
The Effects of Six Weeks Pulmonary Rehabilitation on Functional and Psychological Outcomes in Long-COVID Patients: Preliminary Results from Serbian Single Center Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
2.1. Study Group
2.2. Study Instruments
2.3. Rehabilitation Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guziejko, K.; Tałałaj, J.; Czupryna, P.; Moniuszko-Malinowska, A. Long COVID. Prz. Epidemiol. 2022, 76, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef] [PubMed]
- Haque, A.; Pant, A.B. Long Covid: Untangling the Complex Syndrome and the Search for Therapeutics. Viruses 2022, 15, 42. [Google Scholar] [CrossRef] [PubMed]
- Anaya, J.M.; Rojas, M.; Salinas, M.L.; Rodríguez, Y.; Roa, G.; Lozano, M.; Rodríguez-Jiménez, M.; Montoya, N.; Zapata, E.; Post-COVID study group; et al. Post-COVID syndrome. A case series and comprehensive review. Autoimmun. Rev. 2021, 20, 102947. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.K.; Dehgani-Mobaraki, P. Long Covid. Prog. Mol. Biol. Transl. Sci. 2024, 202, 113–125. [Google Scholar]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875, Erratum in Diabetes Metab. Syndr. 2022, 16, 102504; Erratum in Diabetes Metab. Syndr. 2022, 16, 102660. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.J.; Lin, C.W.; Hsiao, M.Y.; Wang, T.G.; Liang, H.W. Long COVID and rehabilitation. J. Formos. Med. Assoc. 2024, 123 (Suppl. S1), S61–S69. [Google Scholar] [CrossRef] [PubMed]
- NICE. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 9 March 2024).
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Jimeno-Almazán, A.; Franco-López, F.; Buendía-Romero, Á.; Martínez-Cava, A.; Sánchez-Agar, J.A.; Sánchez-Alcaraz Martínez, B.J.; Courel-Ibáñez, J.; Pallarés, J.G. Rehabilitation for post-COVID-19 condition through a supervised exercise intervention: A randomized controlled trial. Scand. J. Med. Sci. Sports 2022, 32, 1791–1801. [Google Scholar] [CrossRef] [PubMed]
- Chetta, A.; Pisi, G.; Aiello, M.; Tzani, P.; Olivieri, D. The walking capacity assessment in the respiratory patient. Respiration 2009, 77, 361–367. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117, Erratum in Am. J. Respir. Crit. Care Med. 2016, 193, 1185. [Google Scholar]
- Matos Casano, H.A.; Anjum, F. Six-Minute Walk Test. [Updated 2023 Aug 14]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK576420/ (accessed on 20 February 2024).
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef]
- Pereira, M.C.; Lima, L.N.G.; Moreira, M.M.; Mendes, F.A.R. One minute sit-to-stand test as an alternative to measure functional capacity in patients with pulmonary arterial hypertension. J. Bras. Pneumol. 2022, 48, e20210483. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, T.; de Bisschop, C.; Beaumont, M.; Ouksel, H.; Jean, V.; Dessables, F.; Chambellan, A. Is the 1-minute sit-to-stand test a good tool for the evaluation of the impact of pulmonary rehabilitation? Determination of the minimal important difference in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2609–2616. [Google Scholar] [CrossRef]
- Heller, G.Z.; Manuguerra, M.; Chow, R. How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance. Scand. J. Pain 2016, 13, 67–75. [Google Scholar] [CrossRef]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients With Low Back Pain: A Systematic Review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef]
- Ries, A.L. Minimally clinically important difference for the UCSD Shortness of Breath Questionnaire, Borg Scale, and Visual Analog Scale. COPD 2005, 2, 105–110. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef]
- Toussaint, A.; Hüsing, P.; Gumz, A.; Wingenfeld, K.; Härter, M.; Schramm, E.; Löwe, B. Sensitivity to change and minimal clinically important difference of the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). J. Affect. Disord. 2020, 265, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Clinical Procedures for Safer Patient Care. Doyle and McCutcheon. British Columbia Institute of Technology. Libre Texts. Available online: https://med.libretexts.org/Bookshelves/Nursing/Clinical_Procedures_for_Safer_Patient_Care_(Doyle_and_McCutcheon)/05%3A_Oxygen_Therapy/5.04%3A_Signs_and_Symptoms_of_Hypoxia#:~:text=Oxygen%20saturation%20levels%20should%20be,than%2088%25%20is%20considered%20hypoxic (accessed on 4 March 2024).
- Gosselink, R.; De Vos, J.; van den Heuvel, S.P.; Segers, J.; Decramer, M.; Kwakkel, G. Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur. Respir. J. 2011, 37, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Dierckx, W.; De Backer, W.; De Meyer, Y.; Lauwers, E.; Franck, E.; De Backer, J.; Ides, K. Personalized pulmonary rehabilitation program for patients with post-acute sequelae of COVID-19: A proof-of-concept retrospective study. Physiol. Rep. 2024, 12, e15931. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Mustafaoglu, R.; Yeldan, I.; Yasaci, Z.; Erhan, B. Effect of Pulmonary Rehabilitation Approaches on Dyspnea, Exercise Capacity, Fatigue, Lung Functions, and Quality of Life in Patients With COVID-19: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 2051–2062. [Google Scholar] [CrossRef]
- Kunoor, A.; Surendran, D.; Hari, H.; Viswan, V.; Harikrishnan, K.; Mehta, A.A. Impact of early pulmonary rehabilitation in postacute COVID Disease: A single-center experience from India—A quasi-experimental study. Indian J. Public Health 2022, 66, S51–S55. [Google Scholar] [CrossRef]
- Nopp, S.; Moik, F.; Klok, F.A.; Gattinger, D.; Petrovic, M.; Vonbank, K.; Koczulla, A.R.; Ay, C.; Zwick, R.H. Outpatient Pulmonary Rehabilitation in Patients with Long COVID Improves Exercise Capacity, Functional Status, Dyspnea, Fatigue, and Quality of Life. Respiration 2022, 101, 593–601. [Google Scholar] [CrossRef]
- Oliveira, M.R.; Hoffman, M.; Jones, A.W.; Holland, A.E.; Borghi-Silva, A. Effect of Pulmonary Rehabilitation on Exercise Capacity, Dyspnea, Fatigue, and Peripheral Muscle Strength in Patients With Post-COVID-19 Syndrome: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2024; ahead of print. [Google Scholar]
- Nair, S.P.; Augustine, A.; Panchabhai, C.; Patil, S.; Parmar, K.; Panhale, V.P. Safety and feasibility of pulmonary rehabilitation in patients hospitalized with post-COVID-19 fibrosis: A feasibility study. PM R, 2023; ahead of print. [Google Scholar] [CrossRef]
- Martínez-Pozas, O.; Meléndez-Oliva, E.; Rolando, L.M.; Rico, J.A.Q.; Corbellini, C.; Sánchez Romero, E.A. The pulmonary rehabilitation effect on long covid-19 syndrome: A systematic review and meta-analysis. Physiother. Res. Int. 2024, 29, e2077. [Google Scholar] [CrossRef]
- Moine, E.; Molinier, V.; Castanyer, A.; Calvat, A.; Coste, G.; Vernet, A.; Faugé, A.; Magrina, P.; Aliaga-Parera, J.L.; Oliver, N.; et al. Safety and Efficacy of Pulmonary Rehabilitation for Long COVID Patients Experiencing Long-Lasting Symptoms. Int. J. Environ. Res. Public Health 2024, 21, 242. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Parameters | Values |
|---|---|
| Age (years), (MV ± SD) | 54.87 ± 13.78 |
| Gender: males/females, N(%) | 26 (56.5%)/20 (43.5%) |
| Body mass index, M (25–75% IQR) | 27.38 (25.67–32.75) |
| Outpatient hospitalization length (days), M (25–75% IQR) | 14 (7–22) |
| SpO2 on admission on initial hospitalization due to COVID-19, M (25–75% IQR) | 90.0 (83.5–96.0) |
| Oxygen support, N (%) | 35 (76.1%) |
| CT score, M (25–75% IQR) | 14 (11–18) |
| Respiratory insufficiency, N (%) | 21 (45.7%) |
| Malignancy, N (%) | 5 (10.9%) |
| Obesity, N (%) | 8 (17.4%) |
| Diabetes mellitus, N (%) | 9 (19.6%) |
| Diabetes mellitus complications, N (%) | 4 (8.7%) |
| Number of comorbidities, M (25–75% IQR) | 2 (1–2) |
| Pulmonary comorbidity, N (%) | 12 (26.1%) |
| Cardiovascular comorbidity, N (%) | 28 (60.8%) |
| Endocrinological comorbidities, N (%) | 13 (28.3%) |
| Psychiatric comorbidities, N (%) | 2 (4.3%) |
| Complications, N (%) | 14 (30.4%) |
| Pulmonary thromboembolism, N (%) | 5 (10.9%) |
| Pneumomediastinum, N (%) | 4 (8.7%) |
| Pneumothorax, N (%) | 2 (4.3%) |
| Sepsis, N (%) | 3 (6.5%) |
| Physical therapy duration on initial hospitalization due to COVID-19 (days), M (25–75% IQR) | 35.5 (25.5–47.75) |
| CURB-65, M (25–75% IQR) | 1 (1–2) |
| Outpatient Rehabilitation Program | ||||||
|---|---|---|---|---|---|---|
| Tested Variables M (25–75% IQR) | Admission | Discharge | ||||
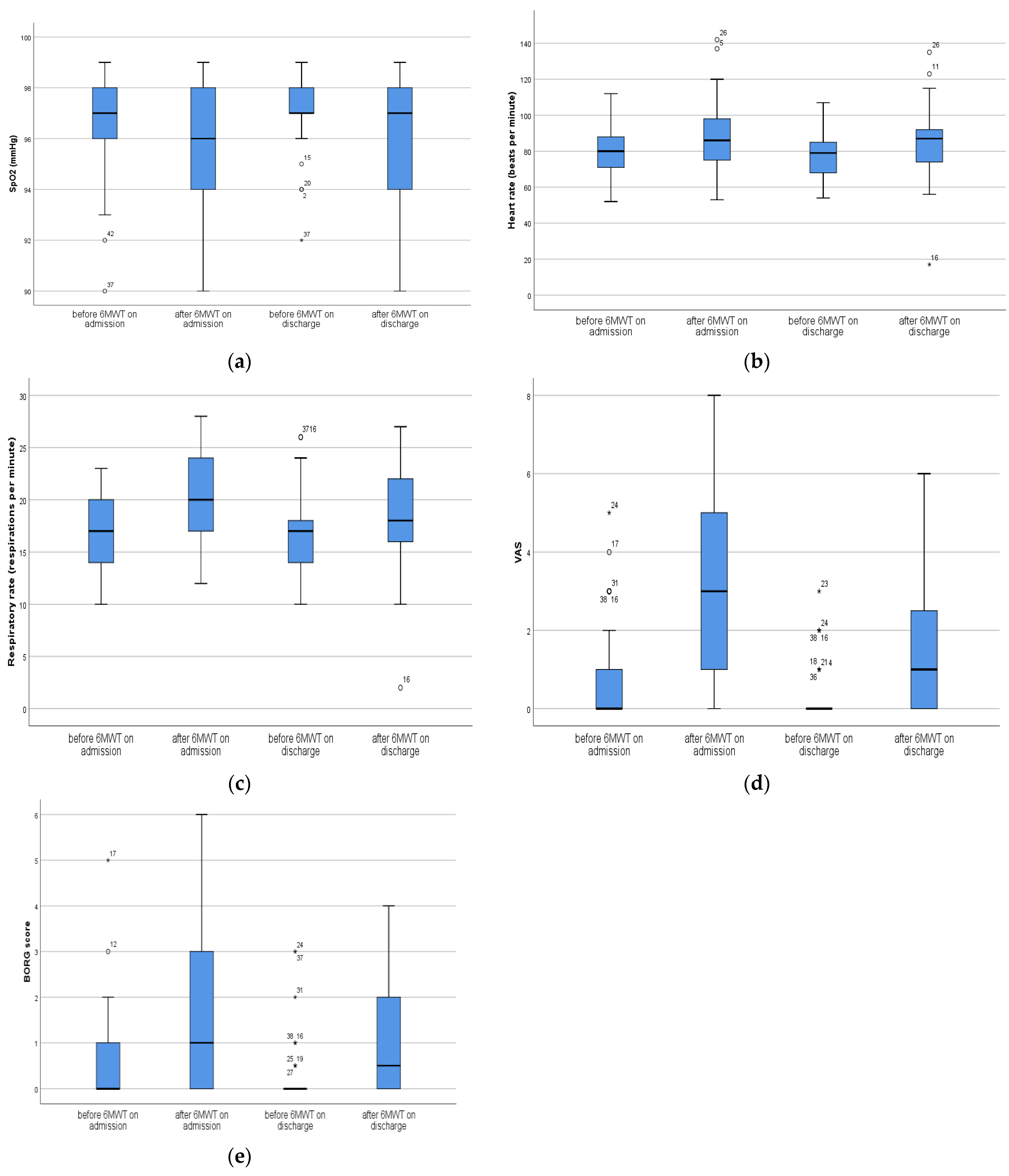
| 6 MWT | ||||||
| Before Testing | After Testing | p * Value | Before Testing | After Testing | p * Value | |
| SpO2 | 97 (96–98) | 96 (94–98) | 0.083 | 97 (97–98) | 97 (94–98) | <0.001 |
| Heart rate | 80 (71–88) | 86 (74.5–99.5) | <0.001 | 79 (67.5–85.5) | 87 (74–92) | <0.001 |
| RR | 17 (14–20) | 20 (17–24) | <0.001 | 17 (13.5–18.5) | 18 (16–22) | <0.001 |
| VAS | 0 (0–1) | 3 (1–5) | <0.001 | 0 (0–0) | 1 (0–2.5) | <0.001 |
| Borg score | 0 (0–1) | 1 (0–3) | <0.001 | 0 (0–0.25) | 0.5 (0–2) | <0.001 |
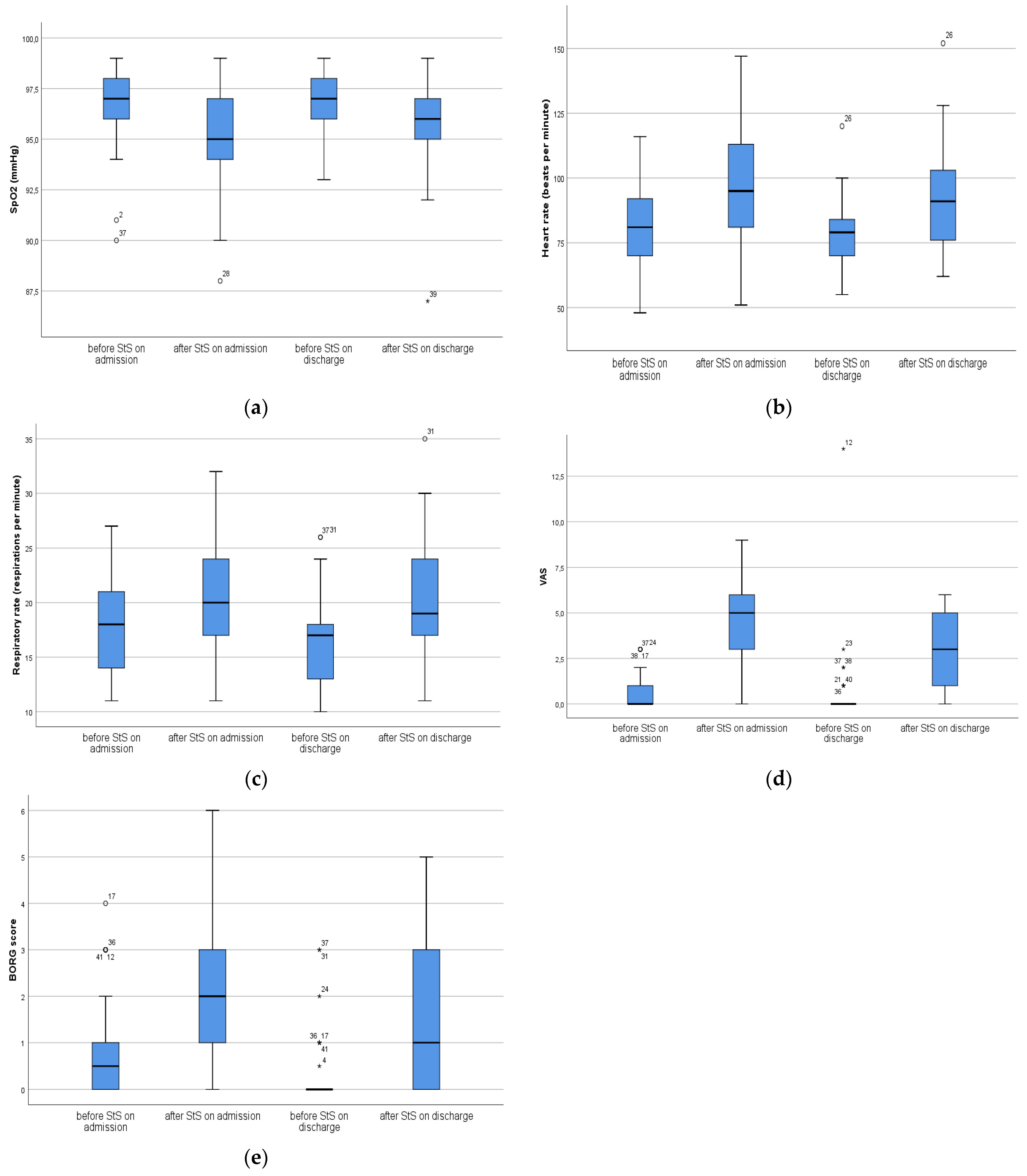
| StS test | ||||||
| Before Testing | After Testing | p * Value | Before Testing | After Testing | p * Value | |
| SpO2 | 97 (96–98) | 95 (94–97.5) | <0.001 | 97 (96–98) | 96 (95–97) | <0.001 |
| Heart rate | 81 (68.5–92) | 95 (81–113.5) | <0.001 | 79 (68.5–84.5) | 91 (76–104) | <0.001 |
| RR | 18 (14–21.5) | 20 (17–24) | <0.001 | 17 (13–18) | 19 (17–24) | <0.001 |
| VAS | 0 (0–1) | 5 (3–6) | <0.001 | 0 (0–0) | 3 (1–5) | <0.001 |
| Borg score | 0.5 (0–1) | 2 (1–3) | <0.001 | 0 (0–0) | 1 (0–3) | <0.001 |
| Outpatient Rehabilitation Program | ||||
|---|---|---|---|---|
| Tested Variables | Admission/Discharge | Admission/Discharge | ||
| 6MWT | StS Test | |||
| p * Value before Testing | p * Value after Testing | p * Value before Testing | p * Value after Testing | |
| SpO2 | 0.007 | 0.914 | 0.143 | 0.036 |
| Heart rate | 0.231 | 0.252 | 0.371 | 0.227 |
| RR | 0.103 | 0.097 | 0.005 | 0.293 |
| VAS | 0.036 | <0.001 | 0.197 | <0.001 |
| Borg score | 0.078 | 0.016 | 0.001 | 0.008 |
| Tested Variables M (25–75% IQR) | Outpatient Rehabilitation Program | ||
|---|---|---|---|
| Admission | Discharge | p * Value | |
| StS test (repetitions) | 24 (18–27.5) | 25 (22–31.5) | 0.011 |
| Distance 6MWT (m) | 506 (462–581) | 588 (504–677) | <0.001 |
| PHQ9 score | 7 (4–10.25) | 3 (1–5) | <0.001 |
| GAD anxiety score | 2.5 (1–5.5) | 2 (0–3) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mujovic, N.; Nikolic, D.; Markovic, F.; Stjepanovic, M.; Zekovic, M.; Ali, H.S.H.; Zivanovic, D.; Savic, M.; Laban, M. The Effects of Six Weeks Pulmonary Rehabilitation on Functional and Psychological Outcomes in Long-COVID Patients: Preliminary Results from Serbian Single Center Study. Medicina 2024, 60, 671. https://doi.org/10.3390/medicina60040671
Mujovic N, Nikolic D, Markovic F, Stjepanovic M, Zekovic M, Ali HSH, Zivanovic D, Savic M, Laban M. The Effects of Six Weeks Pulmonary Rehabilitation on Functional and Psychological Outcomes in Long-COVID Patients: Preliminary Results from Serbian Single Center Study. Medicina. 2024; 60(4):671. https://doi.org/10.3390/medicina60040671
Chicago/Turabian StyleMujovic, Natasa, Dejan Nikolic, Filip Markovic, Mihailo Stjepanovic, Milica Zekovic, Hussain Saleh H. Ali, Dubravka Zivanovic, Milan Savic, and Marija Laban. 2024. "The Effects of Six Weeks Pulmonary Rehabilitation on Functional and Psychological Outcomes in Long-COVID Patients: Preliminary Results from Serbian Single Center Study" Medicina 60, no. 4: 671. https://doi.org/10.3390/medicina60040671