Advances in Photopletysmography Signal Analysis for Biomedical Applications

 ,
,  and
and
Abstract
:1. Introduction
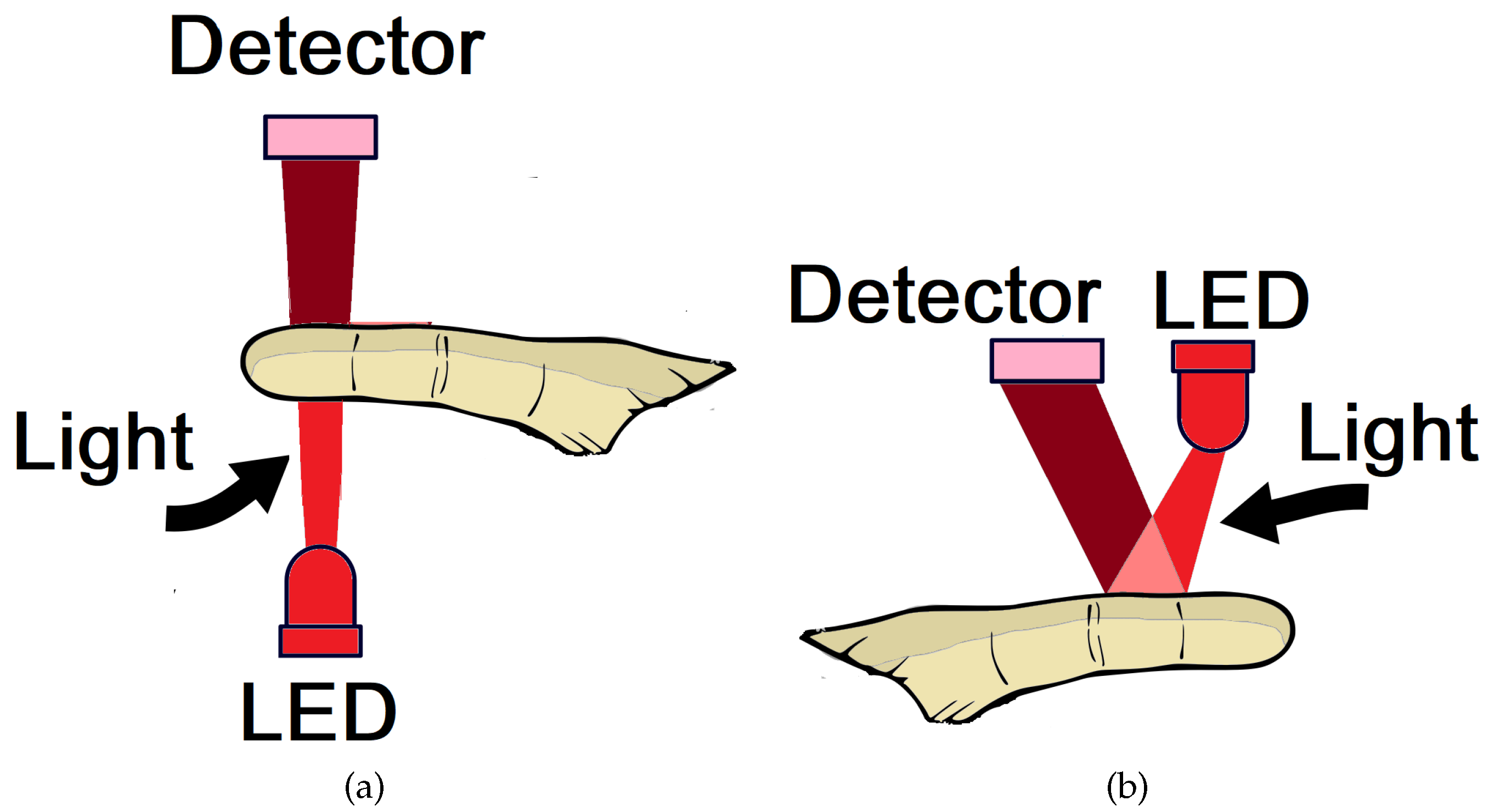
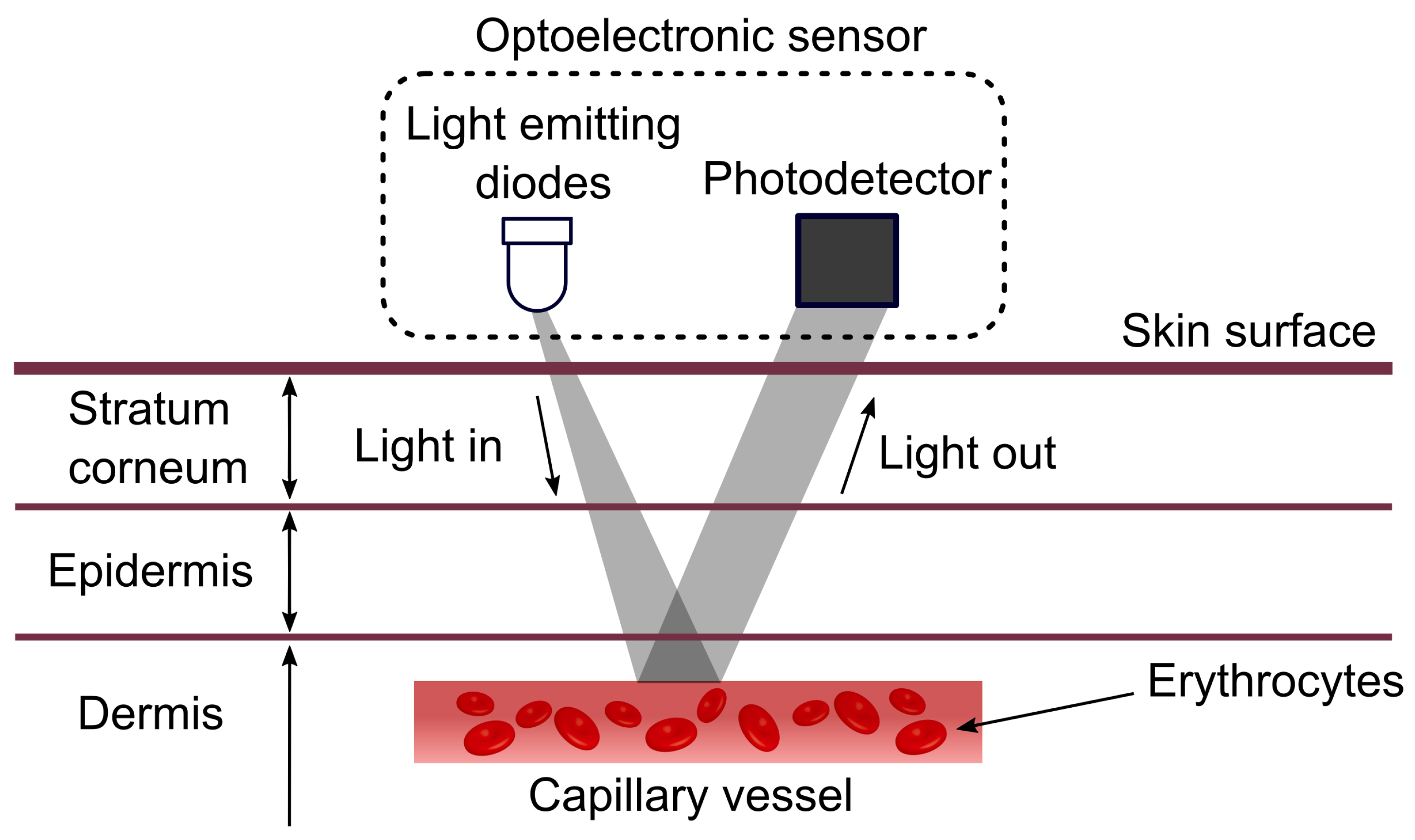
2. Photoplethysmography
- Maximum first derivative: Equals the maximum positive pulse gradient, i.e., the maximum rate of upswing of the pulse wave signal corresponding to the peak velocity of the vessel wall. This is determined numerically from the maximum positive value of the first derivative of the pulse wave.
- Maximum second derivative: Equals the maximum positive rate of change of the gradient, i.e., the maximum acceleration of the vessel wall. This is determined from the calculation of the maximum positive value of the second derivative of the pulse wave.
PPG Sensor
3. Photoplethysmography Signal Processing and Analysis
3.1. Time Domain—Statistical Indicators
- SDNN—standard deviation of all intervals read in a time interval, expressed in ms;
- SDANN—standard deviation of the means of the intervals , every 5 min, in a time interval, expressed in ms;
- SDNNi—the mean of the standard deviation of the intervals every 5 min, expressed in ms;
- rMSSD—the square root of the square mean of the differences between adjacent intervals , in a time interval, expressed in ms; and
- pNN50—the percentage of the adjacent intervals with duration difference greater than 50 ms.
3.2. Time Domain–Geometric Indices
- Triangular index (RRtri);
- Triangular interpolation of RR intervals (TINN); and
- Plot of Poincaré.
- Figure similar to a comet, in which an increase in the scattering of the beat-to-beat intervals is analyzed, characteristic of a normal plot;
- Figure similar to a torpedo, with slight global beat-to-beat scattering (SD1) and without increasing the scattering of long-term beat-to-beat intervals; and
- Parabolic or complex figure, in which two or more distinct ends are separated from the main body of the plot, with at least three points included in each end.
3.3. Frequency Domain
- High frequency (HF) (0.15 to 0.40 Hz), modulated by the parasympathetic nervous system and generated by breathing;
- Low frequency (LF) (0.04 to 0.15 Hz); and
- Very low frequency (VLF) (0.01 to 0.04 Hz), modulated by both the sympathetic nervous system and the parasympathetic nervous system.
- (1)
- The HF component corresponds to the respiratory rhythm and is a vagal modulation marker.
- (2)
- The LF component indicates the sympathetic activities.
- (3)
- The reciprocal relationship between the two characterizes the simpato-vagal balance.
3.4. Nonlinear Methods
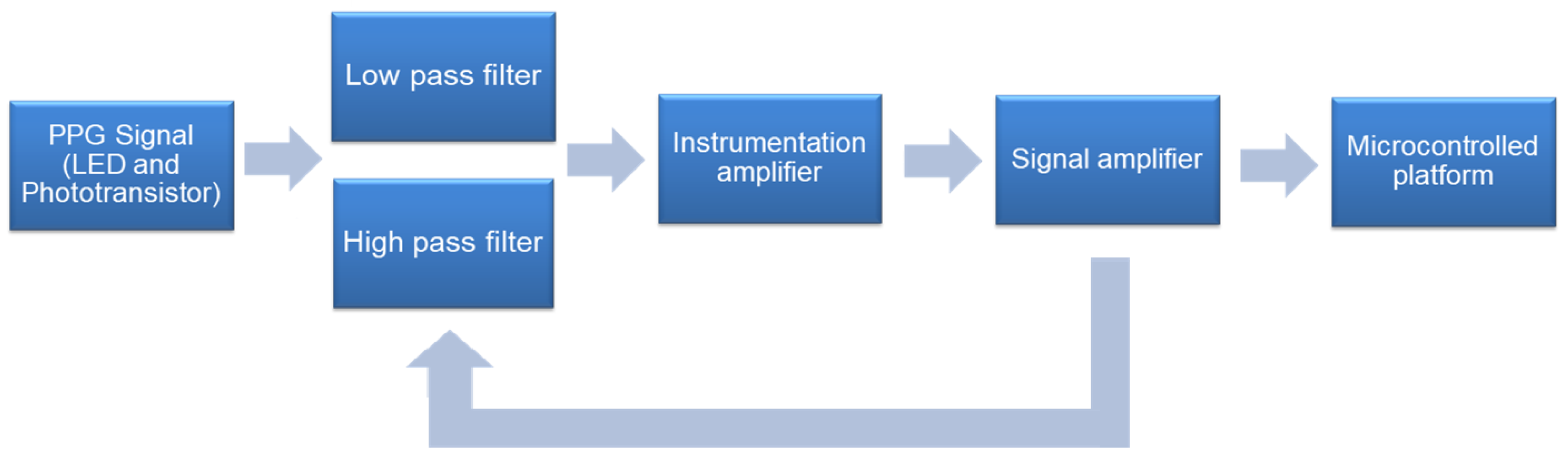
4. Instrumentation
5. Related Work and Clinical Applicability
6. Discussion and Open Issues
7. Learned Lessons
8. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Paschoal, M.; Gonçalves, N.; Petrelluzzi, K.; Machado, R. Controle autonômico cardíaco durante a execução de atividade física dinâmica de baixa intensidade. Rev. Soc. Cardiol. Estado de São Paulo 2003, 13, S1–S11. [Google Scholar]
- Lin, C.H. Assessment of bilateral photoplethysmography for lower limb peripheral vascular occlusive disease using color relation analysis classifier. Comput. Methods Progr. Biomed. 2011, 103, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Faurholt-Jepsen, M.; Kessing, L.V.; Munkholm, K. Heart rate variability in bipolar disorder: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 73, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Palma, J.A.; Benarroch, E.E. Neural control of the heart. Neurology 2014, 83, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Aubert, A.E.; Seps, B.; Beckers, F. Heart rate variability in athletes. Sports Med. 2003, 33, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Florea, V.G.; Cohn, J.N. The Autonomic Nervous System and Heart Failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajendra, A.U.; Paul, J.K.; Natarajan, K.; Min, L.C.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Porto, L.G.G.; Junqueira, L.F., Jr. Comparison of Time-Domain Short-Term Heart Interval Variability Analysis Using a Wrist-Worn Heart Rate Monitor and the Conventional Electrocardiogram. Pacing Clin. Electrophysiol. 2009, 32, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014; p. 298. [Google Scholar]
- De Alexandria, A.R.; Cortez, P.C.; Bessa, J.A.; da Silva Félix, J.H.; de Abreu, J.S.; de Albuquerque, V.H.C. Psnakes: A new radial active contour model and its application in the segmentation of the left ventricle from echocardiographic images. Comput. Methods Progr. Biomed. 2014, 116, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, L.A.F. Sistema não Invasivo de Monitorização da Pressão Arterial e da Onda de Pulso Utilizando a Fotopletismografia. Ph.D. Thesis, Programa de Pós Graduação em Engenharia Biomédica, Universidade Federal do Rio de Janeiro, UFRJ, Rio de Janeiro, Brasil, 2006. [Google Scholar]
- Kilsztajn, S.; Rossbach, A.; Câmara, M.; Carmo, M. Health services, expenses and aging of the Brazilian population. Rev. Bras. Study Popul. 2003, 20, 93–108. [Google Scholar]
- Fan, F.; Yan, Y.; Tang, Y.; Zhang, H. A motion-tolerant approach for monitoring SpO2 and heart rate using photoplethysmography signal with dual frame length processing and multi-classifier fusion. Comput. Biol. Med. 2017, 91, 291–305. [Google Scholar] [CrossRef] [PubMed]
- Birrenkott, D.; Pimentel, M.A.; Watkinson, P.J.; Clifton, D.A. A robust fusion model for estimating respiratory rate from photoplethysmography and electrocardiography. IEEE Trans. Biomed. Eng. 2017. [Google Scholar] [CrossRef]
- Akay, M. Wiley Encyclopedia of Biomedical Engineering; Wiley-Interscience: Hoboken, NJ, USA, 2006; p. 4152. [Google Scholar]
- Papini, G.; Fonseca, P.; Aubert, X.; Overeem, S.; Bergmans, J.; Vullings, R. Photoplethysmography beat detection and pulse morphology quality assessment for signal reliability estimation. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; pp. 117–120. [Google Scholar]
- Da, S.; Luz, E.J.; Nunes, T.M.; de Albuquerque, V.H.C.; Papa, J.P.; Menotti, D. ECG arrhythmia classification based on optimum-path forest. Expert Syst. Appl. 2013, 40, 3561–3573. [Google Scholar]
- De Albuquerque, V.H.C.; Nunes, T.M.; Pereira, D.R.; Luz, E.J.D.S.; Menotti, D.; Papa, J.P.; Tavares, J.M.R.S. Robust automated cardiac arrhythmia detection in ECG beat signals. Neural Comput. Appl. 2018, 29, 679–693. [Google Scholar] [CrossRef]
- Zhao, D.; Sun, Y.; Wan, S.; Wang, F. SFST: A robust framework for heart rate monitoring from photoplethysmography signals during physical activities. Biomed. Signal Process. Control 2017, 33, 316–324. [Google Scholar] [CrossRef]
- Pradhan, N.; Rajan, S.; Adler, A.; Redpath, C. Classification of the quality of wristband-based photoplethysmography signals. In Proceedings of the 2017 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rochester, MN, USA, 7–10 May 2017; pp. 269–274. [Google Scholar]
- Hussein, A.F.; Kumar, A.; Burbano-Fernandez, M.; Ramirez-Gonzalez, G.; Abdulhay, E.; de Albuquerque, V.H.C. An Automated Remote Cloud-Based Heart Rate Variability Monitoring System. IEEE Access 2018. [Google Scholar] [CrossRef]
- Hassan, M.; Malik, A.; Fofi, D.; Saad, N.; Karasfi, B.; Ali, Y.; Meriaudeau, F. Heart rate estimation using facial video: A review. Biomed. Signal Process. Control 2017, 38, 346–360. [Google Scholar] [CrossRef]
- Charlton, P.; Birrenkott, D.A.; Bonnici, T.; Pimentel, M.A.F.; Johnson, A.E.W.; Alastruey, J.; Tarassenko, L.; Watkinson, P.J.; Beale, R.; Clifton, D.A. Breathing Rate Estimation from the Electrocardiogram and Photoplethysmogram: A Review. IEEE Rev. Biomed. Eng. 2018. [Google Scholar] [CrossRef]
- Alian, A.A.; Shelley, K.H. Photoplethysmography. Best Pract. Res. Clin. Anaesthesiol. 2014, 28, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Thakor, N. Photoplethysmography Revisited: From Contact to Noncontact, From Point to Imaging. IEEE Trans. Biomed. Eng. 2016, 63, 463–477. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, G.; Garfinkel, S.N.; Praag, C.D.G.V.; Sahota, K.; Betka, S.; Critchley, H.D. Feedback from the heart: Emotional learning and memory is controlled by cardiac cycle, interoceptive accuracy and personality. Biol. Psychol. 2017, 126, 19–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, K.A.S.; Pereira, M.H.R.; Pádua, F.L.C. Detecção em tempo real da frequência cardíaca de pessoas por meio da análise de variações temporais em vídeos. E-xacta 2016, 9, 49–62. [Google Scholar] [CrossRef]
- Choi, S.; Min, K.; Kim, N.N.; Munarriz, R.; Goldstein, I.; Traish, A.M. Laser Oximetry: A Novel Noninvasive Method to Determine Changes in Penile Hemodynamics in an Anesthetized Rabbit Model. J. Androl. 2002, 23, 278–283. [Google Scholar] [PubMed]
- Schwarz, L. Proposta de um Sistema Telemétrico Para Aquisição de Sinais Fisiológicos. Ph.D. Thesis, Programa de Pós-Graduação em Engenharia Elétrica, Universidade Federal de Santa Catarina, UFSC, Santa Catarina, Brasil, 2007. [Google Scholar]
- Peter, L.; Vorek, I.; Massot, B.; Bryjova, I.; Urbanczyk, T. Determination of Blood Vessels Expandability; Multichannel Photoplethysmography. IFAC–PapersOnLine 2016, 49, 284–288. [Google Scholar] [CrossRef]
- Madhavan, G. Plethysmography. Biomed. Instrum. Technol. 2005, 39, 367–371. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed]
- Fan, Q.; Li, K. Non-contact remote estimation of cardiovascular parameters. Biomed. Signal Process. Control 2018, 40, 192–203. [Google Scholar] [CrossRef]
- Bhattacharya, J.; Kanjilal, P.; Muralidhar, V. Analysis and characterization of photo-plethysmographic signal. IEEE Trans. Biomed. Eng. 2001, 48, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Meredith, D.; Clifton, D.; Charlton, P.; Brooks, J.; Pugh, C.; Tarassenko, L. Photoplethysmographic derivation of respiratory rate: A review of relevant physiology. J. Med. Eng. Technol. 2012, 36, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moyle, J.T.B. Pulse Oximetry, 2nd ed.; BMJ: London, UK, 2002. [Google Scholar]
- Hejjel, L.; Gál, I. Heart rate variability analysis. Acta Physiologica Hungarica 2001, 88, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Hemon, M.C.; Phillips, J.P. Comparison of foot finding methods for deriving instantaneous pulse rates from photoplethysmographic signals. J. Clin. Monit. Comput. 2016, 30, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.P.; Kyriacou, P.A. Comparison of methods for determining pulse arrival time from Doppler and photoplethysmography signals. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Chicago, IL, USA, 26–30 August 2014; pp. 3809–3812. [Google Scholar]
- Millasseau, S.C.; Stewart, A.D.; Patel, S.J.; Redwood, S.R.; Chowienczyk, P.J. Evaluation of Carotid-Femoral Pulse Wave Velocity. Hypertension 2005, 45, 222–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardoulis, O.; Papaioannou, T.G.; Stergiopulos, N. Validation of a novel and existing algorithms for the estimation of pulse transit time: Advancing the accuracy in pulse wave velocity measurement. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, H1558–H1567. [Google Scholar] [CrossRef] [PubMed]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Hennig, A.; Patzak, A. Continuous blood pressure measurement using pulse transit time. Somnol. Schlafforschung Schlafmed. 2013, 17, 104–110. [Google Scholar] [CrossRef]
- Zheng, Y.L.; Yan, B.P.; Zhang, Y.T.; Poon, C.C.Y. An Armband Wearable Device for Overnight and Cuff-Less Blood Pressure Measurement. IEEE Trans. Biomed. Eng. 2014, 61, 2179–2186. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Zhang, Q.; Ko, S. Noninvasive cuffless blood pressure estimation using pulse transit time and Hilbert–Huang transform. Comput. Electr. Eng. 2013, 39, 103–111. [Google Scholar] [CrossRef]
- Yang, C.; Tavassolian, N. Pulse transit time measurement using seismocardiogram, photoplethysmogram, and acoustic recordings: Evaluation and comparison. IEEE J. Biomed. Health Inf. 2017, 22, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Mukkamala, R.; Hahn, J.O. Toward Ubiquitous Blood Pressure Monitoring via Pulse Transit Time: Predictions on Maximum Calibration Period and Acceptable Error Limits. IEEE Trans. Biomed. Eng. 2018, 65, 1410–1420. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.I.; Struthers, A.D. Pulse wave analysis and pulse wave velocity: A critical review of their strengths and weaknesses. J. Hypertens. 2003, 21, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Nabeel, P.M.; Jayaraj, J.; Mohanasankar, S. Single-source PPG-based local pulse wave velocity measurement: a potential cuffless blood pressure estimation technique. Physiol. Meas. 2017, 12, 2122–2140. [Google Scholar] [CrossRef] [PubMed]
- Borik, S.; Cap, I. Measurement and Analysis Possibilities of Pulse Wave Signals. Adv. Electr. Electron. Eng. 2013, 11. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2571. [Google Scholar] [CrossRef] [PubMed]
- Alvim, R.D.O.; Santos, P.C.J.L.; Bortolotto, L.A.; Mill, J.A.G.; Pereira, A.D.C. Arterial Stiffness: Pathophysiological and Genetic Aspects. Int. J. Cardiovasc. Sci. 2017, 30, 433–441. [Google Scholar] [CrossRef]
- Pereira, T.; Maldonado, J.; Pereira, L.; Conde, J. Aortic stiffness is an independent predictor of stroke in hypertensive patients. Arq. Bras. Cardiol. 2013, 100, 437–443. [Google Scholar] [CrossRef] [PubMed]
- McCombie, D.B.; Reisner, A.T.; Asada, H.H. Adaptive blood pressure estimation from wearable PPG sensors using peripheral artery pulse wave velocity measurements and multi-channel blind identification of local arterial dynamics. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 3521–3524. [Google Scholar]
- Gil, E.; Orini, M.; Bailón, R.; Vergara, J.M.; Mainardi, L.; Laguna, P. Photoplethysmography pulse rate variability as a surrogate measurement of heart rate variability during non-stationary conditions. Physiol. Meas. 2010, 31, 1271. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.T.; Zhang, Y. Spectral analysis of pulse transit time variability and its coherence with other cardiovascular variabilities. In Proceedings of the 28th 2006 EMBS’06 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 6442–6445. [Google Scholar]
- Boulnois, J.L. Photophysical processes in recent medical laser developments: A review. Lasers Med. Sci. 1986, 1, 47–66. [Google Scholar] [CrossRef]
- Martins, R.M.S. Fotopletismografia para Monitorização Cardíaca para aplicação no Pulso. Master’s Thesis, Universidade de Coimbra, Coimbra, Portugal, 2010; 114p. [Google Scholar]
- Gubbi, S.; Amrutur, B. Adaptive Pulse Width Control and Sampling for Low Power Pulse Oximetry. IEEE Trans. Biomed. Circuits Syst. 2015, 9, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Chung, H.; Ko, H.; Lee, J. Wearable Multichannel Photoplethysmography Framework for Heart Rate Monitoring During Intensive Exercise. IEEE Sens. J. 2018, 18, 2983–2993. [Google Scholar] [CrossRef]
- Haahr, R.; Duun, S.; Toft, M.; Belhage, B.; Larsen, J.; Birkelund, K.; Thomsen, E. An Electronic Patch for Wearable Health Monitoring by Reflectance Pulse Oximetry. IEEE Trans. Biomed. Circuits Syst. 2012, 6, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.Z.; Zheng, Y.P. Home-Telecare of the elderly living alone using an new designed ear-wearable sensor. In Proceedings of the 2008 5th International Summer School and Symposium on Medical Devices and Biosensors, Hong Kong, China, 1–3 June 2008; pp. 71–74. [Google Scholar]
- Rhee, S.; Yang, B.H.; Asada, H. Artifact-resistant power-efficient design of finger-ring plethysmographic sensors. IEEE Trans. Biomed. Eng. 2001, 48, 795–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosero, G.; Fernando, O. Sistema móvel de Monitoramento E Treinamento Para Ciclista com Smartphone Android. Master’s Thesis, Engenharia de Sistemas Eletrônicos e de Automação, Universidade de Brasília, Brasília, Brasil, 2012. [Google Scholar]
- Allen, J.; Murray, A. Similarity in bilateral photoplethysmographic peripheral pulse wave characteristics at the ears, thumbs and toes. Physiol. Meas. 2000, 21, 369. [Google Scholar] [CrossRef] [PubMed]
- Shelley, K.H.; Tamai, D.; Jablonka, D.; Gesquiere, M.; Stout, R.G.; Silverman, D.G. The Effect of Venous Pulsation on the Forehead Pulse Oximeter Wave Form as a Possible Source of Error in SpO2 Calculation. Anesth. Analg. 2005, 100, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, Y.; Duckworth, R.; Comtois, G. A Wearable Reflectance Pulse Oximeter for Remote Physiological Monitoring. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 912–915. [Google Scholar]
- Shin, K.; Kim, Y.; Bae, S.; Park, K.; Kim, S. A Novel Headset with a Transmissive PPG Sensor for Heart Rate Measurement. In Proceedings of the 13th International Conference on Biomedical Engineering, Singapore, 3–6 December 2008; Lim, C.T., Goh, J.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 519–522. [Google Scholar]
- Paul, B.; Manuel, M.; Alex, Z. Design and development of non invasive glucose measurement system. In Proceedings of the 2012 1st International Symposium on Physics and Technology of Sensors (ISPTS-1), Pune, India, 7–10 March 2012; pp. 43–46. [Google Scholar]
- Karlen, W.; Raman, S.; Ansermino, J.; Dumont, G. Multiparameter Respiratory Rate Estimation from the Photoplethysmogram. IEEE Trans. Biomed. Eng. 2013, 60, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.O. Infraestrutura De Hardware E Software Para Monitoramento De Batimentos Cardíacos Em Bovinos De Corte; Trabalho de Conclusão de Curso em Engenharia Elétrica; Universidade Federal do Mato Grosso do Sul, FAENG, Campo Grande: Vila Olinda, Brasil, 2014. [Google Scholar]
- Vanderlei, L.C.M.; Pastre, C.M.; Hoshi, R.A.; Carvalho, T.D.D.; Godoy, M.F.D. Basic notions of heart rate variability and its clinical applicability. Braz. J. Cardiovasc. Surg. 2009, 24, 205–217. [Google Scholar] [CrossRef]
- Javorka, M.; Zila, I.; Balhãrek, T.; Javorka, K. Heart rate recovery after exercise: Relations to heart rate variability and complexity. Braz. J. Med. Biol. Res. 2002, 35, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Sandercock, G.R.; Brodie, D.A. A Quantitative Systematic Review of Normal Values for Short-Term Heart Rate Variability in Healthy Adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Task, F. Force of the European Society of Cardiology, Heart rate variability, standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Pumprla, J.; Howorka, K.; Groves, D.; Chester, M.; Nolan, J. Functional assessment of heart rate variability: Physiological basis and practical applications. Int. J. Cardiol. 2002, 84, 1–14. [Google Scholar] [CrossRef]
- Hirfanoglu, T.; Serdaroglu, A.; Cetin, I.; Kurt, G.; Capraz, I.Y.; Ekici, F.; Arhan, E.; Bilir, E. Effects of vagus nerve stimulation on heart rate variability in children with epilepsy. Epilepsy Behav. 2018, 81, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Khaled, A.; Owis, M.; Mohamed, S.A.A. Employing Time-Domain Methods and Poincaré Plot of Heart Rate Variability Signals to Detect Congestive Heart Failure. BIME J. 2006, 6, 35–41. [Google Scholar]
- De Carvalho, T.D.; Pastre, C.M.; Rossi, R.C.; de Abreu, L.; Valenti, V.; Vanderlei, L.M. Índices geométricos de variabilidade da frequência cardíaca na doença pulmonar obstrutiva crônica. Rev. Port. Pneumol. 2011, 17, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.L.; Reynolds, K.J.; Owen, H. Correlated Poincaré indices for measuring heart rate variability. Australas. Phys. Eng. Sci. Med. 2007, 30, 336. [Google Scholar] [PubMed]
- Lam, J.C.; Yan, C.S.; Lai, A.Y.; Tam, S.; Fong, D.Y.; Lam, B.; Ip, M.S. Determinants of Daytime Blood Pressure in Relation to Obstructive Sleep Apnea in Men. Lung 2009, 187, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Tulppo, M.P.; Mäkikallio, T.H.; Seppänen, T.; Laukkanen, R.T.; Huikuri, H.V. Vagal modulation of heart rate during exercise: Effects of age and physical fitness. Am. J. Physiol. Heart Circ. Physiol. 1998, 274, H424–H429. [Google Scholar] [CrossRef]
- Sarén-Koivuniemi, T.J.; Yli-Hankala, A.M.; van Gils, M.J. Increased variation of the response index of nociception during noxious stimulation in patients during general anaesthesia. Comput. Methods Progr. Biomed. 2011, 104, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Gamelin, F.X.; Berthoin, S.; Bosquet, L. Validity of the polar S810 heart rate monitor to measure RR intervals at rest. Med. Sci. Sports Exerc. 2006, 38, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Shields Robert, W. Heart rate variability with deep breathing as a clinical test of cardiovagal function. Cleve. Clin. J. Med. 2009, 76, S37–40. [Google Scholar] [CrossRef] [PubMed]
- Akselrod, S.; Gordon, D.; Ubel, F.; Shannon, D.; Berger, A.; Cohen, R. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M.; Fletcher, R.R.; Norton, I.; Brearley, M.; Abbott, D.; Lovell, N.H.; Schuurmans, D. Frequency analysis of photoplethysmogram and its derivatives. Comput. Methods Progr. Biomed. 2015, 122, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M. Standard Terminologies for Photoplethysmogram Signals. Curr. Cardiol. Rev. 2012, 8, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P. Nonlinear systems in medicine. Yale J. Biol. Med. 2002, 75, 247. [Google Scholar] [PubMed]
- Niskanen, J.P.; Tarvainen, M.P.; Ranta-aho, P.O.; Karjalainen, P.A. Software for advanced HRV analysis. Comput. Methods Progr. Biomed. 2004, 76, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puri, C.; Ukil, A.; Bandyopadhyay, S.; Singh, R.; Pal, A.; Mandana, K. iCarMa: Inexpensive Cardiac Arrhythmia Management–An IoT Healthcare Analytics Solution. In Proceedings of the First IoT of Health ’16 Workshop on IoT-enabled Healthcare and Wellness Technologies and Systems, Singapore, 25–30 June 2016; ACM: New York, NY, USA, 2016; pp. 3–8. [Google Scholar]
- Karegar, F.P.; Fallah, A.; Rashidi, S. ECG based human authentication with using Generalized Hurst Exponent. In Proceedings of the 2017 Iranian Conference on Electrical Engineering (ICEE), Tehran, Iran, 2–4 May 2017; pp. 34–38. [Google Scholar]
- Pham, T.D.; Oyama-Higa, M. Photoplethysmography technology and its feature visualization for cognitive stimulation assessment. In Proceedings of the 2015 IEEE International Conference on Industrial Technology (ICIT), Seville, Spain, 17–19 March 2015; pp. 1735–1740. [Google Scholar]
- Horio, K.; Li, Y. Visualization and Analysis of Mental States Based on Photoplethysmogram. In Proceedings of the 2009 Fourth International Conference on Innovative Computing, Information and Control (ICICIC), Kaohsiung, Taiwan, 7–9 December 2009; pp. 1401–1404. [Google Scholar]
- Lee, J.; Jung, W.; Kang, I.; Kim, Y.; Lee, G. Design of filter to reject motion artifact of pulse oximetry. Comput. Stand. Interfaces 2004, 26, 241–249. [Google Scholar] [CrossRef]
- Lee, H.W.; Lee, J.W.; Jung, W.G.; Lee, G.K. The periodic moving average filter for removing motion artifacts from PPG signals. Int. J. Control Autom. Syst. 2007, 5, 701–706. [Google Scholar]
- Ruiz, L.M.; Manzo, A.; Casimiro, E.; Cárdenas, E.; González, R. Heart rate variability using photoplethysmography with green wavelength. In Proceedings of the 2014 IEEE International Autumn Meeting on Power, Electronics and Computing (ROPEC), Ixtapa, Mexico, 5–7 Noember 2014; pp. 1–5. [Google Scholar]
- Manonelles Rincón, L. Development of an Acquisition Circuit of Multiple Biological Signals for Integration into a Wearable Bracelet. Bachelor’s Thesis, Universitat Politècnica de Catalunya, Barcelona, Spain, 2017. [Google Scholar]
- Kukkapalli, R. Non-Invasive Wearable Sensors for Respiration Monitoring. Bachelor’s Thesis, University of Maryland, Baltimore County, Baltimore, MD, USA, 2016. [Google Scholar]
- Asada, H.; Reisner, A.; Shaltis, P.; McCombie, D. Towards the Development of Wearable Blood Pressure Sensors: A Photo-Plethysmograph Approach Using Conducting Polymer Actuators. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2005; pp. 4156–4159. [Google Scholar]
- Baheti, P.K.; Garudadri, H. An Ultra Low Power Pulse Oximeter Sensor Based on Compressed Sensing. In Proceedings of the 2009 Sixth International Workshop on Wearable and Implantable Body Sensor Networks, Berkeley, CA, USA, 3–5 June 2009; pp. 144–148. [Google Scholar]
- Wang, L.; Lo, B.P.; Yang, G.Z. Multichannel Reflective PPG Earpiece Sensor With Passive Motion Cancellation. IEEE Trans. Biomed. Circuits Syst. 2007, 1, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.; Liu, S. An ultra-low power, self-organizing wireless network and non-invasive biomedical instrumentation. In Proceedings of the Second Joint 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society, Engineering in Medicine and Biology, Houston, TX, USA, 23–26 October 2002; Volume 3, pp. 1803–1804. [Google Scholar]
- Guyton, A.; Hall, J. Renal regulation of potassium, calcium, phosphate, and magnesium; integration of renal mechanisms for control of blood volume and extracellular fluid volume. Guyton Hall Textb. Med. Physiol. 2006, 10, 371–373. [Google Scholar]
- Silva, M.D.C. Monitoramento Remoto Preventivo de Pacientes Com Doenças Cardiovasculares Utilizando Dispositivo Móvel Como Agente Inteligente. Ph.D. Thesis, Programa de Pós-Graduação em Informática, Universidade Federal da Paraíba, UFPB, João Pessoa, Brasil, 2012. [Google Scholar]
- Pantoni, C.; Reis, M.; Martins, L.; Catai, A.; Costa, D.; Borghi-Silva, A. Study of heart rate autonomic modulation at rest in elderly patients with chronic obstructive pulmonary disease. Braz. J. Phys. Ther. 2007, 11, 35–41. [Google Scholar]
- Pickett, J.; Amoroso, P.; Nield, D.; Jones, D. Pulse oximetry and PPG measurements in plastic surgery. Engineering in Medicine and Biology Society, 1997. In Proceedings of the 19th Annual International Conference of the IEEE, Chicago, IL, USA, 30 October–2 November 1997; Volume 5, pp. 2330–2332. [Google Scholar]
- Allen, J.; Oates, C.P.; Lees, T.A.; Murray, A. Photoplethysmography detection of lower limb peripheral arterial occlusive disease: A comparison of pulse timing, amplitude and shape characteristics. Physiol. Meas. 2005, 26, 811. [Google Scholar] [CrossRef] [PubMed]
- Custódio Rubira, M.; Angelis Rubira, A.P.F.D.; Silva Soares, P.P.D.; Gusmão Medeiros, L.; Alves Neves, G.; Consolim-Colombo, F.M. Cardiovascular risk in eutrophic young subjects: Influence of corporal fat and sympathetic activity. ConSci. Saúde 2011, 10, 223–230. [Google Scholar]
- Amir, O.; Barak-Shinar, D.; Henry, A.; Smart, F.W. Photoplethysmography as a single source for analysis of sleep-disordered breathing in patients with severe cardiovascular disease. J. Sleep Res. 2012, 21, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Melillo, P.; Fusco, R.; Sansone, M.; Bracale, M.; Pecchia, L. Discrimination power of long-term heart rate variability measures for chronic heart failure detection. Med. Biol. Eng. Comput. 2011, 49, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnethon, M.R.; Liao, D.; Evans, G.W.; Cascio, W.E.; Chambless, L.E.; Heiss, G. Correlates of the shift in heart rate variability with an active postural change in a healthy population sample: The Atherosclerosis Risk In Communities study. Am. Heart J. 2002, 143, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Naydenova, E.; Tsanas, A.; Casals-Pascual, C.; Vos, M.D. Smart diagnostic algorithms for automated detection of childhood pneumonia in resource-constrained settings. In Proceedings of the 2015 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 8–11 October 2015; pp. 377–384. [Google Scholar]
- Karlen, W.; Brouse, C.; Cooke, E.; Ansermino, J.; Dumont, G. Respiratory rate estimation using respiratory sinus arrhythmia from photoplethysmography. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 1201–1204. [Google Scholar]
- Furuland, H.; Linde, T.; Englund, A.; Wikström, B. Heart rate variability is decreased in chronic kidney disease but may improve with hemoglobin normalization. J. Nephrol. 2008, 21, 45–52. [Google Scholar] [PubMed]
- Sommermeyer, D.; Zou, D.; Ficker, J.H.; Randerath, W.; Fischer, C.; Penzel, T.; Sanner, B.; Hedner, J.; Grote, L. Detection of cardiovascular risk from a photoplethysmographic signal using a matching pursuit algorithm. Med. Biol. Eng. Comput. 2016, 54, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, D.M. Diseño De Un Dispositivo Para La Detección Del Estrés A Partir De La Señal De Fotopletismografía. Trabajo Fin de G, Escuela Técnica Superior De Ingeniería Grado En Ingeniería De Las Tecnologías De Telecomunicación, Sevilla. 2014. Available online: http://bibing.us.es/proyectos/abreproy/90024/ (accessed on 08 June 2018).
- Vilhegas, L.Z. Development of a Prototype for Monitoring Oxygen Saturation and Heart Rate for Rodents. Master’s Thesis, Título de Engenharia Elétrica, Escola Politécnica, São Paulo, Brasil, 2007. [Google Scholar]
- Hickey, M.; Samuels, N.; Randive, N.; Langford, R.; Kyriacou, P. A new fibre optic pulse oximeter probe for monitoring splanchnic organ arterial blood oxygen saturation. Comput. Methods Progr. Biomed. 2012, 108, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Zhao, H.; Dou, S. A new signal decomposition to estimate breathing rate and heart rate from photoplethysmography signal. Biomed. Signal Process. Control 2015, 19, 89–95. [Google Scholar] [CrossRef]
- Jovanov, E.; Nallathimmareddygari, V.; Pryor, J. SmartStuff: A case study of a smart water bottle. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 6307–6310. [Google Scholar]
- Da Cruz, M.A.A.; Rodrigues, J.J.P.C.; Al-Muhtadi, J.; Korotaev, V.V.; de Albuquerque, V.H.C. A Reference Model for Internet of Things Middleware. IEEE Internet Things J. 2018, 5, 871–883. [Google Scholar] [CrossRef]
- Rodrigues, J.J.P.C.; Segundo, D.B.D.R.; Junqueira, H.A.; Sabino, M.H.; Prince, R.M.; Al-Muhtadi, J.; Albuquerque, V.H.C.D. Enabling Technologies for the Internet of Health Things. IEEE Access 2018, 6, 13129–13141. [Google Scholar] [CrossRef]
- Lakshmanaprabu, S.K.; Shankar, K.; Khanna, A.; Gupta, D.; Rodrigues, J.J.P.C.; Pinheiro, P.R.; Albuquerque, V.H.C.D. Effective Features to Classify Big Data Using Social Internet of Things. IEEE Access 2018, 6, 24196–24204. [Google Scholar] [CrossRef]
- Rodrigues, J.; Segundo, D.; Junqueira, H.; Sabino, M.; Prince, R.; Al-Muhtadi, J.; de Albuquerque, V. Enabling Technologies for the Internet of Health Things. IEEE Access 2018, 6, 13129–13141. [Google Scholar] [CrossRef]
- Woo, M.W.; Lee, J.; Park, K. A reliable IoT system for Personal Healthcare Devices. Future Gener. Comput. Syst. 2018, 78, 626–640. [Google Scholar] [CrossRef]
- Farahani, B.; Firouzi, F.; Chang, V.; Badaroglu, M.; Constant, N.; Mankodiya, K. Towards fog-driven IoT eHealth: Promises and challenges of IoT in medicine and healthcare. Future Gener. Comput. Syst. 2018, 78, 659–676. [Google Scholar] [CrossRef]
- Islam, S.; Kwak, D.; Kabir, M.; Hossain, M.; Kwak, K. The Internet of Things for Health Care: A Comprehensive Survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Constant, N.; Douglas-Prawl, O.; Johnson, S.; Mankodiya, K. Pulse-Glasses: An unobtrusive, wearable HR monitor with Internet-of-Things functionality. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–5. [Google Scholar]
- Wannenburg, J.; Malekian, R. Body Sensor Network for Mobile Health Monitoring, a Diagnosis and Anticipating System. IEEE Sens. J. 2015, 15, 6839–6852. [Google Scholar] [CrossRef]
- Bobbia, S.; Macwan, R.; Benezeth, Y.; Mansouri, A.; Dubois, J. Unsupervised skin tissue segmentation for remote photoplethysmography. Pattern Recognit. Lett. 2017. [Google Scholar] [CrossRef]
- Wijshoff, R.; Mischi, M.; Aarts, R. Reduction of Periodic Motion Artifacts in Photoplethysmography. IEEE Trans. Biomed. Eng. 2017, 64, 196–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Memon, S.F.; Newe, T.; Lewis, E.; Leen, G. Motion artefact minimization from photoplethysmography based non-invasive hemoglobin sensor based on an envelope filtering algorithm. Measurement 2018, 115, 288–298. [Google Scholar] [CrossRef]
- Ram, M.R.; Madhav, K.V.; Krishna, E.H.; Komalla, N.R.; Reddy, K.A. A novel approach for motion artifact reduction in PPG signals based on AS-LMS adaptive filter. IEEE Trans. Instrum. Meas. 2012, 61, 1445–1457. [Google Scholar] [CrossRef]
- Relente, A.; Sison, L. Characterization and adaptive filtering of motion artifacts in pulse oximetry using accelerometers. In Proceedings of the Second Joint IEEE 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society EMBS/BMES Conference, Engineering in Medicine and Biology, Houston, TX, USA, 23–26 October 2002; Volume 2, pp. 1769–1770. [Google Scholar]
- Chan, K.; Zhang, Y. Adaptive reduction of motion artifact from photoplethysmographic recordings using a variable step-size LMS filter. In Proceedings of the IEEE Sensors, Orlando, FL, USA, 12–14 June 2002; Volume 2, pp. 1343–1346. [Google Scholar]
- Lee, C.; Zhang, Y.T. Reduction of motion artifacts from photoplethysmographic recordings using a wavelet denoising approach. In Proceedings of the 2003 IEEE EMBS Asian-Pacific Conference on Biomedical Engineering, IEEE, Kyoto, Japan, 20–22 October 2003; pp. 194–195. [Google Scholar]
- Raghuram, M.; Madhav, K.V.; Krishna, E.H.; Reddy, K.A. Evaluation of wavelets for reduction of motion artifacts in photoplethysmographic signals. In Proceedings of the 10th International Conference on Information Science, Signal Processing and their Applications (ISSPA 2010), Kuala Lumpur, Malaysia, 10–13 May 2010; pp. 460–463. [Google Scholar]
- Alfaouri, M.; Daqrouq, K. ECG signal denoising by wavelet transform thresholding. Am. J. Appl. Sci. 2008, 5, 276–281. [Google Scholar] [CrossRef]
- Coetzee, F.M.; Elghazzawi, Z. Noise-resistant pulse oximetry using a synthetic reference signal. IEEE Trans. Biomed. Eng. 2000, 47, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Cvetkovic, D.; Übeyli, E.D.; Cosic, I. Wavelet transform feature extraction from human PPG, ECG, and EEG signal responses to ELF PEMF exposures: A pilot study. Digit. Signal Process. 2008, 18, 861–874. [Google Scholar] [CrossRef]
- Raghuram, M.; Madhav, K.V.; Krishna, E.H.; Komalla, N.R.; Sivani, K.; Reddy, K.A. Dual-tree complex wavelet transform for motion artifact reduction of PPG signals. In Proceedings of the 2012 IEEE International Symposium on Medical Measurements and Applications Proceedings, Budapest, Hungary, 18–19 May 2012; pp. 1–4. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Domain | Evaluated Indices |
|---|---|---|
| Linear | Time domain | Statistical indices: SDNN, SDANN, |
| SDNN, rMSSD, pNN50. | ||
| Linear | Time domain | Geometric indices: RRtri, TINN and |
| plot of Poincaré. | ||
| Linear | Frequency domain | HF, LF and VLF. |
| Nonlinear | - | Correlation function, hurst exponent, |
| fractal dimension and the | ||
| Lyapunovexponent. |
| Reference | Year | Disease | Evaluated Indices | Results |
|---|---|---|---|---|
| [70] | 2013 | Pneumonia | HRV and PPG signal | Mean squared error of 3.0 breathing/minute. |
| [108] | 2005 | Peripheral arterial occlusive disease of the lower limbs (PAOD) | PPG signal | 90% of accuracy and 100% of sensitivity. |
| [109] | 2011 | Obesity | HF, LF and VLF | Low levels of excess fat in eutrophic young increase cardiovascular risk. |
| [110] | 2012 | Respiratory sleeping disorders in patients with severe cardiovascular disease | PPG, EEG, ECG and EMG | Sensitivity of 98%, and specificity of 96%. |
| [111] | 2011 | Chronic heart failure (CHF) | Frequency and time domain | 89.74% sensitivity and 100% of specificity. |
| [112] | 2002 | Coronary heart disease | SDNN, HF | HRV can be used for identifying differences in the cardiac autonomic balance of healthy adults. |
| [113] | 2015 | Childhood pneumonia | Respiratory rate, HRV and SPO2 | 96.6% of sensitivity, 96.4% of specificity. |
| [106] | 2007 | Chronic obstructive pulmonary disease (COPD) | SDNN, RMSSD, HF, LF | Reduced HRV with decreased sympathetic and vagal activity. |
| [114] | 2011 | Respiratory sinus arrhythmia | HF | Mean error in RR detection of 0.05 to 4.23 breathing/minute for PPG and 1.59 to 3.70 breathing/minute for ECG. |
| [115] | 2008 | Renal insufficiency | SDNN, LF | Chronic renal patients not undergoing dialysis have reduced HRV. |
| [116] | 2015 | Cardiovascular risk (CR) | Pulse, SpO2 and PPG signal | Technical error of 0.8% and 1.0%. |
| [2] | 2011 | Peripheral arterial occlusive disease (PAOD) | Time domain | The PPG signal amplitude and distortion increases with disease severity. |
| Reference | Year | Technique | Proposal |
|---|---|---|---|
| [105] | 2012 | ECG | Application to assist in remote |
| monitoring of cardiac patients. | |||
| [117] | 2010 | ECG e PPG | Device for measuring the level |
| of stress of an individual. | |||
| [11] | 2006 | PPG | Low-cost prototype for blood |
| pressure measurement. | |||
| [119] | 2012 | PPG | A new prototype fiber–optic |
| probe was developed for | |||
| investigating PPG signals | |||
| from various splanchnic organs. | |||
| [25] | 2016 | PPG | Measurement of HRV through |
| hand image. | |||
| [64] | 2012 | PPG | Wireless system for monitoring |
| and training cyclists. | |||
| [70] | 2013 | PPG | Portable oximeter to aid in the |
| diagnosis of childhood pneumonia. | |||
| [27] | 2016 | PPG | Measurement of HRV by |
| facial detection. | |||
| [71] | 2014 | PPG | Obtainment of HRV in beef cattle. |
| [118] | 2008 | PPG | Oxygen saturation and heart rate |
| monitoring system for rodents. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraes, J.L.; Rocha, M.X.; Vasconcelos, G.G.; Vasconcelos Filho, J.E.; De Albuquerque, V.H.C.; Alexandria, A.R. Advances in Photopletysmography Signal Analysis for Biomedical Applications. Sensors 2018, 18, 1894. https://doi.org/10.3390/s18061894
Moraes JL, Rocha MX, Vasconcelos GG, Vasconcelos Filho JE, De Albuquerque VHC, Alexandria AR. Advances in Photopletysmography Signal Analysis for Biomedical Applications. Sensors. 2018; 18(6):1894. https://doi.org/10.3390/s18061894
Chicago/Turabian StyleMoraes, Jermana L., Matheus X. Rocha, Glauber G. Vasconcelos, José E. Vasconcelos Filho, Victor Hugo C. De Albuquerque, and Auzuir R. Alexandria. 2018. "Advances in Photopletysmography Signal Analysis for Biomedical Applications" Sensors 18, no. 6: 1894. https://doi.org/10.3390/s18061894