
Feasibility of Multiple Examinations Using 68Ga-Labelled Collagelin Analogues: Organ Distribution in Rat for Extrapolation to Human Organ and Whole-Body Radiation Dosimetry


Abstract
:1. Introduction
2. Material and Methods
2.1. Materials
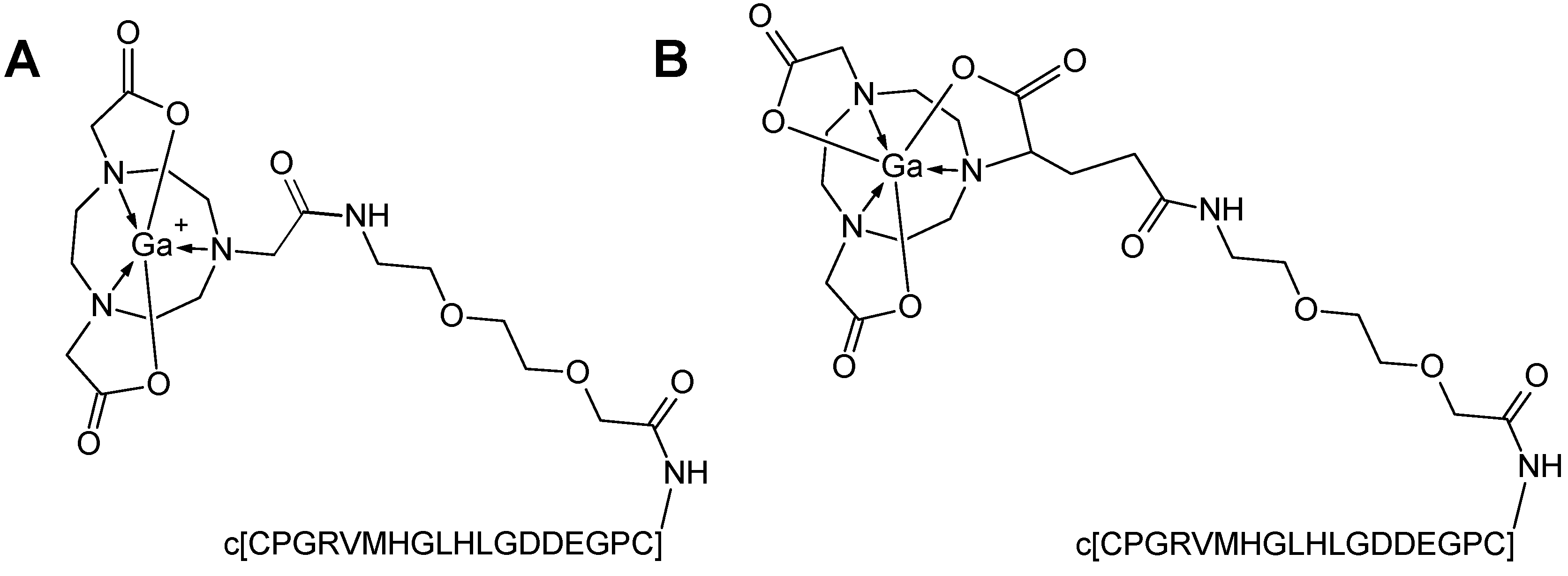
2.2. Peptide Synthesis and Radiochemistry
2.3. Organ Distribution Study
2.4. Dosimetric Calculations
2.5. Statistical Analysis
3. Results
3.1. Radiochemistry
3.2. Organ Distribution and Kinetics
3.3. Dosimetry
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Muzard, J.; Sarda-Mantel, L.; Loyau, S.; Meulemans, A.; Louedec, L.; Bantsimba-Malanda, C.; Hervatin, F.; Marchal-Somme, J.; Michel, J.B.; Le Guludec, D.; et al. Non-invasive molecular imaging of fibrosis using a collagen-targeted peptidomimetic of the platelet collagen receptor glycoprotein vi. PLoS ONE 2009, 4, e5585. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I.; Rosenstrom, U.; Estrada, S.; Ljungvall, I.; Haggstrom, J.; Eriksson, O.; Antoni, G. Synthesis and preclinical evaluation of 68Ga-labeled collagelin analogs for imaging and quantification of fibrosis. Nucl. Med. Biol. 2014, 41, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I. Positron emitting [68Ga]Ga-based imaging agents: Chemistry and diversity. Med. Chem. 2011, 7, 338–372. [Google Scholar] [CrossRef]
- Velikyan, I. The diversity of 68Ga-based imaging agents. Recent Results Cancer Res. 2013, 194, 101–131. [Google Scholar] [PubMed]
- Velikyan, I. Prospective of 68Ga-radiopharmaceutical development. Theranostics 2014, 4, 47–80. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I. Continued rapid growth in 68Ga applications: Update 2013 to June 2014. J. Label. Compd. Radiopharm. 2015, 58, 99–121. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I. 68Ga-based radiopharmaceuticals: Production and application relationship. Molecules 2015, 20, 12913–12943. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, U.; Lassmann, M. Dosimetry of [68Ga]-labeled compounds. Appl. Radiat. Isot. 2013, 76, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, M.; Chiesa, C.; Flux, G.; Bardiès, M. Eanm dosimetry committee guidance document: Good practice of clinical dosimetry reporting. Eur. J. Nucl. Med. Mol. Imaging 2010, 38, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Bouchelouche, K.; Capala, J. Image and treat: An individualized approach to urological tumors. Curr. Opin. Oncol. 2010, 22, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Bolch, W.E.; Eckerman, K.F.; Sgouros, G.; Thomas, S.R.; Brill, A.B.; Fisher, D.R.; Howell, R.W.; Meredith, R.; Wessels, B.W. Mird pamphlet No. 21: A generalized schema for radiopharmaceutical dosimetry-standardization of nomenclature. J. Nucl. Med. 2009, 50, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Loevinger, R.; Budinger, T.; Watson, E. Mird Primer for Absorbed Dose Calculations; Society of Nuclear Medicine: New York, NY, USA, 1988. [Google Scholar]
- Stabin, M.G.; Sparks, R.B.; Crowe, E. Olinda/EXM: The second-generation personal computer software for internal dose assessment in nuclear medicine. J. Nucl. Med. 2005, 46, 1023–1027. [Google Scholar] [PubMed]
- Sgouros, G. Bone marrow dosimetry for radioimmunotherapy: Theoretical considerations. J. Nucl. Med. 1993, 34, 689–694. [Google Scholar] [PubMed]
- Bouchet, L.G.; Bolch, W.E.; Blanco, H.P.; Wessels, B.W.; Siegel, J.A.; Rajon, D.A.; Clairand, I.; Sgouros, G. Mird pamphlet No. 19: Absorbed fractions and radionuclide s values for six age-dependent multiregion models of the kidney. J. Nucl. Med. 2003, 44, 1113–1147. [Google Scholar] [PubMed]
- Lewis, J.S.; Wang, M.; Laforest, R.; Wang, F.; Erion, J.L.; Bugaj, J.E.; Srinivasan, A.; Anderson, C.J. Toxicity and dosimetry of 177Lu-DOTA-Y3-octreotate in a rat model. Int. J. Cancer 2001, 94, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.; Bernhardt, P.; Nilsson, O.; Ahlman, H.; Kolby, L.; Schmitt, J.; Forssel-Aronsson, E. Biodistribution and dosimetry of 177Lu-labeled [DOTA0,Tyr3]octreotate in male nude mice with human small cell lung cancer. Cancer Biother. Radiopharm. 2003, 18, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Laforest, R.; Lewis, M.R.; Anderson, C.J. Comparative dosimetry of copper-64 and yttrium-90-labeled somatostatin analogs in a tumor-bearing rat model. Cancer Biother. Radiopharm. 2000, 15, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I.; Bulenga, T.N.; Selvaraju, K.R.; Lubberink, M.; Espes, D.; Rosenstrom, U.; Eriksson, O. Dosimetry of [177Lu]-DO3A-vs-Cys40-exendin-4—Impact on the feasibility of insulinoma internal radiotherapy. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 109–126. [Google Scholar] [PubMed]
- De Jong, M.; Breeman, W.A.P.; Bernard, B.F.; Bakker, W.H.; Schaar, M.; van Gameren, A.; Bugaj, J.E.; Erion, J.; Schmidt, M.; Srinivasan, A.; et al. [177Lu-DOTA0,Tyr3]octreotate for somatostatin receptor-targeted radionuclide therapy. Int. J. Cancer 2001, 92, 628–633. [Google Scholar] [CrossRef]
- Selvaraju, R.; Bulenga, T.N.; Espes, D.; Lubberink, M.; Sörensen, J.; Eriksson, B.; Estrada, S.; Velikyan, I.; Eriksson, O. Dosimetry of [68Ga]Ga-DO3A-vs-Cys40-exendin-4 in rodents, pigs, non-human primates and human—Repeated scanning in human is possible. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 259–269. [Google Scholar] [PubMed]
- Sandstrom, M.; Garske-Roman, U.; Granberg, D.; Johansson, S.; Widstrom, C.; Eriksson, B.; Sundin, A.; Lundqvist, H.; Lubberink, M. Individualized dosimetry of kidney and bone marrow in patients undergoing 177Lu-DOTA-octreotate treatment. J. Nucl. Med. 2013, 54, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Forrer, F.; Krenning, E.P.; Kooij, P.P.; Bernard, B.F.; Konijnenberg, M.; Bakker, W.H.; Teunissen, J.J.; de Jong, M.; van Lom, K.; de Herder, W.W.; et al. Bone marrow dosimetry in peptide receptor radionuclide therapy with [177Lu-DOTA0,Tyr3]octreotate. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Sandström, M.; Velikyan, I.; Garske-Román, U.; Sörensen, J.; Eriksson, B.; Granberg, D.; Lundqvist, H.; Sundin, A.; Lubberink, M. Comparative biodistribution and radiation dosimetry of 68Ga-DOTATOC and 68Ga-DOTATATE in patients with neuroendocrine tumors. J. Nucl. Med. 2013, 54, 1755–1759. [Google Scholar] [CrossRef] [PubMed]
- Radiation exposure, dose limits, Germany. European Nuclear Sosciety. Available online: http://www.euronuclear.org/info/encyclopedia/r/radiation-exposure-dose-limit.htm (accessed on 2 June 2016).
- U.S. Food and Drug Administration Web Site. Code of Federal Regulations Title 21, section 361.1: Radioactive Drugs for Certain Research Uses. Available online: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?FR5361.1 (accessed on 1 April 2013).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tracer | N (gender) | Animal Weight *, (g) | Injected Dose *, (MBq) |
|---|---|---|---|
| [68Ga]Ga-NO2A-Col | 6 (male) | 397 ± 18 | 8.5 ± 1.5 |
| [68Ga]Ga-NO2A-Col | 6 (female) | 261 ± 23 | 7.7 ± 2.6 |
| [68Ga]Ga-NODAGA-Col | 6 (male) | 374 ± 28 | 17.3 ± 1.7 |
| [68Ga]Ga-NODAGA-Col | 6 (female) | 243 ± 7 | 11.9 ± 4.4 |
| Organ | [68Ga]Ga-NO2A-Col | [68Ga]Ga-NODAGA-Col | ||
|---|---|---|---|---|
| Female | Male | Female | Male | |
| Kidneys | 0.103 | 0.102 | 0.111 | 0.100 |
| Adrenals | 0.009 | 0.009 | 0.009 | 0.008 |
| Liver | 0.007 | 0.006 | 0.014 | 0.012 |
| LLI wall * | 0.022 | 0.020 | 0.023 | 0.020 |
| ULI wall ** | 0.019 | 0.016 | 0.019 | 0.015 |
| Red marrow | 0.017 | 0.017 | 0.016 | 0.016 |
| Spleen | 0.008 | 0.006 | 0.011 | 0.011 |
| Osteogenic cells | 0.032 | 0.025 | 0.030 | 0.024 |
| Small intestine | 0.020 | 0.018 | 0.020 | 0.018 |
| Ovaries/testes | 0.009 | 0.015 | 0.009 | 0.015 |
| Urinary bladder wall | 0.016 | 0.013 | 0.017 | 0.018 |
| Breasts | 0.016 | N/A *** | 0.016 | N/A *** |
| Uterus | 0.019 | N/A *** | 0.019 | N/A *** |
| Stomach wall | 0.019 | 0.015 | 0.019 | 0.015 |
| Skin | 0.015 | 0.012 | 0.015 | 0.011 |
| Lungs | 0.009 | 0.007 | 0.008 | 0.007 |
| Heart wall | 0.008 | 0.006 | 0.008 | 0.006 |
| Muscle | 0.006 | 0.005 | 0.006 | 0.005 |
| Pancreas | 0.008 | 0.007 | 0.008 | 0.007 |
| Brain | 0.003 | 0.002 | 0.002 | 0.002 |
| Total body | 0.018 | 0.015 | 0.018 | 0.015 |
| Total effective dose (mSv/MBq) | 0.016 | 0.016 | 0.016 | 0.014 |
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velikyan, I.; Rosenström, U.; Bulenga, T.N.; Eriksson, O.; Antoni, G. Feasibility of Multiple Examinations Using 68Ga-Labelled Collagelin Analogues: Organ Distribution in Rat for Extrapolation to Human Organ and Whole-Body Radiation Dosimetry. Pharmaceuticals 2016, 9, 31. https://doi.org/10.3390/ph9020031
Velikyan I, Rosenström U, Bulenga TN, Eriksson O, Antoni G. Feasibility of Multiple Examinations Using 68Ga-Labelled Collagelin Analogues: Organ Distribution in Rat for Extrapolation to Human Organ and Whole-Body Radiation Dosimetry. Pharmaceuticals. 2016; 9(2):31. https://doi.org/10.3390/ph9020031
Chicago/Turabian StyleVelikyan, Irina, Ulrika Rosenström, Thomas N. Bulenga, Olof Eriksson, and Gunnar Antoni. 2016. "Feasibility of Multiple Examinations Using 68Ga-Labelled Collagelin Analogues: Organ Distribution in Rat for Extrapolation to Human Organ and Whole-Body Radiation Dosimetry" Pharmaceuticals 9, no. 2: 31. https://doi.org/10.3390/ph9020031