

Mucoadhesive Budesonide Solution for the Treatment of Pediatric Eosinophilic Esophagitis
 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Results and Discussion
2.1. Mucoadhesive Property Determination
2.2. Determination of Syringeability Properties
2.3. Solubility Study
2.4. Evaluation of Rheological Properties
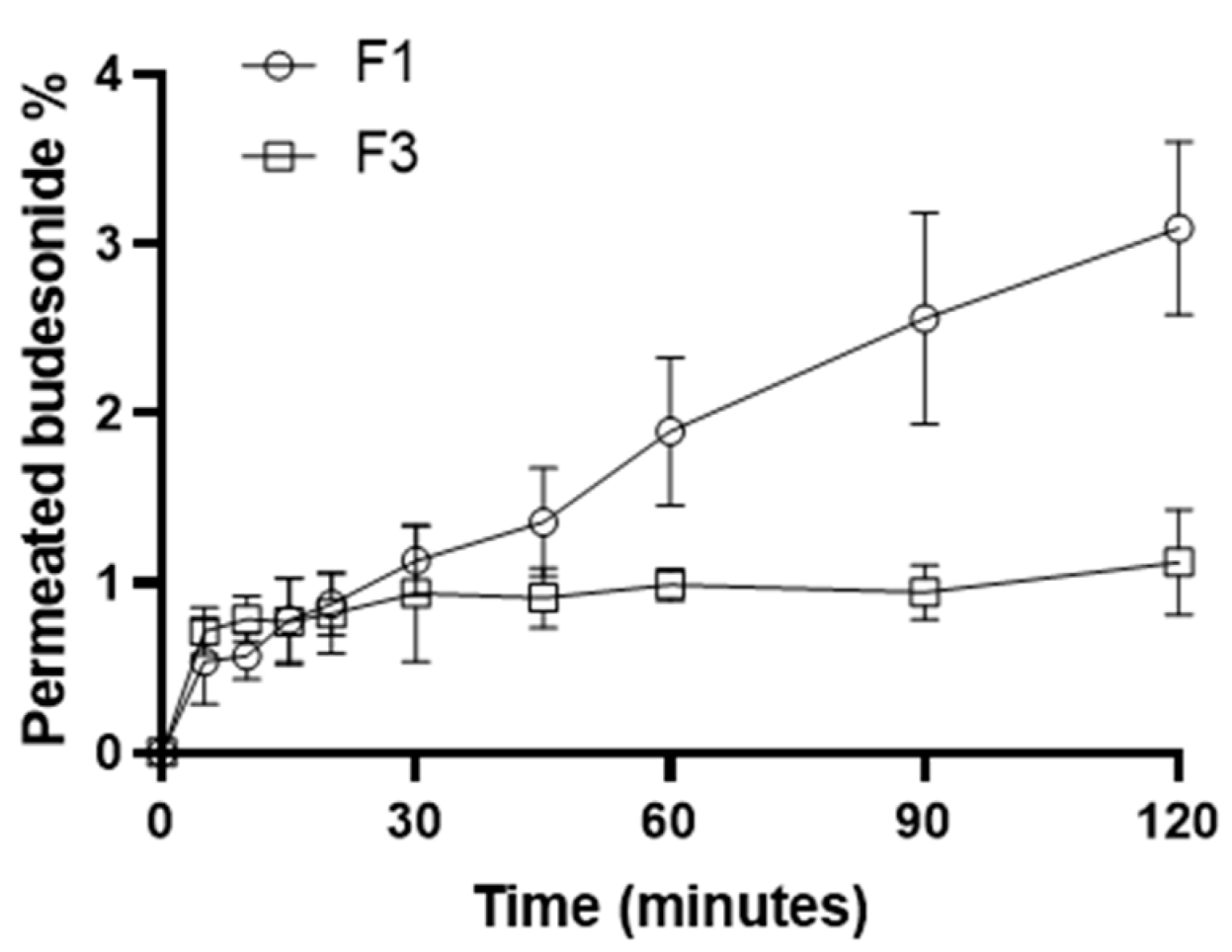
2.5. In Vitro Diffusion–Permeation Study
2.6. Physical–Chemical Stability Study
3. Materials and Methods
3.1. Materials
3.2. Preparation of BU Formulations
3.3. HPLC Method and Calibration Curve
3.4. Mucoadhesive Properties Determination
3.5. Determination of Syringeability Properties
3.6. Solubility Study
3.7. Evaluation of Rheological Properties
3.8. In Vitro Diffusion–Permeation Study
3.9. Physical–Chemical Stability Study
3.10. Statistical Analysis
4. Conclusions
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murali, A.R.; Gupta, A.; Attar, B.M.; Ravi, V.; Koduru, P. Topical Steroids in Eosinophilic Esophagitis: Systematic Review and Meta-Analysis of Placebo-Controlled Randomized Clinical Trials. J. Gastroenterol. Hepatol. 2016, 31, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Dellon, E.S.; Katzka, D.A.; Collins, M.H.; Hamdani, M.; Gupta, S.K.; Hirano, I.; Kagalwalla, A.; Lewis, J.; Markowitz, J.; Nurko, S.; et al. Budesonide Oral Suspension Improves Symptomatic, Endoscopic, and Histologic Parameters Compared with Placebo in Patients with Eosinophilic Esophagitis. Gastroenterology 2017, 152, 776–786.e5. [Google Scholar] [CrossRef] [PubMed]
- Greuter, T.; Safroneeva, E.; Bussmann, C.; Biedermann, L.; Vavricka, S.R.; Katzka, D.A.; Schoepfer, A.M.; Straumann, A. Maintenance Treatment of Eosinophilic Esophagitis with Swallowed Topical Steroids Alters Disease Course over A 5-Year Follow-up Period in Adult Patients. Clin. Gastroenterol. Hepatol. 2019, 17, 419–428.e6. [Google Scholar] [CrossRef] [PubMed]
- Oliva, S.; Rossetti, D.; Papoff, P.; Tiberti, A.; Mallardo, S.; Volpe, D.; Ruggiero, C.; Russo, G.; Vezzoli, D.; Isoldi, S.; et al. A 12-Week Maintenance Therapy with a New Prepared Viscous Budesonide in Pediatric Eosinophilic Esophagitis. Dig. Dis. Sci. 2019, 64, 1571–1578. [Google Scholar] [CrossRef]
- Underwood, B.; Troutman, T.D.; Schwartz, J.T. Breaking down the Complex Pathophysiology of Eosinophilic Esophagitis. Ann. Allergy Asthma Immunol. 2023, 130, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, D.; Marella, S.; Idelman, G.; Chang, J.W.; Chehade, M.; Hogan, S.P. Eosinophilic Esophagitis: Immune Mechanisms and Therapeutic Targets. Clin. Exp. Allergy 2022, 52, 1142–1156. [Google Scholar] [CrossRef] [PubMed]
- Hirano, I.; Safroneeva, E.; Roumet, M.C.; Comer, G.M.; Eagle, G.; Schoepfer, A.; Falk, G.W. Randomised Clinical Trial: The Safety and Tolerability of Fluticasone Propionate Orally Disintegrating Tablets versus Placebo for Eosinophilic Oesophagitis. Aliment. Pharmacol. Ther. 2020, 51, 750–759. [Google Scholar] [CrossRef]
- Syverson, E.P.; Hait, E.J. Treatment for Eosinophilic Esophagitis. Curr. Opin. Gastroenterol. 2020, 36, 485–490. [Google Scholar] [CrossRef]
- Gonsalves, N.P.; Aceves, S.S. Diagnosis and Treatment of Eosinophilic Esophagitis. J. Allergy Clin. Immunol. 2020, 145, 1–7. [Google Scholar] [CrossRef]
- Cotton, C.C.; Eluri, S.; Wolf, W.A.; Dellon, E.S. Six-Food Elimination Diet and Topical Steroids Are Effective for Eosinophilic Esophagitis: A Meta-Regression. Dig. Dis. Sci. 2017, 62, 2408–2420. [Google Scholar] [CrossRef]
- Molina–Infante, J.; Ferrando–Lamana, L.; Ripoll, C.; Hernandez–Alonso, M.; Mateos, J.M.; Fernandez–Bermejo, M.; Dueñas, C.; Fernandez–Gonzalez, N.; Quintana, E.M.; Gonzalez–Nuñez, M.A. Esophageal Eosinophilic Infiltration Responds to Proton Pump Inhibition in Most Adults. Clin. Gastroenterol. Hepatol. 2011, 9, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Molina-Infante, J.; Bredenoord, A.J.; Cheng, E.; Dellon, E.S.; Furuta, G.T.; Gupta, S.K.; Hirano, I.; Katzka, D.A.; Moawad, F.J.; Rothenberg, M.E.; et al. Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia: An Entity Challenging Current Diagnostic Criteria for Eosinophilic Oesophagitis. Gut 2016, 65, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Feo-Ortega, S.; Lucendo, A.J. Evidence-Based Treatments for Eosinophilic Esophagitis: Insights for the Clinician. Therap. Adv. Gastroenterol. 2022, 15, 175628482110686. [Google Scholar] [CrossRef] [PubMed]
- Nennstiel, S.; Schlag, C. Treatment of Eosinophlic Esophagitis with Swallowed Topical Corticosteroids. World J. Gastroenterol. 2020, 26, 5395–5407. [Google Scholar] [CrossRef] [PubMed]
- Hao, L.; Lu, Y.; Li, T.; Gong, B. A Meta-Analysis of Efficacy of Topical Steroids in Eosinophilic Esophagitis: From the Perspective of Histologic, Clinical, and Endoscopic Outcome. Gastroenterol. Hepatol. 2021, 44, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Casiraghi, A.; Gennari, C.G.; Musazzi, U.M.; Ortenzi, M.A.; Bordignon, S.; Minghetti, P. Mucoadhesive Budesonide Formulation for the Treatment of Eosinophilic Esophagitis. Pharmaceutics 2020, 12, 211. [Google Scholar] [CrossRef] [PubMed]
- Soltani, F.; Kamali, H.; Akhgari, A.; Garekani, H.A.; Nokhodchi, A.; Sadeghi, F. Different Trends for Preparation of Budesonide Pellets with Enhanced Dissolution Rate. Adv. Powder Technol. 2022, 33, 103684. [Google Scholar] [CrossRef]
- Bodas, D.S.; Ige, P.P. Central Composite Rotatable Design for Optimization of Budesonide-Loaded Cross-Linked Chitosan–Dextran Sulfate Nanodispersion: Characterization, in Vitro Diffusion and Aerodynamic Study. Drug Dev. Ind. Pharm. 2019, 45, 1193–1204. [Google Scholar] [CrossRef]
- López-Sanromán, A.; Clofent, J.; Garcia-Planella, E.; Menchén, L.; Nos, P.; Rodríguez-Lago, I.; Domènech, E. Revisando El Papel Terapéutico de La Budesonida En La Enfermedad de Crohn. Gastroenterol. Hepatol. 2018, 41, 458–471. [Google Scholar] [CrossRef]
- Reed, C.C.; Fan, C.; Koutlas, N.; Stefanadis, Z.; Eluri, S.; Shaheen, N.J.; Dellon, E.S. Compounded Oral Viscous Budesonide Is Effective and Provides a Durable Response in Eosinophilic Esophagitis. J. Gastroenterol. Hepatol. Res. 2018, 7, 2509–2515. [Google Scholar] [CrossRef]
- Pistone, M.; Racaniello, G.F.; Rizzi, R.; Iacobazzi, R.M.; Arduino, I.; Lopalco, A.; Lopedota, A.A.; Denora, N. Direct Cyclodextrin Based Powder Extrusion 3D Printing of Budesonide Loaded Mini-Tablets for the Treatment of Eosinophilic Colitis in Paediatric Patients. Int. J. Pharm. 2023, 632, 122592. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, J.P.; Gordon, M.; Sinopoulou, V.; Dellon, E.S.; Gupta, S.K.; Reed, C.C.; Gutiérrez-Junquera, C.; Venkatesh, R.D.; Erwin, E.A.; Egiz, A.; et al. Medical Treatment of Eosinophilic Esophagitis. Cochrane Database Syst. Rev. 2023, 2023, CD004065. [Google Scholar] [CrossRef] [PubMed]
- Bhalani, D.V.; Nutan, B.; Kumar, A.; Singh Chandel, A.K. Bioavailability Enhancement Techniques for Poorly Aqueous Soluble Drugs and Therapeutics. Biomedicines 2022, 10, 2055. [Google Scholar] [CrossRef] [PubMed]
- Lynnerup, J.T.; Eriksen, J.B.; Bauer-Brandl, A.; Holsæter, A.M.; Brandl, M. Insight into the Mechanism behind Oral Bioavailability-Enhancement by Nanosuspensions through Combined Dissolution/Permeation Studies. Eur. J. Pharm. Sci. 2023, 184, 106417. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Hill, M.; Vitanza, J.M.; Farber, R.H.; Desai, N.K.; Williams, J.; Song, I.H. Pharmacokinetics of Budesonide Oral Suspension in Children and Adolescents With Eosinophilic Esophagitis. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Ijaz, M.; Ahmad, M.; Akhtar, N.; Laffleur, F.; Bernkop-Schnürch, A. Thiolated α-Cyclodextrin: The Invisible Choice to Prolong Ocular Drug Residence Time. J. Pharm. Sci. 2016, 105, 2848–2854. [Google Scholar] [CrossRef] [PubMed]
- Bonengel, S.; Hauptstein, S.; Leonaviciute, G.; Griessinger, J.; Bernkop-Schnürch, A. Thiolated Alkyl-Modified Carbomers: Novel Excipients for Mucoadhesive Emulsions. Eur. J. Pharm. Sci. 2015, 75, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Baus, R.A.; Zahir-Jouzdani, F.; Dünnhaupt, S.; Atyabi, F.; Bernkop-Schnürch, A. Mucoadhesive Hydrogels for Buccal Drug Delivery: In Vitro-in Vivo Correlation Study. Eur. J. Pharm. Biopharm. 2019, 142, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Cilurzo, F.; Gennari, C.G.M.; Selmin, F.; Musazzi, U.M.; Rumio, C.; Minghetti, P. A Novel Oromucosal Prolonged Release Mucoadhesive Suspension by One Step Spray Coagulation Method. Curr. Drug Deliv. 2013, 10, 251–260. [Google Scholar] [CrossRef]
- Jones, D.S.; Woolfson, A.D.; Brown, A.F. Textural, Viscoelastic and Mucoadhesive Properties of Pharmaceutical Gels Composed of Cellulose Polymers. Int. J. Pharm. 1997, 151, 223–233. [Google Scholar] [CrossRef]
- Saxena, A.; Tewari, G.; Saraf, S.A. Formulation and Evaluation of Mucoadhesive Buccal Patch of Acyclovir Utilizing Inclusion Phenomenon. Brazilian J. Pharm. Sci. 2011, 47, 887–897. [Google Scholar] [CrossRef]
- Singh, G. Formulationn and evaluation of mucoadhesive microspheres of flurbiprofen. Pharmacologyonline 2010, 3, 659–670. [Google Scholar]
- Lee, C.A.; Kim, B.S.; Cho, C.W. Quantitative Evaluation of Mucoadhesive Polymers to Compare the Mucoadhesion. J. Pharm. Investig. 2016, 46, 189–194. [Google Scholar] [CrossRef]
- Alonso, J.M.; Andrade del Olmo, J.; Perez Gonzalez, R.; Saez-Martinez, V. Injectable Hydrogels: From Laboratory to Industrialization. Polymers 2021, 13, 650. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Racaniello, G.F.; Denora, N.; Gentile, L.; Lopalco, A.; Cutrignelli, A.; Franco, M.; Iacobazzi, R.M.; Laquintana, V.; Lopedota, A. Thermoresponsive Mucoadhesive Hydrogel Based on Pluronic F127/Thiolated Glycol Chitosan for Intravesical Administration of Celecoxib/Gemcitabine. J. Drug Deliv. Sci. Technol. 2023, 86, 104687. [Google Scholar] [CrossRef]
- Laquintana, V.; Asim, M.H.; Lopedota, A.; Cutrignelli, A.; Lopalco, A.; Franco, M.; Bernkop-Schnürch, A.; Denora, N. Thiolated Hydroxypropyl-β-Cyclodextrin as Mucoadhesive Excipient for Oral Delivery of Budesonide in Liquid Paediatric Formulation. Int. J. Pharm. 2019, 572, 118820. [Google Scholar] [CrossRef] [PubMed]
- Loftsson, T.; Guǒmundsdóttir, T.K.; Friǒriksdóttir, H. The Influence of Water-Soluble Polymers and PH on Hydroxypropyl-β-Cyclodextrin Complexation of Drugs. Drug Dev. Ind. Pharm. 1996, 22, 401–405. [Google Scholar] [CrossRef]
- Loftsson, T.; Másson, M.; Sigurjónsdóttir, J.F. Methods to Enhance the Complexation Efficiency of Cyclodextrins. S.T.P. Pharma Sci. 1999, 9, 237–242. [Google Scholar]
- Singh, I.; Aboul-Enein, H.Y. Influence of Water Soluble Polymers on Hydroxypropyl-β-Cyclodextrin Complexation of Rofecoxib. Pharmazie 2007, 62, 284–286. [Google Scholar] [CrossRef]
- Sorab, J.; Vanarsdale, W.E. A Correlation for the Pressure and Temperature Dependence of Viscosity. Tribol. Trans. 1991, 34, 604–610. [Google Scholar] [CrossRef]
- Fisher, C.H. Correlating Viscosity with Temperature and Other Properties. JAOCS J. Am. Oil Chem. Soc. 1998, 75, 1229–1232. [Google Scholar] [CrossRef]
- Chalah, K.; Benmounah, A.; Mahdad, M.; Kheribet, R. Rheological Study of Sodium Carboxymethylcellulose: Effect of Concentration and Molecular Weight. Mater. Today Proc. 2022, 53, 185–190. [Google Scholar] [CrossRef]
- Ghannam, M.T.; Esmail, M.N. Rheological Properties of Carboxymethyl Cellulose. J. Appl. Polym. Sci. 1997, 64, 289–301. [Google Scholar] [CrossRef]
- Edali, M.; Esmail, M.N.; Vatistas, G.H. Rheological Properties of High Concentrations of Carboxymethyl Cellulose Solutions. J. Appl. Polym. Sci. 2001, 79, 1787–1801. [Google Scholar] [CrossRef]
- Dabbaghi, M.; Namjoshi, S.; Panchal, B.; Grice, J.E.; Prakash, S.; Roberts, M.S.; Mohammed, Y. Viscoelastic and Deformation Characteristics of Structurally Different Commercial Topical Systems. Pharmaceutics 2021, 13, 1351. [Google Scholar] [CrossRef] [PubMed]
- Farinha, A.; Toscano, C.; Campos, R.; Bica, A.; Hadgraft, J. Permeation of Naproxen from Saturated Solutions and Commercial Formulations through Synthetic Membranes. Drug Dev. Ind. Pharm. 2003, 29, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.F.; Rouse, J.; Sanderson, D.; Eccleston, G. A Comparative Study of Transmembrane Diffusion and Permeation of Ibuprofen across Synthetic Membranes Using Franz Diffusion Cells. Pharmaceutics 2010, 2, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Francesco, G.; Lopedota, A.; Laquintana, V.; Arduino, I.; Lopalco, A.; Cutrignelli, A.; Franco, M.; Hrafn, H.; Denora, N. Chitosan/Sulfobutylether-β-Cyclodextrin Based Nanoparticles Coated with Thiolated Hyaluronic Acid for Indomethacin Ophthalmic Delivery. Int. J. Pharm. 2022, 622, 121905. [Google Scholar] [CrossRef] [PubMed]
- Sohi, H.; Ahuja, A.; Ahmad, F.J.; Khar, R.K. Critical Evaluation of Permeation Enhancers for Oral Mucosal Drug Delivery. Drug Dev. Ind. Pharm. 2010, 36, 254–282. [Google Scholar] [CrossRef]
- Másson, M.; Loftsson, T.; Másson, G.; Stefánsson, E. Cyclodextrins as Permeation Enhancers: Some Theoretical Evaluations and in Vitro Testing. J. Control. Release 1999, 59, 107–118. [Google Scholar] [CrossRef]
- Racaniello, G.F.; Balenzano, G.; Arduino, I.; Iacobazzi, R.M.; Lopalco, A.; Lopedota, A.A.; Sigurdsson, H.H.; Denora, N. Chitosan and Anionic Solubility Enhancer Sulfobutylether-β-Cyclodextrin-Based Nanoparticles as Dexamethasone Ophthalmic Delivery System for Anti-Inflammatory Therapy. Pharmaceutics 2024, 16, 277. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, Y.B.; Gurny, R.; Jordan, O. A Novel Thermoresponsive Hydrogel Based on Chitosan. Eur. J. Pharm. Biopharm. 2008, 68, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Spennacchio, A.; Lopedota, A.A.; la Forgia, F.M.; Fontana, S.; Denora, N.; Lopalco, A. Stability of Omeprazole Extemporaneous Oral Solution in Chopin Base. Int. J. Pharm. Compd. 2023, 27, 250–255. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Syringeability * (s) |
|---|---|
| F1 | 3.310 ± 0.266 |
| F2 | 2.014 ± 0.210 |
| F3 | 4.022 ± 0.318 |
| Sample | Temperature (°C) | Viscosity (mPa·s) | Δ Viscosity 56.3 vs. 100 s−1 (%) | Loss Factor (tan δ) | ||
|---|---|---|---|---|---|---|
| 56.3 (s−1) | 75 (s−1) | 100 (s−1) | ||||
| B1 | 25 | 190.65 | 180.31 | 169.23 | −11.23 | 9.68 ± 6.28 |
| B1 | 37 | 116.36 | 111.37 | 106.43 | −8.534 | 4.33 ± 2.43 |
| F1 | 25 | 178.91 | 169.88 | 160.40 | −10.35 | 12.73 ± 9.98 |
| F1 | 37 | 107.87 | 103.81 | 99.766 | −7.513 | 24.49 ± 22.49 |
| B3 | 25 | 166.77 | 156.83 | 146.85 | −11.94 | 4.90 ± 3.69 |
| B3 | 37 | 102.38 | 98.083 | 93.071 | −9.092 | 17.15 ± 19.88 |
| F3 | 25 | 100.78 | 97.81 | 94.775 | −5.959 | 15.81 ± 12.68 |
| F3 | 37 | 60.167 | 59.075 | 57.887 | −3.789 | 32.99 ± 30.62 |
| Sample | Temperature (°C) | K (Pa sn) | n | R2 |
|---|---|---|---|---|
| B1 | 25 | 0.2553 | 0.9517 | 0.9935 |
| B1 | 37 | 0.1598 | 0.9178 | 0.9949 |
| F1 | 25 | 0.2438 | 0.9239 | 0.9872 |
| F1 | 37 | 0.1439 | 0.9097 | 0.9653 |
| B3 | 25 | 0.1779 | 0.9490 | 0.9933 |
| B3 | 37 | 0.1200 | 0.8716 | 0.9554 |
| F3 | 25 | 0.1008 | 1.0360 | 0.9647 |
| F3 | 37 | 0.0835 | 0.8758 | 0.8913 |
| Formulation | J [µg h−1 cm−2] | Papp (×10−6) [cm s−1] | R |
|---|---|---|---|
| F1 | 8.05 | 3.19 | 2.72 |
| F3 | 2.96 | 1.18 |
| Qualitative Composition of the Liquid Vehicles | ||
|---|---|---|
| B1 | B2 | B3 |
| CMC Na | / | CMC Na |
| HP-β-CD | HP-β-CD | / |
| Sorbitol | Sorbitol | Sorbitol |
| Glycerol | Glycerol | Glycerol |
| Potassium sorbate | Potassium sorbate | Potassium sorbate |
| Citric acid | Citric acid | Citric acid |
| Trisodium citrate dihydrate | Trisodium citrate dihydrate | Trisodium citrate dihydrate |
| Raspberry flavor | Raspberry flavor | Raspberry flavor |
| Preserved water | Preserved water | Preserved water |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spennacchio, A.; Lopalco, A.; Racaniello, G.F.; Cutrignelli, A.; la Forgia, F.M.; Fontana, S.; Cristofori, F.; Francavilla, R.; Lopedota, A.A.; Denora, N. Mucoadhesive Budesonide Solution for the Treatment of Pediatric Eosinophilic Esophagitis. Pharmaceuticals 2024, 17, 550. https://doi.org/10.3390/ph17050550
Spennacchio A, Lopalco A, Racaniello GF, Cutrignelli A, la Forgia FM, Fontana S, Cristofori F, Francavilla R, Lopedota AA, Denora N. Mucoadhesive Budesonide Solution for the Treatment of Pediatric Eosinophilic Esophagitis. Pharmaceuticals. 2024; 17(5):550. https://doi.org/10.3390/ph17050550
Chicago/Turabian StyleSpennacchio, Antonio, Antonio Lopalco, Giuseppe Francesco Racaniello, Annalisa Cutrignelli, Flavia Maria la Forgia, Sergio Fontana, Fernanda Cristofori, Ruggiero Francavilla, Angela Assunta Lopedota, and Nunzio Denora. 2024. "Mucoadhesive Budesonide Solution for the Treatment of Pediatric Eosinophilic Esophagitis" Pharmaceuticals 17, no. 5: 550. https://doi.org/10.3390/ph17050550