
Histologically Validated Myocardial Fibrosis in Relation to Left Ventricular Geometry and Its Function in Aortic Stenosis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics
3.2. Left Ventricular Geometry and Function
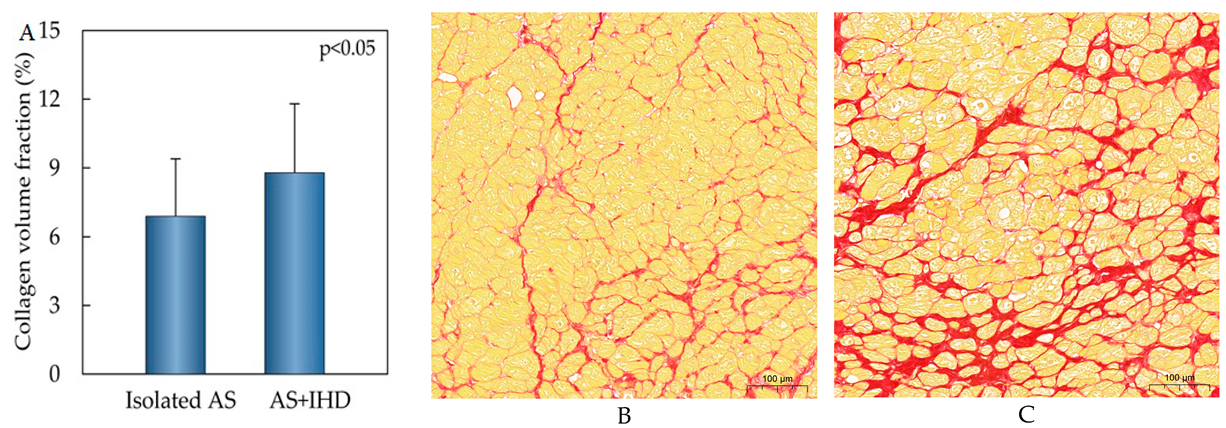
3.3. Myocardial Fibrosis
3.4. Myocardial Fibrosis Association with Left Ventricular Geometry and Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variables | Preoperative Period | Early Postoperative Period | Follow-Up Period | |||
|---|---|---|---|---|---|---|
| r | p Value | r | p Value | r | p Value | |
| Isolated A | ||||||
| LVEDD (mm) | 0.59 | 0.000 | 0.45 | 0.002 | 0.35 | 0.032 |
| LVEDDi (mm/m2) | 0.30 | 0.074 | 0.06 | 0.703 | 0.08 | 0.647 |
| LVM (g) | 0.42 | 0.011 | 0.36 | 0.026 | 0.43 | 0.007 |
| LVMi (g/m2) | 0.23 | 0.173 | 0.16 | 0.334 | 0.28 | 0.085 |
| LVEF (%) | −0.67 | 0.000 | −0.35 | 0.022 | −0.25 | 0.101 |
| LV septal thickness (mm) | −0.21 | 0.192 | 0.03 | 0.842 | 0.09 | 0.600 |
| LV posterior wall thickness (mm) | −0.28 | 0.082 | −0.07 | 0.678 | 0.09 | 0.594 |
| Mitral E velocity (cm/s) | −0.07 | 0.692 | −0.30 | 0.116 | −0.15 | 0.466 |
| Mitral E/A | 0.05 | 0.487 | −0.01 | 0.988 | −0.18 | 0.365 |
| Mitral E/e’ | −0.18 | 0.548 | −0.08 | 0.797 | −0.15 | 0.473 |
| AS+IHD | ||||||
| LVEDD (mm) | 0.14 | 0.254 | −0.09 | 0.453 | 0.07 | 0.612 |
| LVEDDi (mm/m2) | 0.22 | 0.075 | −0.02 | 0.879 | −0.04 | 0.769 |
| LVM (g) | 0.03 | 0.814 | 0.02 | 0.877 | 0.15 | 0.308 |
| LVMi (g/m2) | 0.06 | 0.650 | 0.03 | 0.787 | 0.06 | 0.693 |
| LVEF (%) | −0.03 | 0.780 | 0.05 | 0.681 | 0.05 | 0.756 |
| LV septal thickness (mm) | −0.14 | 0.254 | 0.07 | 0.584 | 0.02 | 0.917 |
| LV posterior wall thickness (mm) | −0.07 | 0.580 | 0.09 | 0.476 | 0.23 | 0.111 |
| Mitral E velocity (cm/s) | −0.19 | 0.176 | 0.08 | 0.571 | 0.10 | 0.608 |
| Mitral E/A | −0.14 | 0.361 | −0.18 | 0.225 | −0.09 | 0.653 |
| Mitral E/e’ | 0.01 | 0.945 | 0.35 | 0.070 | 0.60 | 0.001 |
References
- Herrmann, S.; Fries, B.; Salinger, T.; Liu, D.; Hu, K.; Gensler, D.; Strotmann, J.; Christa, M.; Beer, M.; Gattenlöhner, S.; et al. Myocardial Fibrosis Predicts 10-Year Survival in Patients Undergoing Aortic Valve Replacement. Circ. Cardiovasc. Imaging 2018, 11, e007131. [Google Scholar] [CrossRef]
- Krayenbuehl, H.P.; Hess, O.M.; Monrad, E.S.; Schneider, J.; Mall, G.; Turina, M. Left ventricular myocardial structure in aortic valve disease before, intermediate, and late after aortic valve replacement. Circulation 1989, 79, 744–755. [Google Scholar] [CrossRef]
- Paradis, J.-M.; Labbé, B.; Rodés-Cabau, J. Coronary artery disease and transcatheter aortic valve replacement: Current treatment paradigms. Coron. Artery Dis. 2015, 26, 272–278. [Google Scholar] [CrossRef]
- Virk, S.A.; Tian, D.H.; Liou, K.; Pathan, F.; Villanueva, C.; Akhunji, Z.; Cao, C. Systematic review of percutaneous coronary intervention and transcatheter aortic valve implantation for concomitant aortic stenosis and coronary artery disease. Int. J. Cardiol. 2015, 187, 453–455. [Google Scholar] [CrossRef]
- Ferreira, R.; Milei, J.; Forcada, P.; Beigelman, R.; Molteni, L.; Cutrin, J.C. The hypertrophied myocardium and coronary disease. Structural changes in patients submitted to aortocoronary bypass surgery. Int. J. Cardiol. 1992, 36, 203–212. [Google Scholar] [CrossRef]
- Hein, S.; Arnon, E.; Kostin, S.; Schönburg, M.; Elsässer, A.; Polyakova, V.; Bauer, E.P.; Klövekorn, W.-P.; Schaper, J. Progression from compensated hypertrophy to failure in the pressure-overloaded human: Heart structural deterioration and compensatory mechanisms. Circulation 2003, 107, 984–991. [Google Scholar] [CrossRef]
- Mohammed, S.F.; Hussain, S.; Mirzoyev, S.A.; Edwards, W.D.; Maleszewski, J.J.; Redfield, M.M. Coronary microvascular rarefaction and myocardial fibrosis in heart failure with preserved ejection fraction. Circulation 2015, 131, 550–559. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Aitaliyev, S.; Rumbinaitė, E.; Mėlinytė-Ankudavičė, K.; Nekrošius, R.; Keturakis, V.; Benetis, R. Early outcomes of patient-prosthesis mismatch following aortic valve replacement. Perfusion 2022, 37, 692–699. [Google Scholar] [CrossRef]
- Aitaliyev, S.; Rumbinaitė, E.; Mėlinytė-Ankudavičė, K.; Nekrošius, R.; Keturakis, V.; Benetis, R. Early hemodynamics after aortic valve replacement. Medicina 2020, 56, 674. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Takaoka, H.; Funabashi, N.; Uehara, M.; Iida, Y.; Kobayashi, Y. Diagnostic accuracy of CT for the detection of left ventricular myocardial fibrosis in various myocardial diseases. Int. J. Cardiol. 2017, 228, 375–379. [Google Scholar] [CrossRef]
- Chin, C.W.; Everett, R.J.; Kwiecinski, J.; Vesey, A.T.; Yeung, E.; Esson, G.; Jenkins, W.; Koo, M.; Mirsadraee, S.; White, A.C.; et al. Myocardial Fibrosis and Cardiac Decompensation in Aortic Stenosis. JACC Cardiovasc. Imaging 2017, 10, 1320–1333. [Google Scholar] [CrossRef]
- Balčiūnaitė, G.; Besusparis, J.; Palionis, D.; Žurauskas, E.; Skorniakov, V.; Janušauskas, V.; Zorinas, A.; Zaremba, T.; Valevičienė, N.; Šerpytis, P.; et al. Exploring myocardial fibrosis in severe aortic stenosis: Echo, CMR and histology data from FIB-AS study. Int. J. Cardiovasc. Imaging 2022, 38, 1555–1568. [Google Scholar] [CrossRef]
- Everett, R.J.; Tastet, L.; Clavel, M.-A.; Chin, C.W.; Capoulade, R.; Vassiliou, V.S.; Kwiecinski, J.; Gomez, M.; van Beek, E.J.; White, A.C.; et al. Progression of hypertrophy and myocardial fibrosis in aortic stenosis: A multicenter cardiac magnetic resonance study. Circ. Cardiovasc. Imaging 2018, 11, e007451. [Google Scholar] [CrossRef]
- Kvidal, P.; Bergström, P.; Hörte, L.-G.; Ståhle, E. Observed and relative survival after aortic valve replacement. J. Am. Coll. Cardiol. 2000, 35, 747–756. [Google Scholar] [CrossRef]
- Aleksandric, S.; Banovic, M.; Beleslin, B. Challenges in Diagnosis and Functional Assessment of Coronary Artery Disease in Patients with Severe Aortic Stenosis. Front. Cardiovasc. Med. 2022, 9, 849032. [Google Scholar] [CrossRef]
- Istrătoaie, O.; OfiŢeru, A.-M.; Nicola, G.-C.; Radu, R.-I.; Florescu, C.; Mogoantă, L.; Streba, C.T. Myocardial interstitial fibrosis—Histological and immunohistochemical aspects. Rom. J. Morphol. Embryol. 2015, 56, 1473–1480. [Google Scholar]
- Azevedo, C.F.; Nigri, M.; Higuchi, M.L.; Pomerantzeff, P.M.; Spina, G.S.; Sampaio, R.O.; Tarasoutchi, F.; Grinberg, M.; Rochitte, C.E. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J. Am. Coll. Cardiol. 2010, 56, 278–287. [Google Scholar] [CrossRef]
- Jellis, C.; Martin, J.; Narula, J.; Marwick, T.H. Assessment of Nonischemic Myocardial Fibrosis. J. Am. Coll. Cardiol. 2010, 56, 89–97. [Google Scholar] [CrossRef]
- Kempny, A.; Diller, G.-P.; Kaleschke, G.; Orwat, S.; Funke, A.; Radke, R.; Schmidt, R.; Kerckhoff, G.; Ghezelbash, F.; Rukosujew, A.; et al. Longitudinal left ventricular 2D strain is superior to ejection fraction in predicting myocardial recovery and symptomatic improvement after aortic valve implantation. Int. J. Cardiol. 2013, 167, 2239–2243. [Google Scholar] [CrossRef]
- Kvernby, S.; Rönnerfalk, M.; Warntjes, M.; Carlhäll, C.; Nylander, E.; Engvall, J.; Tamás, É.; Ebbers, T. Longitudinal changes in myocardial T1 and T2 relaxation times related to diffuse myocardial fibrosis in aortic stenosis; before and after aortic valve replacement. J. Magn. Reson. Imaging 2018, 48, 799–807. [Google Scholar] [CrossRef]
- Treibel, T.A.; López, B.; González, A.; Menacho, K.; Schofield, R.S.; Ravassa, S.; Fontana, M.; White, S.K.; DiSalvo, C.; Roberts, N.; et al. Reappraising myocardial fibrosis in severe aortic stenosis: An invasive and non-invasive study in 133 patients. Eur. Heart J. 2018, 39, 699–709. [Google Scholar] [CrossRef]
- Lammey, M.L.; Baskin, G.B.; Gigliotti, A.P.; Lee, D.R.; Ely, J.J.; Sleeper, M.M. Interstitial myocardial fibrosis in a captive chimpanzee (Pan troglodytes) population. Comp. Med. 2008, 58, 389–394. [Google Scholar]
- Messroghli, D.R.; Nordmeyer, S.; Dietrich, T.; Dirsch, O.; Kaschina, E.; Savvatis, K.; O H-Ici, D.; Klein, C.; Berger, F.; Kuehne, T. Assessment of diffuse myocardial fibrosis in rats using small-animal look-locker inversion recovery T1 mapping. Circ. Cardiovasc. Imaging 2011, 4, 636–640. [Google Scholar] [CrossRef]
- Rai, V.; Sharma, P.; Agrawal, S.; Agrawal, D.K. Relevance of mouse models of cardiac fibrosis and hypertrophy in cardiac research. Mol. Cell. Biochem. 2017, 424, 123–145. [Google Scholar] [CrossRef]
- Everett, R.; Stirrat, C.; Semple, S.; Newby, D.; Dweck, M.; Mirsadraee, S. Assessment of myocardial fibrosis with T1 mapping MRI. Clin. Radiol. 2016, 71, 768–778. [Google Scholar] [CrossRef]
- Flett, A.S.; Hayward, M.P.; Ashworth, M.T.; Hansen, M.S.; Taylor, A.M.; Elliott, P.M.; McGregor, C.; Moon, J.C. Equilibrium contrast cardiovascular magnetic resonance for the measurement of diffuse myocardial fibrosis: Preliminary validation in humans. Circulation 2010, 122, 138–144. [Google Scholar] [CrossRef]
- Evertz, R.; Hub, S.; Beuthner, B.E.; Backhaus, S.J.; Lange, T.; Schulz, A.; Toischer, K.; Seidler, T.; von Haehling, S.; Puls, M.; et al. Aortic valve calcification and myocardial fibrosis determine outcome following transcatheter aortic valve replacement. ESC Heart Fail. 2023, 10, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Giuseppe, T.; Giulia, P.; Alessandra, G.F.; Wanda, D.; Antonino, I.; Tito, T.; Giuseppe, B.; Teresa, C.M.; Corrado, T. Myocardial fibrosis in aortic stenosis: Comparison between clinical data, laboratory, echocardiography, and cardiac magnetic resonance. J. Cardiol. Cardiovasc. Med. 2023, 8, 051–058. [Google Scholar] [CrossRef]
- Park, S.J.; Cho, S.W.; Kim, S.M.; Ahn, J.; Carriere, K.; Jeong, D.S.; Lee, S.C.; Park, S.W.; Choe, Y.H.; Park, P.W.; et al. Assessment of myocardial fibrosis using multimodality imaging in severe aortic stenosis: Comparison with histologic fibrosis. Int. J. Cardiol. 2019, 228, 479–498. [Google Scholar] [CrossRef]
- Diao, K.-Y.; Yang, Z.-G.; Xu, H.-Y.; Liu, X.; Zhang, Q.; Shi, K.; Jiang, L.; Xie, L.-J.; Wen, L.-Y.; Guo, Y.-K. Histologic validation of myocardial fibrosis measured by T1 mapping: A systematic review and meta-analysis. J. Cardiovasc. Magn. Reson. 2016, 18, 92. [Google Scholar] [CrossRef]
- Iles, L.M.; Ellims, A.H.; Llewellyn, H.; Hare, J.L.; Kaye, D.M.; McLean, C.A.; Taylor, A.J. Histological validation of cardiac magnetic resonance analysis of regional and diffuse interstitial myocardial fibrosis. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 14–22. [Google Scholar] [CrossRef]
- Zegard, A.; Okafor, O.; de Bono, J.; Kalla, M.; Lencioni, M.; Marshall, H.; Hudsmith, L.; Qiu, T.; Steeds, R.; Stegemann, B.; et al. Myocardial Fibrosis as a Predictor of Sudden Death in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 2021, 77, 29–41. [Google Scholar] [CrossRef]


| Variables | Isolated AS (n = 43) | AS+IHD (n = 73) | p Value |
|---|---|---|---|
| Gender | |||
| Male | 23 (53.5%) | 45 (61.6%) | NS |
| Female | 20 (46.5%) | 28 (38.4%) | NS |
| Age (year) | 65.5 ± 9.5 | 70.1 ± 9.6 | <0.05 |
| BMI (kg/m2) | 28.76 ± 5.4 | 28.98 ± 5.4 | NS |
| BSA (m2) | 1.9 ± 0.3 | 1.9 ± 0.3 | NS |
| Onset of symptoms (months) | 8 (1–84) | 7 (0–60) | NS |
| NYHA class | |||
| I | No | 1 (1.4%) | NS |
| II | 21 (48.8%) | 34 (46.6%) | NS |
| III | 22 (51.2%) | 37 (50.7%) | NS |
| IV | No | 1 (1.4%) | NS |
| Severity of aortic valve pathology | |||
| severe | 40 (93.1%) | 55 (75.4%) | <0.05 |
| moderate | 3 (6.9%) | 18 (24.6%) | <0.05 |
| AH | 34 (79.1%) | 62 (84.9%) | NS |
| STS score (%) | 1.23 (0.38–11.48) | 2.62 (0.52–23.5) | NS |
| EuroScore II (%) | 1.6 (0.50–23.80) | 3.8 (0.80–42.40) | NS |
| Hospital stay (days) | 13 (7–98) | 14 (8–133) | NS |
| Follow-up period (months) | 7.0 ± 1.9 | 6.6 ± 2.1 | NS |
| Variables | Isolated AS (n = 43) | AS+IHD (n = 73) | p Value |
|---|---|---|---|
| Preoperative data | |||
| Vmax (m/s) | 4.63 ± 0.79 | 4.24 ± 0.96 | <0.05 |
| Gmax (mmHg) | 88.1 ± 29.5 | 73.9 ± 33.6 | <0.05 |
| Gmean (mmHg) | 52.9 ± 20.8 | 44.4 ± 19.9 | <0.05 |
| EOA (cm2) | 0.93 ± 0.27 | 0.91 ± 0.31 | NS |
| EOAi (cm2/m2) | 0.47 ± 0.14 | 0.46 ± 0.15 | NS |
| Early postoperative data | |||
| Vmax (m/s) | 1.94 ± 0.50 ‡‡ | 1.88 ± 0.42 ‡‡ | NS |
| Gmax (mmHg) | 16.9 ± 9.1 ‡‡ | 15.6 ± 7.4 ‡‡ | NS |
| Gmean (mmHg) | 9.7 ± 5.6 ‡‡ | 7.9 ± 4.7 ‡‡ | NS |
| EOA (cm2) | 3.07 ± 0.64 ‡‡ | 2.51 ± 0.64 ‡‡ | <0.01 |
| EOAi (cm2/m) | 1.54 ± 0.38 ‡‡ | 1.31 ± 0.32 ‡‡ | <0.01 |
| Follow-up data | |||
| Vmax (m/s) | 1.91 ± 0.45 ‡‡ | 1.79 ± 0.41 ‡‡ | NS |
| Gmax (mmHg) | 14.9 ± 7.4 ‡‡ | 12.7 ± 4.5 ‡‡ | NS |
| Gmean (mmHg) | 8.5 ± 5.0 ‡‡ | 7.0 ± 3.5 ‡‡ | NS |
| EOA (cm2) | 2.99 ± 0.91 ‡‡ | 2.86 ± 0.86 ‡‡ | NS |
| EOAi (cm2/m2) | 1.51 ± 0.45 ‡‡ | 1.45 ± 0.46 ‡‡ | NS |
| Variables | Isolated AS (n = 43) | AS+IHD (n = 73) | p Value |
|---|---|---|---|
| Preoperative data | |||
| LVEDD (mm) | 50.3 ± 7.7 | 49.7 ± 7.7 | NS |
| LVEDDi (mm/m2) | 25.8 ± 4.2 | 25.7 ± 3.4 | NS |
| LVM (g) | 269.7 ± 72.2 | 267.6 ± 57.1 | NS |
| LVMi (g/m2) | 136.6 ± 35.4 | 137.1 ± 29.3 | NS |
| LVEF (%) | 48.6 ± 11.1 | 48.9 ± 10.0 | NS |
| LV septal thickness (mm) | 14.6 ± 5.4 | 14.0 ± 2.4 | NS |
| LV posterior wall thickness (mm) | 12.3 ± 1.7 | 12.2 ± 1.8 | NS |
| Mitral E velocity (cm/s) | 69.8 ± 25.3 | 76.6 ± 27.5 | NS |
| Mitral E/A | 0.92 ± 0.44 | 1.04 ± 0.61 | NS |
| Mitral E/e’ | 13.3 ± 3.6 | 13.8 ± 6.1 | NS |
| Early postoperative data | |||
| LVEDD (mm) | 49.2 ± 6.1 | 48.4 ± 6.1 | NS |
| LVEDDi (mm/m2) | 25.5 ± 3.0 | 24.8 ± 3.4 † | NS |
| LVM (g) | 244.8 ± 51.9 † | 241.9 ± 61.5 † | NS |
| LVMi (g/m2) | 125.6 ± 24.7 † | 123.3 ± 27.5 ‡‡ | NS |
| LVEF (%) | 48.7 ± 6.7 | 46.8 ± 8.1 † | NS |
| LV septal thickness (mm) | 12.9 ± 1.8 | 13.2 ± 1.8 † | NS |
| LV posterior wall thickness (mm) | 12.1 ± 1.8 | 12.2 ± 1.4 | NS |
| Mitral E velocity (cm/s) | 87.8 ± 22.6 ‡‡ | 88.2 ± 24.9 ‡ | NS |
| Mitral E/A | 1.51 ± 0.39 † | 1.34 ± 0.31 | NS |
| Mitral E/e’ | 12.3 ± 3.9 | 14.2 ± 4.9 | NS |
| Follow-up data | |||
| LVEDD (mm) | 45.1 ± 11.1 ‡ | 47.2 ± 5.7 | NS |
| LVEDDi (mm/m2) | 23.5 ± 4.4 ‡‡ | 23.8 ± 3.4 ‡‡ | NS |
| LVM (g) | 206.3 ± 61.5 ‡‡ | 225.9 ± 52.8 ‡‡ | NS |
| LVMi (g/m2) | 104.3 ± 26.5 ‡‡ | 113.4 ± 23.5 ‡‡ | NS |
| LVEF (%) | 48.9 ± 7.8 | 48.8 ± 6.8 | NS |
| LV septal thickness (mm) | 12.4 ± 2.1 † | 12.8 ± 1.7 † | NS |
| LV posterior wall thickness (mm) | 11.5 ± 1.5 | 12.1 ± 1.3 | NS |
| Mitral E velocity (cm/s) | 79.2 ± 29.3 † | 77.9 ± 29.5 | NS |
| Mitral E/A | 1.15 ± 0.90 | 1.20 ± 0.89 | NS |
| Mitral E/e’ | 10.2 ± 5.7 | 7.4 ± 6.5 ‡‡ | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aitaliyev, S.; Rumbinaitė, E.; Jurenas, M.; Čeponienė, I.; Keturakis, V.; Nekrošius, R.; Orazymbetov, Y.; Benetis, R.; Pangonytė, D. Histologically Validated Myocardial Fibrosis in Relation to Left Ventricular Geometry and Its Function in Aortic Stenosis. Medicina 2024, 60, 667. https://doi.org/10.3390/medicina60040667
Aitaliyev S, Rumbinaitė E, Jurenas M, Čeponienė I, Keturakis V, Nekrošius R, Orazymbetov Y, Benetis R, Pangonytė D. Histologically Validated Myocardial Fibrosis in Relation to Left Ventricular Geometry and Its Function in Aortic Stenosis. Medicina. 2024; 60(4):667. https://doi.org/10.3390/medicina60040667
Chicago/Turabian StyleAitaliyev, Serik, Egle Rumbinaitė, Martynas Jurenas, Indrė Čeponienė, Vytenis Keturakis, Rokas Nekrošius, Yerlan Orazymbetov, Rimantas Benetis, and Dalia Pangonytė. 2024. "Histologically Validated Myocardial Fibrosis in Relation to Left Ventricular Geometry and Its Function in Aortic Stenosis" Medicina 60, no. 4: 667. https://doi.org/10.3390/medicina60040667