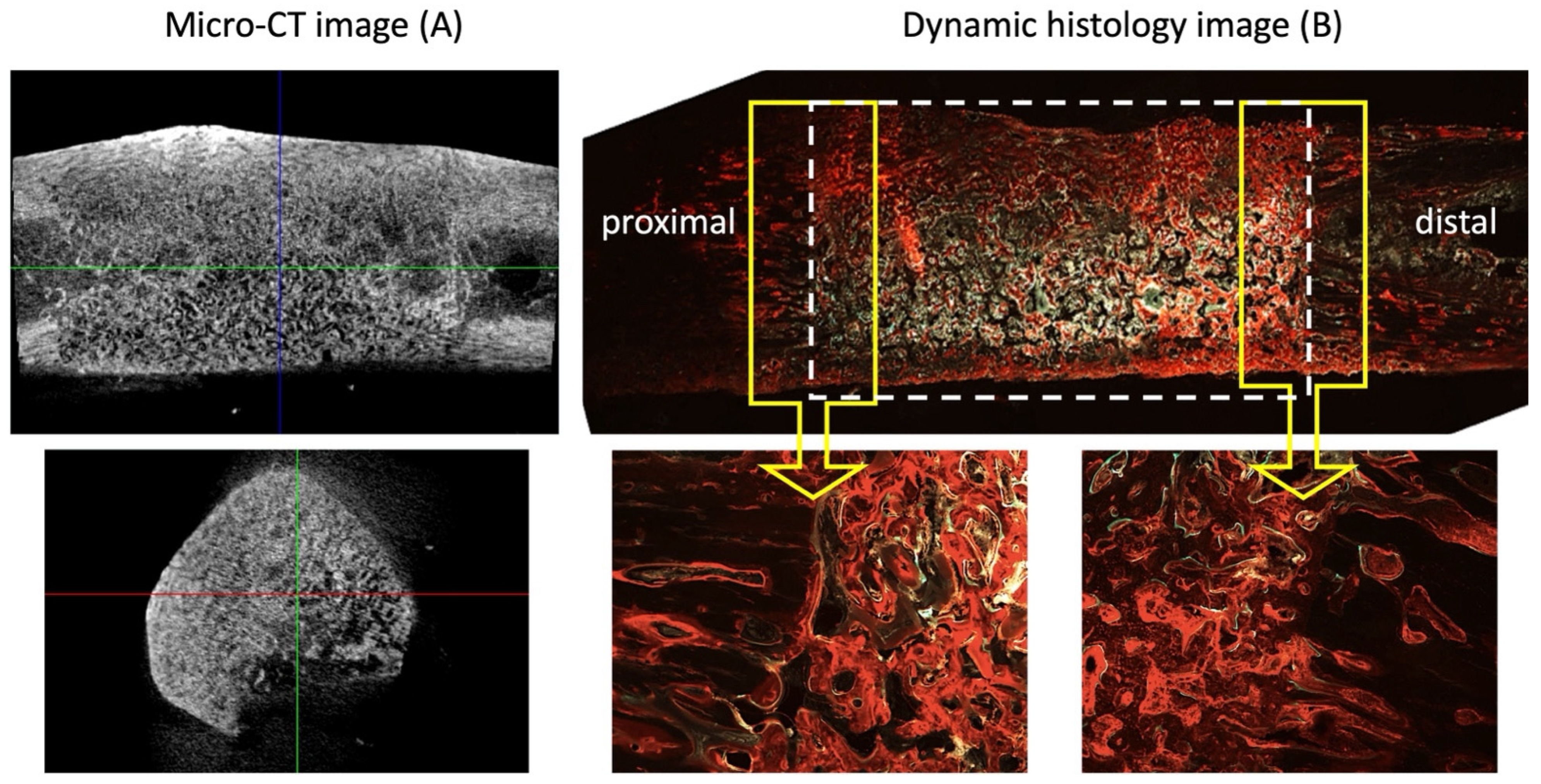
2.4. Micro-CT Evaluation
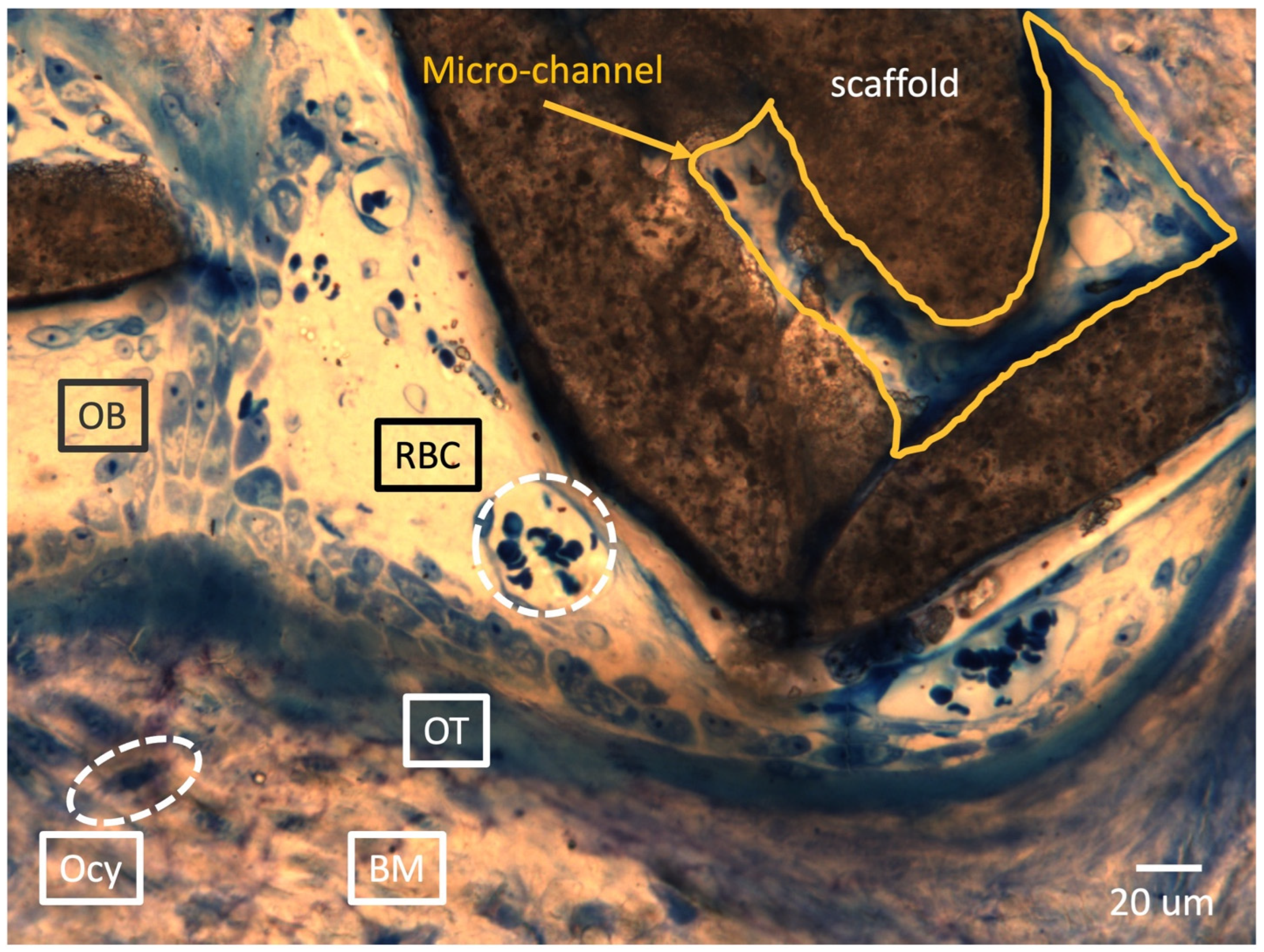
2.5. Histological Analysis
3. Discussion
4. Materials and Methods
4.1. Fabrication and Characterization of Bi-Phasic Scaffold
4.2. Surgical Procedure
4.3. Radiographical Assessment
4.4. Scintigraphic Evaluation
4.5. Micro-CT Evaluation
4.6. Histological Evaluation
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dabezies, E.J.; Stewart, W.E.; Goodman, F.G.; Deffer, P.A. Management of segmental defects of the radius and ulna. J. Trauma 1971, 11, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Grace, T.G.; Eversmann, W.W., Jr. The management of segmental bone loss associated with forearm fractures. J. Bone Jt. Surg. Am. 1980, 62, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Cierny, G., 3rd; Zorn, K.E. Segmental tibial defects. Comparing conventional and Ilizarov methodologies. Clin. Orthop. Relat. Res. 1994, 301, 118–123. [Google Scholar] [PubMed]
- Green, S.A. Skeletal defects. A comparison of bone grafting and bone transport for segmental skeletal defects. Clin. Orthop. Relat. Res. 1994, 301, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Prokuski, L.J.; Marsh, J.L. Segmental bone deficiency after acute trauma. The role of bone transport. Orthop. Clin. N. Am. 1994, 25, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Covey, D.C. Blast and fragment injuries of the musculoskeletal system. J. Bone Jt. Surg. Am. 2002, 84, 1221–1234. [Google Scholar] [CrossRef] [PubMed]
- Calkins, M.S.; Burkhalter, W.; Reyes, F. Traumatic segmental bone defects in the upper extremity. Treatment with exposed grafts of corticocancellous bone. J. Bone Jt. Surg. Am. 1987, 69, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Delloye, C.; Suratwala, S.J.; Cornu, O.; Lee, F.Y. Treatment of allograft nonunions with recombinant human bone morphogenetic proteins (rhBMP). Acta Orthop. Belg. 2004, 70, 591–597. [Google Scholar] [PubMed]
- Starnes, B.W.; Beekley, A.C.; Sebesta, J.A.; Andersen, C.A.; Rush, R.M., Jr. Extremity vascular injuries on the battlefield: Tips for surgeons deploying to war. J. Trauma 2006, 60, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Viateau, V.; Guillemin, G.; Bousson, V.; Oudina, K.; Hannouche, D.; Sedel, L.; Logeart-Avramoglou, D.; Petite, H. Long-bone critical-size defects treated with tissue-engineered grafts: A study on sheep. J. Orthop. Res. 2007, 25, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Namazian, A.; Wilke, F.; Ettinger, M.; Stübig, T.; Brand, S.; Bengel, F.; Krettek, C.; Berding, G.; Jagodzinski, M. Repair of segmental long-bone defects by stem cell concentrate augmented scaffolds: A clinical and positron emission tomography—Computed tomography analysis. Int. Orthop. 2013, 37, 2231–2237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dumic-Cule, I.; Pecina, M.; Jelic, M.; Jankolija, M.; Popek, I.; Grgurevic, L.; Vukicevic, S. Biological aspects of segmental bone defects management. Int. Orthop. 2015, 39, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Moore, W.R.; Graves, S.E.; Bain, G.I. Synthetic bone graft substitutes. ANZ J. Surg. 2001, 71, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Denes, E.; Barrière, G.; Poli, E.; Lévêque, G. Alumina Biocompatibility. J. Long Term Eff. Med. Implants 2018, 28, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.; Mozafari, M. Biocompatibility of alumina-based biomaterials-A review. J. Cell Physiol. 2019, 234, 3321–3335. [Google Scholar] [CrossRef] [PubMed]
- Montilla-Soler, J.L.; Makanji, R. Skeletal Scintigraphy. Cancer Control 2017, 24, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Davila, D.; Antoniou, A.; Chaudhry, M.A. Evaluation of osseous metastasis in bone scintigraphy. Semin. Nucl. Med. 2015, 45, 3–15, Erratum in Semin. Nucl. Med. 2015, 45, 266. [Google Scholar] [CrossRef] [PubMed]
- Smeele, L.E.; Hoekstra, O.S.; Winters, H.A.; Leemans, C.R. Clinical effectiveness of 99mTc-diphosphonate scintigraphy of revascularized iliac crest flaps. Int. J. Oral Maxillofac. Surg. 1996, 25, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lin, H.; Fang, T.; Li, X.; Dai, W.; Uemura, T.; Dong, J. The repair of large segmental bone defects in the rabbit with vascularized tissue engineered bone. Biomaterials 2010, 31, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Chang, Y.H.; Lin, K.J.; Yen, T.C.; Tai, C.L.; Chen, C.Y.; Lo, W.H.; Hsiao, I.T.; Hu, Y.C. The healing of critical-sized femoral segmental bone defects in rabbits using baculovirus-engineered mesenchymal stem cells. Biomaterials 2010, 31, 3222–3230. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Cui, L.; Zhang, W.J.; Liu, W.; Cao, Y. Repair of canine mandibular bone defects with bone marrow stromal cells and porous beta-tricalcium phosphate. Biomaterials 2007, 28, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Chen, X.; Mao, T.; Chen, F.; Feng, X. Bone marrow-derived osteoblasts seeded into porous beta-tricalcium phosphate to repair segmental defect in canine’s mandibula. Ulus Travma Acil Cerrahi Derg. 2006, 12, 268–276. [Google Scholar] [PubMed]
- Blumer, M.J.F. Bone tissue and histological and molecular events during development of the long bones. Ann. Anat. 2021, 235, 151704. [Google Scholar] [CrossRef] [PubMed]
- Reddi, A.H.; Muthukumaran, N.; Ma, S.; Carrington, J.L.; Luyten, F.P.; Paralkar, V.M.; Cunningham, N.S. Initiation of bone development by osteogenin and promotion by growth factors. Connect. Tissue Res. 1989, 20, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Filipowska, J.; Tomaszewski, K.A.; Niedźwiedzki, Ł.; Walocha, J.A.; Niedźwiedzki, T. The role of vasculature in bone development, regeneration and proper systemic functioning. Angiogenesis 2017, 20, 291–302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- García, J.R.; García, A.J. Biomaterial-mediated strategies targeting vascularization for bone repair. Drug Deliv. Transl. Res. 2016, 6, 77–95. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lafage-Proust, M.H.; Prisby, R.; Roche, B.; Vico, L. Bone vascularization and remodeling. Jt. Bone Spine 2010, 77, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Pamu, D. A comprehensive review on electrical properties of hydroxyapatite based ceramic composites. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 101, 539–563. [Google Scholar] [CrossRef] [PubMed]
- Habibovic, P.; Kruyt, M.C.; Juhl, M.V.; Clyens, S.; Martinetti, R.; Dolcini, L.; Theilgaard, N.; van Blitterswijk, C.A. Comparative in vivo study of six hydroxyapatite-based bone graft substitutes. J. Orthop. Res. 2008, 26, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.S.; Koch, A.; Eisig, S.; Kim, S.G.; Kim, Y.H.; Kim, D.G.; Shim, J.H. Distinctive Capillary Action by Micro-channels in Bone-like Templates can Enhance Recruitment of Cells for Restoration of Large Bony Defect. J. Vis. Exp. 2015, 103, 52947. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Appleford, M.R.; Oh, S.; Oh, N.; Ong, J.L. In vivo study on hydroxyapatite scaffolds with trabecular architecture for bone repair. J. Biomed. Mater. Res. A 2009, 89, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, S.; Cao, L.; Zhang, X.; Wang, J.; Liu, C. Facilitated vascularization and enhanced bone regeneration by manipulation hierarchical pore structure of scaffolds. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 110, 110622. [Google Scholar] [CrossRef] [PubMed]
- Ghiron, J.; Volkert, W.A.; Garlich, J.; Holmes, R.A. Determination of lesion to normal bone uptake ratios of skeletal radiopharmaceuticals by QARG (quantitative autoradiography). Int. J. Rad. Appl. Instrum. B 1991, 18, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Ryu, Y.H.; Lee, S.J.; Moon, S.H.; Kim, K.J.; Jin, B.J.; Lee, K.D.; Park, J.K.; Lee, J.W.; Lee, S.J.; et al. Bone Regeneration with 3D-Printed Hybrid Bone Scaffolds in a Canine Radial Bone Defect Model. Tissue Eng. Regen. Med. 2022, 19, 1337–1347. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chae, H.S.; Choi, H.; Park, I.; Moon, Y.S.; Sohn, D.S. Comparative Histomorphometric Analysis of Bone Regeneration According to Bone Graft Type. Int. J. Oral Maxillofac. Implants 2023, 38, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Moghadam, H.G.; Sándor, G.K.; Holmes, H.H.; Clokie, C.M. Histomorphometric evaluation of bone regeneration using allogeneic and alloplastic bone substitutes. J. Oral Maxillofac. Surg. 2004, 62, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Qahash, M.; Susin, C.; Polimeni, G.; Hall, J.; Wikesjö, U.M. Bone healing dynamics at buccal peri-implant sites. Clin. Oral Implants Res. 2008, 19, 166–172. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Weeks after Surgery | ||||
|---|---|---|---|---|---|
| 0 | 2 | 4 | 6 | 8 | |
| Control | 0 | 0 | 0 | 0 | 0.92 ± 0.33 |
| HA/Al scaffold | 0 | 1.33 ± 0.34 | 3.11 ± 0.41 | 4.33 ± 0.54 | 4.91 ± 0.21 |
| Score | Description | ||||
| 0 | No visible new bone formation | ||||
| 1 | Minimal disorganized new bone | ||||
| 2 | Disorganized new bone bridging graft to host at both ends | ||||
| 3 | Organized new bone of cortical density bridging at both ends | ||||
| 4 | Loss of graft–host distinction | ||||
| 5 | Significant new bone and graft remodeling | ||||
| Group | BMD (g/cm3) | BV/TV (%) | BA/BV (mm−1) | Tb.Th (mm) | Tb.N (1/mm) | SMI |
|---|---|---|---|---|---|---|
| Normal Bone | 0.80 ± 0.01 | 52.71 ± 0.02 | 57.06 ± 0.24 | 0.67 ± 0.02 | 1.22 ± 0.11 | −7.03 ± 0.37 |
| HA/Al scaffold | 0.68 ± 0.04 | 51.75 ± 2.21 | 55.43 ± 0.58 | 0.60 ± 0.07 | 0.87 ± 0.17 | −3.47 ± 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haam, D.-W.; Bae, C.-S.; Kim, J.-M.; Hann, S.-Y.; Yim, C.-M.R.; Moon, H.-S.; Oh, D.S. Reconstruction of Segmental Bone Defect in Canine Tibia Model Utilizing Bi-Phasic Scaffold: Pilot Study. Int. J. Mol. Sci. 2024, 25, 4604. https://doi.org/10.3390/ijms25094604
Haam D-W, Bae C-S, Kim J-M, Hann S-Y, Yim C-MR, Moon H-S, Oh DS. Reconstruction of Segmental Bone Defect in Canine Tibia Model Utilizing Bi-Phasic Scaffold: Pilot Study. International Journal of Molecular Sciences. 2024; 25(9):4604. https://doi.org/10.3390/ijms25094604
Chicago/Turabian StyleHaam, Dae-Won, Chun-Sik Bae, Jong-Min Kim, Sung-Yun Hann, Chang-Min Richard Yim, Hong-Seok Moon, and Daniel S. Oh. 2024. "Reconstruction of Segmental Bone Defect in Canine Tibia Model Utilizing Bi-Phasic Scaffold: Pilot Study" International Journal of Molecular Sciences 25, no. 9: 4604. https://doi.org/10.3390/ijms25094604