
Phytocannabinoids CBD, CBG, and their Derivatives CBD-HQ and CBG-A Induced In Vitro Cytotoxicity in 2D and 3D Colon Cancer Cell Models

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
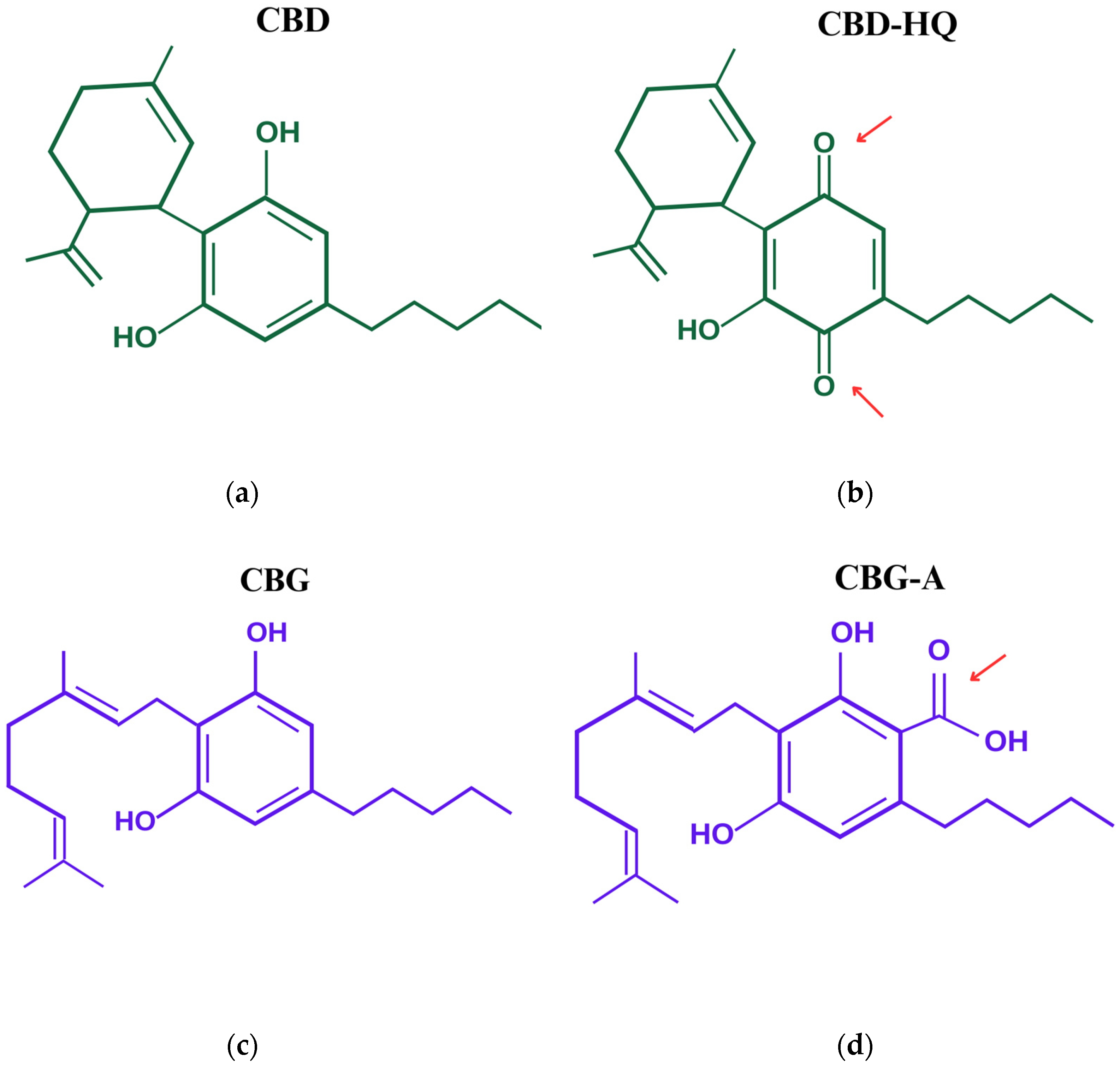
2.2. Compounds

2.3. MTT Assay
2.4. Spheroids
2.5. DCF-DA Assay
2.6. Statistical Analysis
3. Results
3.1. Study of the Capacity of Cannabinoids to Eliminate Colon Cancer Cells
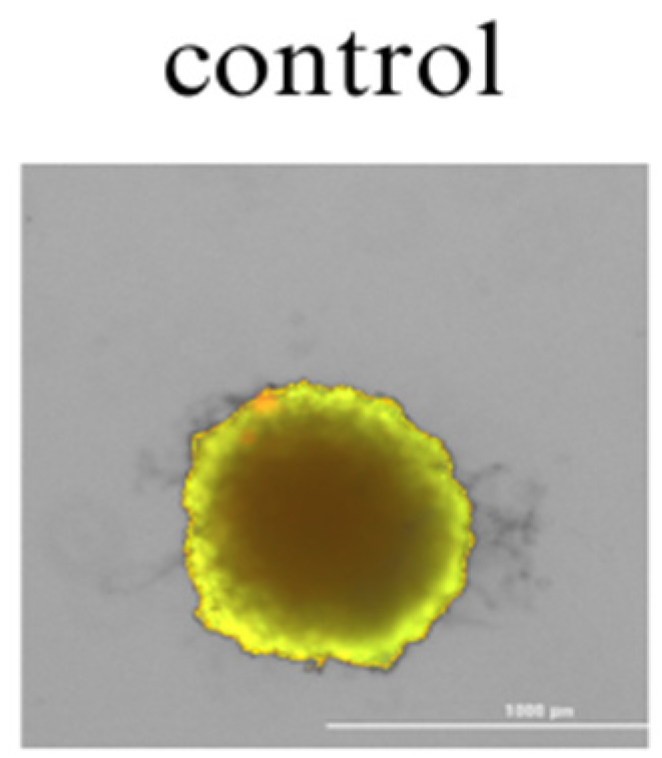
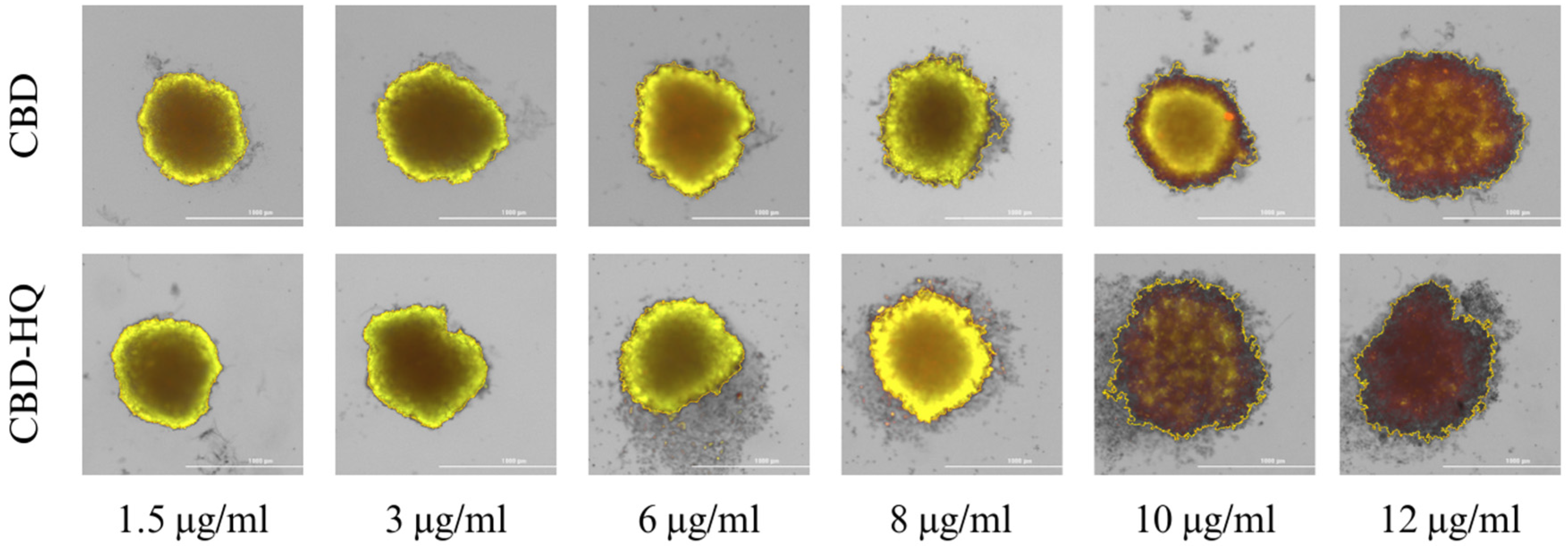
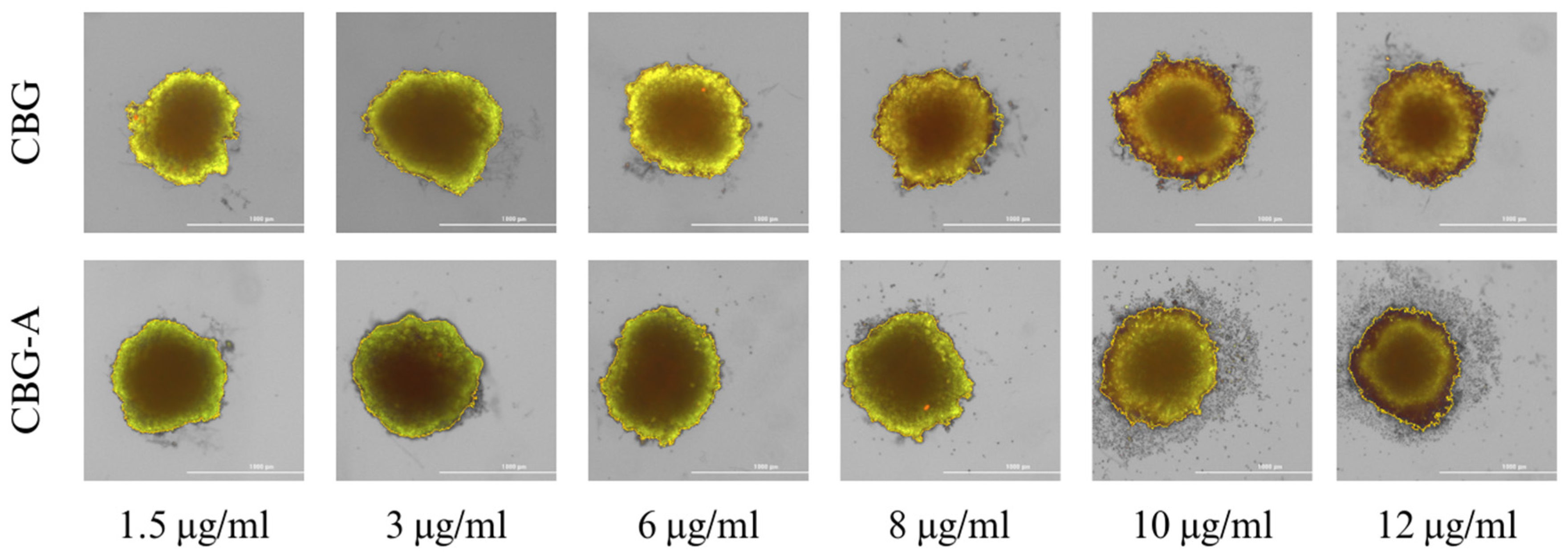
3.2. Study of the Cannabinoid’s Effect on Spheroid Growth
3.3. Study of the Antioxidative Effect of Cannabinoids
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agar, M. Medicinal cannabinoids in palliative care. Br. J. Clin. Pharmacol. 2018, 84, 2491–2494. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Information for Health Care Professionals: Cannabis (Marihuana, Marijuana) and the Cannabinoids; Health Canada: Ottawa, ON, Canada, 2018; ISBN 978-0-660-27828-5.
- Graczyk, M.; Lepper, W. The role of cannabinoids in the management of symptoms in palliative care patients. Palliat. Med. Pract. 2021, 15, 182–191. [Google Scholar] [CrossRef]
- Velasco, G.; Hernández-Tiedra, S.; Dávila, D.; Lorente, M. The use of cannabinoids as anticancer agents. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 64, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Pagano, E.; Iannotti, F.A.; Piscitelli, F.; Romano, B.; Lucariello, G.; Venneri, T.; Di Marzo, V.; Izzo, A.A.; Borrelli, F. Efficacy of combined therapy with fish oil and phytocannabinoids in murine intestinal inflammation. Phytother. Res. 2021, 35, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, F.; Pagano, E.; Romano, B.; Panzera, S.; Maiello, F.; Coppola, D.; De Petrocellis, L.; Buono, L.; Orlando, P.; Izzo, A.A. Colon carcinogenesis is inhibited by the TRPM8 antagonist cannabigerol, a Cannabis-derived non-psychotropic cannabinoid. Carcinogenesis 2014, 35, 2787–2797. [Google Scholar] [CrossRef] [PubMed]
- Guggisberg, J.; Schumacher, M.; Gilmore, G.; Zylla, D.M. Cannabis as an Anticancer Agent: A Review of Clinical Data and Assessment of Case Reports. Cannabis Cannabinoid Res. 2022, 7, 24–33. [Google Scholar] [CrossRef]
- Rodak, K.; Bęben, D.; Birska, M.; Siwiela, O.; Kokot, I.; Moreira, H.; Radajewska, A.; Szyjka, A.; Kratz, E.M. Evaluating the Neuroprotective Potential of Caffeinated Coffee in the Context of Aluminum-Induced Neurotoxicity: Insights from a PC12 Cell Culture Model. Antioxidants 2024, 13, 342. [Google Scholar] [CrossRef]
- Radajewska, A.; Moreira, H.; Bęben, D.; Siwiela, O.; Szyjka, A.; Gębczak, K.; Nowak, P.; Frąszczak, J.; Emhemmed, F.; Muller, C.D.; et al. Combination of Irinotecan and Melatonin with the Natural Compounds Wogonin and Celastrol for Colon Cancer Treatment. Int. J. Mol. Sci. 2023, 24, 9544. [Google Scholar] [CrossRef] [PubMed]
- Horn, S.R.; Stoltzfus, K.C.; Lehrer, E.J.; Dawson, L.A.; Tchelebi, L.; Gusani, N.J.; Sharma, N.K.; Chen, H.; Trifiletti, D.M.; Zaorsky, N.G. Epidemiology of liver metastases. Cancer Epidemiol. 2020, 67, 101760. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Verkuijl, S.J.; Jonker, J.E.; Trzpis, M.; Burgerhof, J.G.M.; Broens, P.M.A.; Furnée, E.J.B. Functional outcomes of surgery for colon cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2021, 47, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371, 4087. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Hamilton, J.P.; Pham, G.M.; Crisovan, E.; Wiegert-Rininger, K.; Vaillancourt, B.; DellaPenna, D.; Buell, C.R. De novo genome assembly of Camptotheca acuminata, a natural source of the anti-cancer compound camptothecin. Gigascience 2017, 6, gix065. [Google Scholar] [CrossRef] [PubMed]
- Arbuck, S.G.; Dorr, A.; Friedman, M.A. Paclitaxel (Taxol) in breast cancer. Hematol. Oncol. Clin. North. Am. 1994, 8, 121–140. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Horbańczuk, M.; Tzvetkov, N.T.; Mocan, A.; Carradori, S.; Maggi, F.; Marchewka, J.; Sut, S.; Dall’Acqua, S.; Gan, R.-Y.; et al. Curcumin: Total-Scale Analysis of the Scientific Literature. Molecules 2019, 24, 1393. [Google Scholar] [CrossRef] [PubMed]
- Echeverry, C.; Reyes-Parada, M.; Scorza, C. Constituents of Cannabis sativa. Adv. Exp. Med. Biol. 2021, 1297, 1–9. [Google Scholar] [CrossRef]
- Radwan, M.M.; Chandra, S.; Gul, S.; ElSohly, M.A. Cannabinoids, Phenolics, Terpenes and Alkaloids of Cannabis. Molecules 2021, 26, 2774. [Google Scholar] [CrossRef]
- Suchopár, J.; Laštůvka, Z.; Mašková, S.; Alblová, M.; Pařízek, A. Endocannabinoids. Endokanabinoidy. Ceska Gynekol. 2021, 86, 414–420. [Google Scholar] [CrossRef]
- Howlett, A.C.; Barth, F.; Bonner, T.I.; Cabral, G.; Casellas, P.; Devane, W.A.; Felder, C.C.; Herkenham, M.; Mackie, K.; Martin, B.R.; et al. International Union of Pharmacology. XXVII. Classification of cannabinoid receptors. Pharmacol. Rev. 2002, 54, 161–202. [Google Scholar] [CrossRef]
- Lu, H.C.; Mackie, K. An Introduction to the Endogenous Cannabinoid System. Biol. Psychiatry 2016, 79, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Lin, Q.; Sun, S.; Yang, N.; Xia, Y.; Cao, S.; Zhang, W.; Li, Q.; Guo, H.; Zhu, M.; et al. Inhibition of cannabinoid receptor type 1 sensitizes triple-negative breast cancer cells to ferroptosis via regulating fatty acid metabolism. Cell Death Dis. 2022, 13, 808. [Google Scholar] [CrossRef] [PubMed]
- Costas-Insua, C.; Guzmán, M. Endocannabinoid signaling in glioma. Glia 2023, 71, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Bunsick, D.A.; Matsukubo, J.; Aldbai, R.; Baghaie, L.; Szewczuk, M.R. Functional Selectivity of Cannabinoid Type 1 G Protein-Coupled Receptor Agonists in Transactivating Glycosylated Receptors on Cancer Cells to Induce Epithelial-Mesenchymal Transition Metastatic Phenotype. Cells 2024, 13, 480. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Bátkai, S.; Kunos, G. The endocannabinoid system as an emerging target of pharmacotherapy. Pharmacol. Rev. 2006, 58, 389–462. [Google Scholar] [CrossRef] [PubMed]
- Jastrząb, A.; Jarocka-Karpowicz, I.; Skrzydlewska, E. The Origin and Biomedical Relevance of Cannabigerol. Int. J. Mol. Sci. 2022, 23, 7929. [Google Scholar] [CrossRef] [PubMed]
- Navarro, G.; Varani, K.; Lillo, A.; Vincenzi, F.; Rivas-Santisteban, R.; Raïch, I.; Reyes-Resina, I.; Ferreiro-Vera, C.; Borea, P.A.; de Medina, V.S.; et al. Pharmacological data of cannabidiol- and cannabigerol-type phytocannabinoids acting on cannabinoid CB1, CB2 and CB1/CB2 heteromer receptors. Pharmacol. Res. 2020, 159, 104940. [Google Scholar] [CrossRef] [PubMed]
- Doppen, M.; Kung, S.; Maijers, I.; John, M.; Dunphy, H.; Townsley, H.; Eathorne, A.; Semprini, A.; Braithwaite, I. Cannabis in Palliative Care: A Systematic Review of Current Evidence. J. Pain. Symptom Manag. 2022, 64, 260–284. [Google Scholar] [CrossRef] [PubMed]
- van Breemen, R.B.; Muchiri, R.N.; Bates, T.A.; Weinstein, J.B.; Leier, H.C.; Farley, S.; Tafesse, F.G. Cannabinoids Block Cellular Entry of SARS-CoV-2 and the Emerging Variants. J. Nat. Prod. 2022, 85, 176–184. [Google Scholar] [CrossRef]
- Cas, M.D.; Casagni, E.; Casiraghi, A.; Minghetti, P.; Fornasari, D.M.M.; Ferri, F.; Arnoldi, S.; Gambaro, V.; Roda, G. Phytocannabinoids Profile in Medicinal Cannabis Oils: The Impact of Plant Varieties and Preparation Methods. Front. Pharmacol. 2020, 11, 570616. [Google Scholar] [CrossRef]
- Morgan, J.; Gschwend, G.; Houston, M.; Jones, A.; Kelso, C. Vaping preferences of individuals who vaporise dry herb cannabis, cannabis liquids and cannabis concentrates. Drug Alcohol. Depend. 2022, 240, 109632. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenberg, A.; Carpenter, H.; Wright, C.; Bayazeid, O.; Brokl, M. Characterizing the degradation of cannabidiol in an e-liquid formulation. Sci. Rep. 2022, 12, 20058. [Google Scholar] [CrossRef] [PubMed]
- Zheljazkov, V.D.; Maggi, F. Valorization of CBD-hemp through distillation to provide essential oil and improved cannabinoids profile. Sci. Rep. 2021, 11, 19890. [Google Scholar] [CrossRef] [PubMed]
- Citti, C.; Pacchetti, B.; Vandelli, M.A.; Forni, F.; Cannazza, G. Analysis of cannabinoids in commercial hemp seed oil and decarboxylation kinetics studies of cannabidiolic acid (CBDA). J. Pharm. Biomed. Anal. 2018, 149, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Orrego-González, E.; Londoño-Tobón, L.; Ardila-González, J.; Polania-Tovar, D.; Valencia-Cárdenas, A.; Velez-Van Meerbeke, A. Cannabinoid Effects on Experimental Colorectal Cancer Models Reduce Aberrant Crypt Foci (ACF) and Tumor Volume: A Systematic Review. Evid. Based Complement. Alternat. Med. 2020, 2020, 2371527. [Google Scholar] [CrossRef] [PubMed]
- Mazuz, M.; Tiroler, A.; Moyal, L.; Hodak, E.; Nadarajan, S.; Vinayaka, A.C.; Gorovitz-Haris, B.; Lubin, I.; Drori, A.; Drori, G.; et al. Synergistic cytotoxic activity of cannabinoids from cannabis sativa against cutaneous T-cell lymphoma (CTCL) in-vitro and ex-vivo. Oncotarget 2020, 11, 1141–1156. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Usami, N.; Yamamoto, I.; Yoshimura, H. Inhibitory effect of cannabidiol hydroxy-quinone, an oxidative product of cannabidiol, on the hepatic microsomal drug-metabolizing enzymes of mice. J. Pharmacobiodyn. 1991, 14, 421–427. [Google Scholar] [CrossRef]
- Usami, N.; Yamamoto, I.; Watanabe, K. Generation of reactive oxygen species during mouse hepatic microsomal metabolism of cannabidiol and cannabidiol hydroxy-quinone. Life Sci. 2008, 83, 717–724. [Google Scholar] [CrossRef]
- Wilson, J.T.; Fief, C.A.; Jackson, K.D.; Mercer, S.L.; Deweese, J.E. HU-331 and Oxidized Cannabidiol Act as Inhibitors of Human Topoisomerase IIα and β. Chem. Res. Toxicol. 2018, 31, 137–144. [Google Scholar] [CrossRef]
- Karelia, D.; Corey, Z.; Wang, H.; Raup-Konsavage, W.M.; Vrana, K.E.; Lü, J.; Jiang, C. Library Screening and Preliminary Characterization of Synthetic Cannabinoids Against Prostate and Pancreatic Cancer Cell Lines. Cannabis Cannabinoid Res. 2023, 9, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Yamaori, S.; Okushima, Y.; Yamamoto, I.; Watanabe, K. Characterization of the structural determinants required for potent mechanism-based inhibition of human cytochrome P450 1A1 by cannabidiol. Chem. Biol. Interact. 2014, 215, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Cohen, K.; Weizman, A.; Weinstein, A. Positive and Negative Effects of Cannabis and Cannabinoids on Health. Clin. Pharmacol. Ther. 2019, 105, 1139–1147. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CBD | CBD-HQ | CBG | CBG-A | CBD+CBG | |
|---|---|---|---|---|---|
| IC50 [μg/mL] | 4.13 | 8.00 | 7.64 | 8.24 | 3.9 |
| IC50 [μM/mL] | 13.13 | 24.35 | 24.14 | 22.86 | 12.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bęben, D.; Siwiela, O.; Szyjka, A.; Graczyk, M.; Rzepka, D.; Barg, E.; Moreira, H. Phytocannabinoids CBD, CBG, and their Derivatives CBD-HQ and CBG-A Induced In Vitro Cytotoxicity in 2D and 3D Colon Cancer Cell Models. Curr. Issues Mol. Biol. 2024, 46, 3626-3639. https://doi.org/10.3390/cimb46040227
Bęben D, Siwiela O, Szyjka A, Graczyk M, Rzepka D, Barg E, Moreira H. Phytocannabinoids CBD, CBG, and their Derivatives CBD-HQ and CBG-A Induced In Vitro Cytotoxicity in 2D and 3D Colon Cancer Cell Models. Current Issues in Molecular Biology. 2024; 46(4):3626-3639. https://doi.org/10.3390/cimb46040227
Chicago/Turabian StyleBęben, Dorota, Oliwia Siwiela, Anna Szyjka, Michał Graczyk, Daniel Rzepka, Ewa Barg, and Helena Moreira. 2024. "Phytocannabinoids CBD, CBG, and their Derivatives CBD-HQ and CBG-A Induced In Vitro Cytotoxicity in 2D and 3D Colon Cancer Cell Models" Current Issues in Molecular Biology 46, no. 4: 3626-3639. https://doi.org/10.3390/cimb46040227