Relationship of Racial Composition and Cancer Risks from Air Toxics Exposure in Memphis, Tennessee, U.S.A.



Abstract
:
1. Introduction

2. Methods
2.1. Data Sources
2.2. Groupings of Racial, SES, and Population Variables
2.3. Geospatially Weighted Regression (GWR) Analysis
3. Results
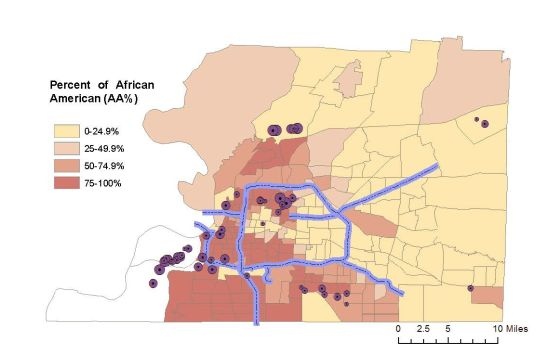
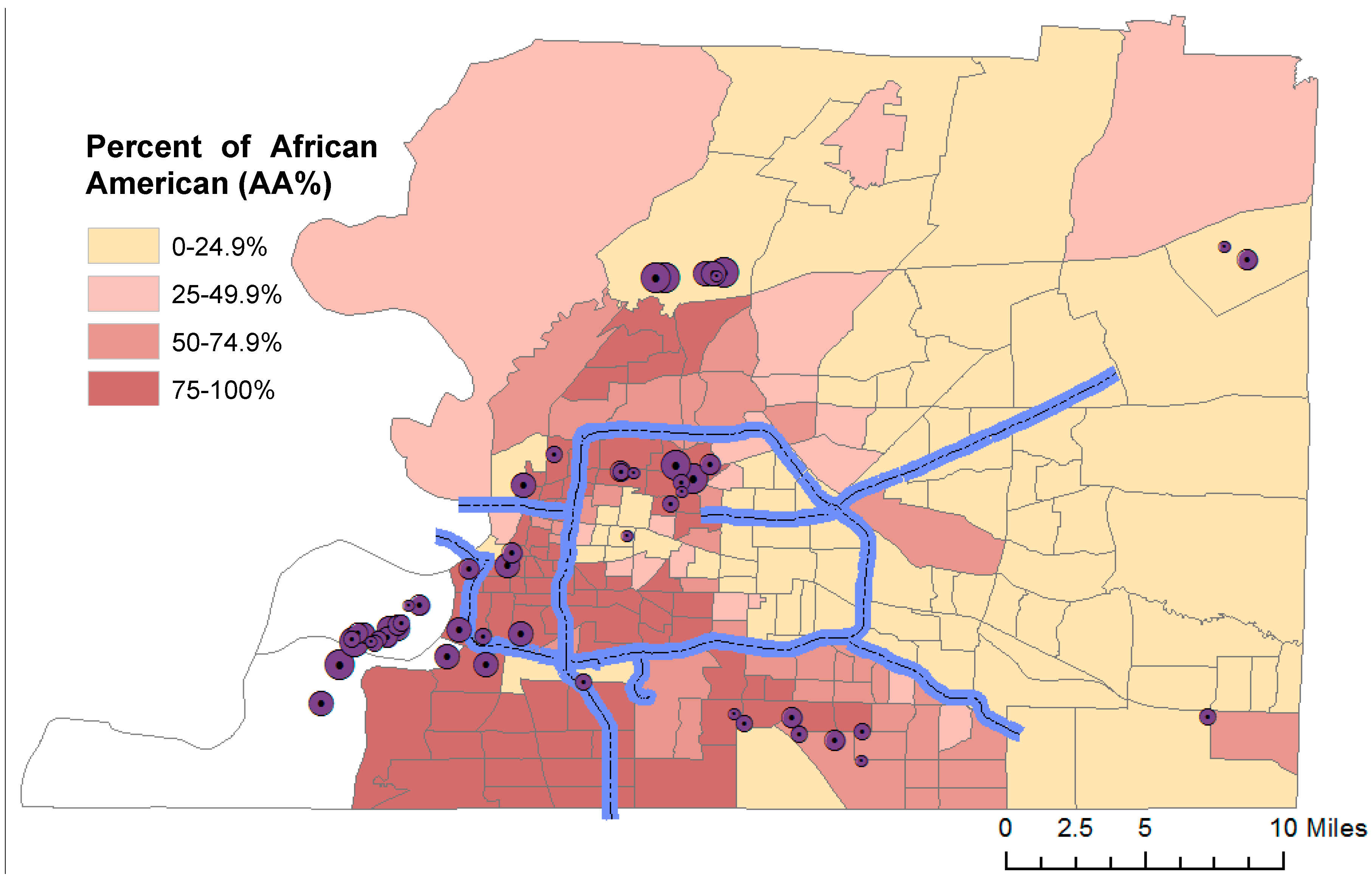
3.1. Higher Cancer Risks in Memphis Populations

{kind=link}
{kind=link}
{kind=link}
| Area | The U.S. | Tennessee | Memphis | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Sample size | (n = 3222) | (n = 95) | (n = 1) | ||||||
| Statistics | Mean | Median | 95th | Mean | Median | 95th | |||
| By source | |||||||||
| Point | 0.54 | 0.17 | 2.09 | 0.73 | 0.24 | 3.64 | 1.12 | ||
| Nonpoint | 2.69 | 1.72 | 9.07 | 1.99 | 1.68 | 4.25 | 3.56 | ||
| On-road | 1.73 | 0.75 | 7.05 | 1.59 | 0.87 | 5.38 | 6.86 | ||
| Non-road | 0.69 | 0.35 | 2.45 | 0.54 | 0.37 | 1.55 | 3.23 | ||
| Background | 7.16 | 6.77 | 11.49 | 7.64 | 7.52 | 11.47 | 10.71 | ||
| Secondary | 17.34 | 16.56 | 28.86 | 23.18 | 23.39 | 27.27 | 29.19 | ||
| Cumulative | 30.16 | 28.96 | 50.97 | 35.67 | 34.49 | 50.39 | 54.68 | ||
| By compound | |||||||||
| Formaldehyde | 15.88 | 15.14 | 26.64 | 20.31 | 20.29 | 24.54 | 28.69 | ||
| Benzene | 3.21 | 2.82 | 7.80 | 3.31 | 2.98 | 7.90 | 8.18 | ||
| Acetaldehyde | 2.78 | 2.66 | 4.59 | 3.78 | 3.80 | 4.40 | 4.73 | ||
| Carbon tetrachloride | 2.85 | 2.85 | 2.87 | 2.85 | 2.86 | 2.88 | 2.86 | ||
| 1,3-Butadiene | 0.61 | 0.45 | 1.80 | 0.54 | 0.45 | 1.38 | 1.68 | ||
| Arsenic | 0.73 | 0.39 | 2.04 | 0.54 | 0.40 | 1.56 | 1.56 | ||
| Naphthalene | 0.62 | 0.38 | 2.06 | 0.49 | 0.41 | 1.08 | 1.21 | ||
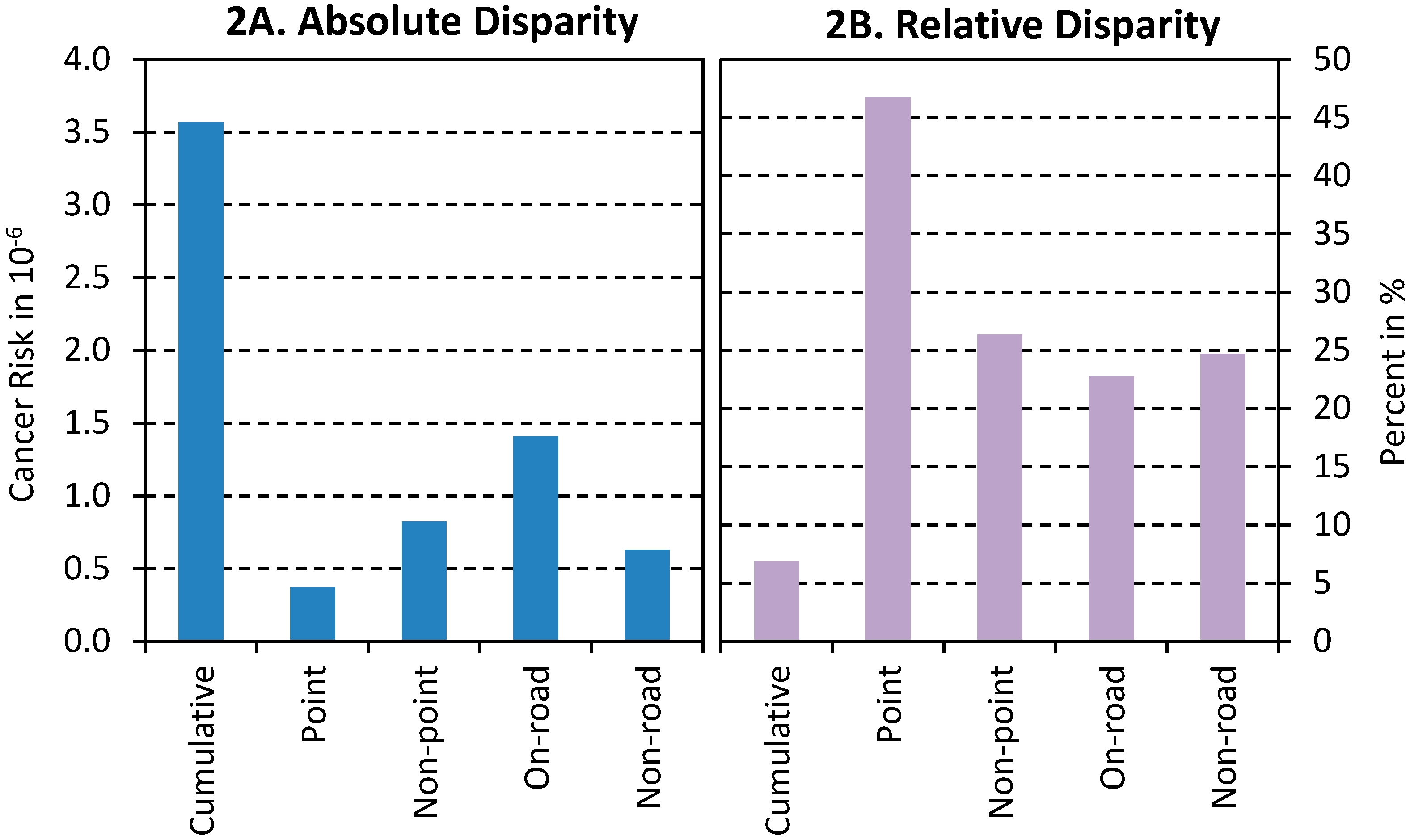
3.2. Significant Racial Disparities in Cancer Risks
| Risk Sources | AA% | p-Value | Popden | p-Value | R2 | Moran’s I | ||
|---|---|---|---|---|---|---|---|---|
| Point | 0.512 | <0.001 | −0.012 | 0.370 | 0.73 | 0.232 | ||
| Nonpoint | 0.235 | 0.003 | 0.063 | 0.000 | 0.54 | 0.597 | ||
| On-road | 0.300 | 0.009 | 0.053 | <0.001 | 0.64 | 0.178 | ||
| Non-road | 0.256 | 0.001 | 0.055 | <0.001 | 0.75 | 0.024 | ||
| Cumulative | 0.084 | 0.001 | 0.013 | <0.001 | 0.68 | 0.343 |

3.3. Higher Risks in More Densely Populated Areas
4. Discussion
4.1. Risk Perception and Disparity Contributors
4.2. Implications and Future Research
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- U.S. Census Bureau 2010 Census, American Fact Finder. Available online: http://factfinder2.census.gov/faces/nav/jsf/pages/index.xhtml (accessed on 28 December 2012).
- Whitman, S.; Orsi, J.; Hurlbert, M. The racial disparity in breast cancer mortality in the 25 largest cities in the United States. Cancer Epidemiol. 2012, 36, E147–E151. [Google Scholar]
- Meyer, P.A.; Yoon, P.W.; Kaufmann, R.B. CDC Health Disparities and Inequalities Report—United States, 2013; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013. [Google Scholar]
- Kjellstrom, T.; Friel, S.; Dixon, J.; Corvalan, C.; Rehfuess, E.; Campbell-Lendrum, D.; Gore, F.; Bartram, J. Urban environmental health hazards and health equity. J. Urban Health 84 (Suppl 1), 86–97.
- Health Power Health Information and Promotion for Multicultural or Minority Health. Available online: http://healthpowerforminorities.com/cities/Memphis-TN.html (accessed on 15 October 2013).
- Shah, P.S.; Balkhair, T.; Knowledge Synthesis Group on Determinants of Preterm/LBW births. Air pollution and birth outcomes: A systematic review. Environ. Int. 2011, 37, 498–516. [Google Scholar] [CrossRef]
- Tzivian, L. Outdoor air pollution and asthma in children. J. Asthma 2011, 48, 470–481. [Google Scholar] [CrossRef]
- Nelin, T.D.; Joseph, A.M.; Gorr, M.W.; Wold, L.E. Direct and indirect effects of particulate matter on the cardiovascular system. Toxicol. Lett. 2012, 208, 293–299. [Google Scholar] [CrossRef]
- Pelucchi, C.; Negri, E.; Gallus, S.; Boffetta, P.; Tramacere, I.; La Vecchia, C. Long-term particulate matter exposure and mortality: A review of European epidemiological studies. BMC Public Health 2009, 9. [Google Scholar]
- U.S. EPA. Toxics Release Inventory. Available online: http://iaspub.epa.gov/triexplorer/tri_release.chemical (accessed on 29 December 2012).
- Daniels, G.; Friedman, S. Spatial inequality and the distribution of industrial toxic releases: Evidence from the 1990 TRI. Soc. Sci. Q. 1999, 80, 244–262. [Google Scholar]
- U.S. Census Bureau. U.S. Census Bureau State & County QuickFacts. Available online: http://quickfacts.census.gov/qfd/states/47/47157.html (accessed on 20 October 2013).
- Green, D.P.; Strolovitch, D.Z.; Wong, J.S. Defended neighborhoods, integration, and racially motivated crime. Am. J. Sociol. 1998, 104, 372–403. [Google Scholar]
- Eastern Research Group, Inc. Results of the 2005 NATA Model-to-Monitor Comparison, Final Report; Eastern Research Group, Inc.: Morrisville, NC, USA, 2010. Available online: http://www.epa.gov/ttn/atw/nata2005/05pdf/nata2005_model2monitor.pdf (accessed on 22 March 2013).
- ICF International. An Overview of Methods for EPA’s National-Scale Air Toxics Assessment; ICF International: Durham, NC, USA, 2011. [Google Scholar]
- James, W.; Jia, C.; Kedia, S. Uneven magnitude of disparities in cancer risks from air toxics. Int. J. Environ. Res. Public Health 2012, 9, 4365–4385. [Google Scholar] [CrossRef]
- Apelberg, B.J.; Buckley, T.J.; White, R.H. Socioeconomic and racial disparities in cancer risk from air toxics in Maryland. Environ. Health Perspect. 2005, 113, 693–699. [Google Scholar] [CrossRef]
- Linder, S.H.; Marko, D.; Sexton, K. Cumulative cancer risk from air pollution in Houston: Disparities in risk burden and social disadvantage. Environ. Sci. Technol. 2008, 42, 4312–4322. [Google Scholar] [CrossRef]
- U.S. EPA. 2005 National-Scale Air Toxics Assessment. Available online: http://www.epa.gov/ttn/atw/nata2005/tables.html (accessed on 18 December 2012).
- U.S. Census Bureau. TIGER/Line® Shapefiles and TIGER/Line® Files. Available online: https://www.census.gov/geo/maps-data/data/tiger-line.html (accessed on 20 July 2013).
- U.S. EPA. NATA: Glossary of Key Terms. Available online: http://www.epa.gov/ttn/atw/natamain/gloss1.html#atmospheric (accessed on 6 July 2014).
- Chakraborty, J. Automobiles, air toxics, and adverse health risks: Environmental inequities in Tampa Bay, Florida. Ann. Assoc. Am. Geogr. 2009, 99, 674–697. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Batterman, S.A. Proximity of schools in Detroit, Michigan to automobile and truck traffic. J. Expo. Sci. Environ. Epidemiol. 2006, 16, 457–470. [Google Scholar] [CrossRef]
- U.S. EPA. Role of the Baseline Risk Assessment in Superfund Remedy Selection Decisions; U.S. Environmental Protection Agency: Washington, DC, USA, 1991. [Google Scholar]
- Parrish, D.D.; Ryerson, T.B.; Mellqvist, J.; Johansson, J.; Fried, A.; Richter, D.; Walega, J.G.; Washenfelder, R.A.; de Gouw, J.A.; Peischl, J.; et al. Primary and secondary sources of formaldehyde in urban atmospheres: Houston Texas region. Atmos. Chem. Phys. 2012, 12, 3273–3288. [Google Scholar] [CrossRef]
- Abel, T.D. Skewed riskscapes and environmental injustice: A case study of metropolitan St. Louis. Environ. Manag. 2008, 42, 232–248. [Google Scholar] [CrossRef]
- Marshall, J.D. Environmental inequality: Air pollution exposures in California’s south coast air basin. Atmos. Environ. 2008, 42, 5499–5503. [Google Scholar] [CrossRef]
- Morello-Frosch, R.; Jesdale, B.M. Separate and unequal: Residential segregation and estimated cancer risks associated with ambient air toxics in US metropolitan areas. Environ. Health Perspect. 2006, 114, 386–393. [Google Scholar] [CrossRef]
- Zoll, M.H.; Boyce, J.K. The New Environmental Activists: Fighting Pollution, Poverty, and Racism by Building Natural Assets; Political Economy Research Institute: Amherst, MA, USA, 2003; pp. 50–51. [Google Scholar]
- U.S. EPA. 2012 Toxics Release Inventory National Analysis Overview; U.S. Environmental Protection Agency: Washington, DC, USA, 2014. [Google Scholar]
- Charlier, T. Environmental racism not clear-cut issue in Memphis. Memphis Commercial Appeal, 19 September 1993; A1. [Google Scholar]
- Healthy Memphis Common Table. Status Report on Efforts to Advance Health Equity in Clinical Care and Health Outcomes in Memphis and Shelby County, Tennessee. Healthy Memphis Common Table: Memphis, TN, USA, 2011. Available online: http://healthcarequalitymatters.org/assets/2011_HMCT_Equity_Report.pdf (accessed on 24 October 2013).
- Payne-Sturges, D.; Gee, G.C. National environmental health measures for minority and low-income populations: Tracking social disparities in environmental health. Environ. Res. 2006, 102, 154–171. [Google Scholar] [CrossRef]
- Lopez, R. Segregation and Black/White differences in exposure to air toxics in 1990. Environ. Health Perspect. 2002, 110, 289–295. [Google Scholar] [CrossRef]
- Gee, G.C.; Payne-Sturges, D.C. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environ. Health Perspect. 2004, 112, 1645–1653. [Google Scholar] [CrossRef]
- Adamkiewicz, G.; Zota, A.R.; Fabian, M.P.; Chahine, T.; Julien, R.; Spengler, J.D.; Levy, J.I. Moving environmental justice indoors: Understanding structural influences on residential exposure patterns in low-income communities. Am. J. Public Health 2011, 101, S238–S245. [Google Scholar] [CrossRef]
- HUD, 2012–2015 Environmental Justice Strategy; U.S. Department of Housing and Urban Development: Washington, DC, USA, 2012.
Appendix
| Variables | Unit | Factor 1 | Factor 2 |
|---|---|---|---|
| Median household income | (× $1000) | −0.92 | 0.02 |
| Poverty percent | (%) | 0.89 | −0.13 |
| Median house value | (× $1000) | −0.69 | −0.28 |
| Percent of blacks | (%) | 0.87 | 0.17 |
| Percent of females headed house | (%) | 0.94 | 0.08 |
| Percent less than high school degree | (%) | 0.92 | −0.16 |
| Total population | (Person) | −0.38 | 0.69 |
| Percent of age >65 | (%) | 0.12 | −0.63 |
| Population density | (Person/km2) | 0.42 | 0.50 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Jia, C.; James, W.; Kedia, S. Relationship of Racial Composition and Cancer Risks from Air Toxics Exposure in Memphis, Tennessee, U.S.A. Int. J. Environ. Res. Public Health 2014, 11, 7713-7724. https://doi.org/10.3390/ijerph110807713
Jia C, James W, Kedia S. Relationship of Racial Composition and Cancer Risks from Air Toxics Exposure in Memphis, Tennessee, U.S.A. International Journal of Environmental Research and Public Health. 2014; 11(8):7713-7724. https://doi.org/10.3390/ijerph110807713
Chicago/Turabian StyleJia, Chunrong, Wesley James, and Satish Kedia. 2014. "Relationship of Racial Composition and Cancer Risks from Air Toxics Exposure in Memphis, Tennessee, U.S.A." International Journal of Environmental Research and Public Health 11, no. 8: 7713-7724. https://doi.org/10.3390/ijerph110807713