
Transtheoretical Model of Change during Travel Behavior Interventions: An Integrative Review




Abstract
:1. Introduction
The Transtheoretical Model of Change
2. Materials and Methods
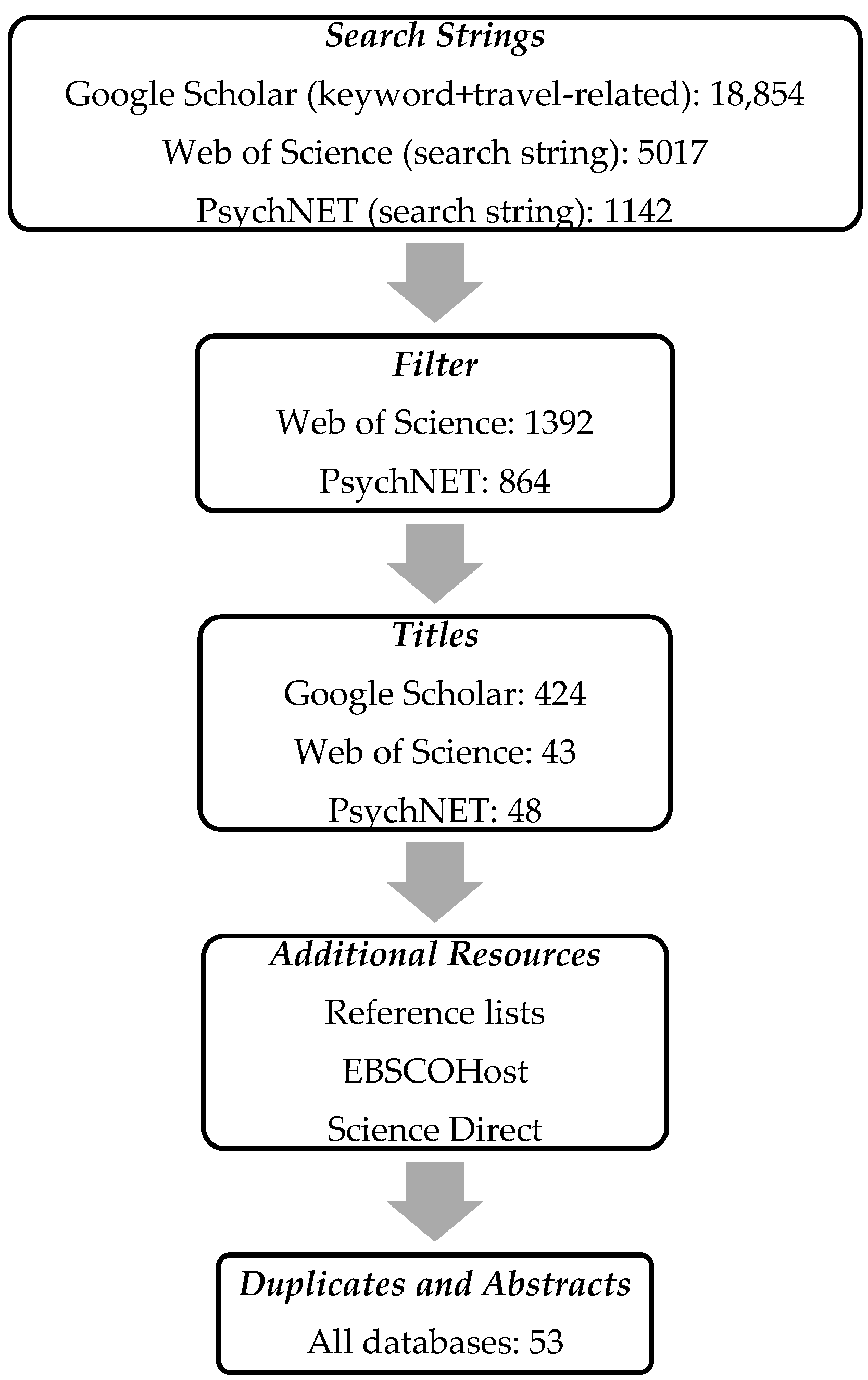
2.1. Integrative Review
2.2. Procedure and Inclusion Criteria
3. Findings
3.1. Classification and Categorization
3.2. Processes and Stages of Change
3.3. Outcome Measures
3.3.1. Travel Behavioral Change
3.3.2. Other Outcome Measures
3.3.3. Summary Outcome Measures
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Prochaska, J.; DiClemente, C. Self change processes, self efficacy and decisional balance across five stages of smoking cessation. Prog. Clin. Biol. Res. 1984, 156, 131–140. [Google Scholar] [PubMed]
- Marlatt, G.A.; Gordon, J.R. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors; Guilford Press: New York, NY, USA, 1985. [Google Scholar]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Nisbet, E.K.L.; Gick, M.L. Can health psychology help the planet? Applying theory and models of health behaviour to environmental actions. Can. Psychol. 2008, 49, 296–303. [Google Scholar] [CrossRef]
- Bird, E.L.; Baker, G.; Mutrie, N.; Ogilvie, D.; Shlqvist, S.; Powell, J. Behavior change techniques used to promote walking and cycling: A systematic review. Health Psychol. 2013, 32, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, S. Is a stage model a useful approach to explain car drivers’ willingness to use public transportation? J. Appl. Soc. Psychol. 2007, 37, 1757–1783. [Google Scholar] [CrossRef]
- Mutrie, N.; Carney, C.; Blamey, A.; Crawford, F.; Aitchison, T.; Whitelaw, A. “Walk in to work out”: A randomised controlled trial of a self help intervention to promote active commuting. J. Epidemiol. Community Health 2002, 56, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Diniz, I.; Duarte, M.; Peres, K.; de Oliveira, E.; Berndt, A. Active commuting by bicycle: Results of an educational intervention study. J. Phys. Act. Health 2015, 12, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Mundorf, N.; Redding, C.A.; Fu, T.; Paiva, A.; Brick, L.; Prochaska, J.O. Promoting sustainable transportation across campus communities using the transtheoretical model of change. Commun. Commons 2013, 427–438. [Google Scholar]
- Crawford, F.; Mutrie, N.; Hanlon, P. Employee attitudes towards active commuting. Int. J. Health Promot. Edu. 2001, 39, 14–20. [Google Scholar] [CrossRef]
- Bartholomew, L.K.K.; Parcel, G.S.S.; Kok, G.; Gottlieb, N.H.H. Planning Health Promotion Programs; Wiley: San Franscisco, CA, USA, 2010. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C.; Norcross, J.C. In search of how people change: Applications to addictive behaviors. Am. Psychol. 1992, 47, 1102–1114. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Holtgrave, D.R.; Tinsley, B.J.; Kay, L.S. Encouraging risk reduction: A decision-making approach to message design. In Designing Health Messages: Approaches from Communication Theory and Public Health Practice; Maibach, E.W., Parrot, R.L., Eds.; Sage: Thousand Oaks, CA, USA, 1995; pp. 24–40. [Google Scholar]
- Maibach, E.W.; Cotton, D. Moving people to behavior change: A staged social—Cognitive approach to message design. In Designing Health Messages: Approaches from Communication Theory and Public Health Practice; Maibach, E.W., Parrot, R.L., Eds.; Sage: Thousand Oaks, CA, USA, 1995; pp. 42–64. [Google Scholar]
- De Vries, H.; Backbier, E. Self-efficacy as an important determinant of quitting among pregnant women who smoke: The ø-pattern. Prev. Med. 1994, 23, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef]
- Kraft, P.; Sutton, S.R.; Reynolds, H.M. The transtheoretical model of behaviour change: Are the stages qualitatively different? Psychol. Health 1999, 14, 433–450. [Google Scholar] [CrossRef]
- Sutton, S. Transtheoretical model applied to smoking cessation. In Understanding and Changing Health Behaviour: From Health Beliefs to Self-Regulation; Abraham, C., Norman, P., Conner, M.E., Eds.; Harwood Academic Publishers: Amsterdam, The Netherlands, 2000; pp. 207–225. [Google Scholar]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Taylor & Francis: New York, NY, USA, 2011. [Google Scholar]
- Fava, J.L.; Velicer, W.F.; Prochaska, J.O. Applying the transtheoretical model to a representative sample of smokers. Addict. Behav. 1995, 20, 189–203. [Google Scholar] [CrossRef]
- Johnson, S.S.; Paiva, A.L.; Cummins, C.O.; Johnson, J.L.; Dyment, S.J.; Wright, J.A.; Prochaska, J.O.; Prochaska, J.M.; Sherman, K. Transtheoretical model-based multiple behavior intervention for weight management: Effectiveness on a population basis. Prev. Med. 2008, 46, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J. A transtheoretical model for assessing organizational change: A study of family service agencies’ movement to time-limited therapy. Fam. Soc. J. Contemp. Soc. Serv. 2000, 81, 76–84. [Google Scholar] [CrossRef]
- Shockey, S.S.; Seiling, S.B. Moving into action: Application of the transtheoretical model of behavior change to financial education. J. Financ. Couns. Plann. 2004, 15, 41–52. [Google Scholar]
- Xiao, J.J.; O’Neill, B.; Prochaska, J.M.; Kerbel, C.M.; Brennan, P.; Bristow, B.J. A consumer education programme based on the transtheoretical model of change. Int. J. Consum. Stud. 2004, 28, 55–65. [Google Scholar] [CrossRef]
- Rose, G.; Marfurt, H. Travel behaviour change impacts of a major ride to work day event. Transp. Res. Part A Policy Pract. 2007, 41, 351–364. [Google Scholar] [CrossRef]
- Gatersleben, B.; Appleton, K.M. Contemplating cycling to work: Attitudes and perceptions in different stages of change. Transp. Res. Part A Policy Pract. 2007, 41, 302–312. [Google Scholar] [CrossRef]
- Cooper, C. Successfully changing individual travel behavior: Applying community-based social marketing to travel choice. Transp. Res. Rec. J. Transp. Res. Board 2007, 2021, 89–99. [Google Scholar] [CrossRef]
- Rissel, C.E.; New, C.; Wen, L.M.; Merom, D.; Bauman, A.E.; Garrard, J. The effectiveness of community-based cycling promotion: Findings from the cycling connecting communities project in Sydney, Australia. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- McKee, R.; Mutrie, N.; Crawford, F.; Green, B. Promoting walking to school: Results of a quasi-experimental trial. J. Epidemiol. Community Health 2007, 61, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, N.; Nagasaki, H.; Ito, H.; Furuna, T. Optimal walking in terms of variability in step length. J. Orthop. Sports Phys. Ther. 1997, 26, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.M.; Orr, N.; Bindon, J.; Rissel, C. Promoting active transport in a workplace setting: Evaluation of a pilot study in Australia. Health Promot. Inter. 2005, 20, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Hemmingsson, E.; Udden, J.; Neovius, M.; Ekelund, U.; Rössner, S. Increased physical activity in abdominally obese women through support for changed commuting habits: A randomized clinical trial. Int. J. Obes. 2009, 33, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Molina-García, J.; Castillo, I.; Queralt, A.; Sallis, J.F. Bicycling to university: Evaluation of a bicycle-sharing program in spain. Health Promot. Inter. 2013, 30, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.; Bopp, M.; Colgan, J.; Sims, D.; Matthews, S.; Rovniak, L.; Poole, E. A social media campaign for promoting active travel to a university campus. J. Healthc. Commun. 2016, 1, 1–6. [Google Scholar] [CrossRef]
- Meloni, I.; Sanjust, B.; Sottile, E.; Cherchi, E. Propensity for voluntary travel behavior changes: An experimental analysis. Procedia—Soc. Behav. Sci. 2013, 87, 31–43. [Google Scholar] [CrossRef]
- Sanjust di Teulada, B.; Meloni, I. Individual Persuasive Eco-travel Technology, a mobile persuasive application for implementing voluntary travel behaviour change programmes. IET Intell. Transp. Syst. 2016, 10, 237–243. [Google Scholar] [CrossRef]
- Weiser, P.; Scheider, S.; Bucher, D.; Kiefer, P.; Raubal, M. Towards sustainable mobility behavior: Research challenges for location-aware information and communication technology. GeoInformatica 2016, 20, 213–239. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Peters, G.J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Peters, G.-J.Y.; de Bruin, M.; Crutzen, R. Everything should be as simple as possible, but no simpler: Towards a protocol for accumulating evidence regarding the active content of health behaviour change interventions. Health Psychol. Rev. 2013, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Processes | Stages | ||||
|---|---|---|---|---|---|
| Precontemplation | Contemplation | Preparation | Action | Maintenance | |
| Consciousness Raising | x | ||||
| Dramatic Relief | x | ||||
| Environmental Reevaluation | x | ||||
| Risk Assessment | x | ||||
| Positive Framing | x | ||||
| Reevaluation of Outcomes | x | ||||
| Perception of Benefits | x | ||||
| Self-Reevaluation | x | ||||
| Self-Efficacy and Social Support | x | ||||
| Decision-Making Perspective | x | ||||
| Tailoring Time Horizons | x | ||||
| Focus on Important Factors | x | ||||
| Trying New Behavior | x | ||||
| Persuasion of Positive Outcomes | x | ||||
| Modeling (Overcoming Barriers) | x | ||||
| Self-Liberation | x | ||||
| Skill Improvement | x | ||||
| Coping with Barriers | x | ||||
| Goal Setting | x | ||||
| Modeling (Social Reinforcement) | x | ||||
| Helping Relationships | x | ||||
| Counterconditioning | x | ||||
| Contingency Management | x | ||||
| Stimulus Control | x | ||||
| Skill Enhancement | x | ||||
| Dealing with Barriers | x | ||||
| Self-Rewards for Success | x | ||||
| Coping Skills | x | ||||
| Keyword | Context (Travel-Related Keywords) |
|---|---|
| TTM | Travel |
| Stage of change | Transport |
| Stages of change | Transit |
| Behavioral change | Cycling |
| Transtheoretical Model | Walk |
| Stage Model of Change | Car |
| Physical activity | |
| Active commuting |
| Author(s) | Transport Mode | Motive | Target Group | Methods | n | Time | Country | Current Mode use | Target Behavior | Use of the TTM | Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cooper (2007) [27] | Car Public Transport | Environment Health | Local community | Quasi-experimental Quantitative Intervention | 1031 | 10 weeks | USA | Habitual car user | Reduced car use | Classification/stages | Stage of change transition |
| Diniz et al. (2015) [9] | Bike | Health Physical activity | Workplace Production industry | Quasi-experimental Quantitative Controlled Intervention | 932 | 6 months | Brazil | Non-bikers | Increased biking | Tailored intervention | Change of commuting behavior |
| Gatersleben & Appleton (2007) [28] | Bike | Sustainability | University | Quasi-experimental Quantitative Intervention (Study 1) Survey (Study 2) | 89 (Study 1) 22 (Study 2) | 2 weeks | UK | Car and public transport users, walkers | Increased biking | Theoretical framework Categorization/strategies | Stage of change transition Motivators and barriers |
| Hemmingsson et al. (2009) [29] | Bike Walk | Health Physical activity | Workplace Health care | Quasi-experimental, Quantitative Controlled Intervention | 120 | 18 months | Sweden | Car and public transport users | Increased everyday activity levels | Tailored intervention | Stage of change transition |
| McKee et al. (2006) [30] | Car Walk | Health Physical activity | School (9–10 years) | Quasi-experimental Mixed Controlled Intervention | 60 | 10 weeks | UK | Habitual car users | Increased walking | Tailored intervention | Stage of change transition Increased walking |
| Meloni et al. (2013) [31] | Car Public Transport | Environment Sustainability | Local community | Descriptive Quantitative Survey and Intervention | 146 | 1 week | Italy | Habitual car users | Increased public transport use | Theoretical framework Classification/stages | Model for voluntary change |
| Molina-Garcia et al. (2013) [32] | Bike | Health Physical activity | University | Cross-sectional, Quantitative Survey and intervention | 173 | 8 weeks | Spain | Car/motorbike/public transport users. Walkers and cyclists | Increased biking | Analytical tool Classification/stages | Increased bike-rentals |
| Mundorf et al. (2013) [10] | Public Transport Bike Walk | Environment Physical activity | University | Quasi-experimental Descriptive Quantitative Survey and Intervention | 588 (Study 1) 1196 (Study 2) 720 (Study 3) 393 (Study 4) | 1 day | USA | Habitual car users | Increased use of alternative transport | Study design Analytical tool Stages of change Decisional balance Self-efficacy Processes of change | Stage of change transition pre-action |
| Mutrie et al. (2002) [7] | Bike Walk | Health Physical activity | Workplace Public sector | Quasi-experimental Descriptive Survey Controlled intervention | 295 | 12 months | UK | Habitual car users | Increased active commuting | Study design Analytical tool Stages of change Decisional balance Self-efficacy Processes of change | Stage of change transition |
| Rissel et al. (2010) [33] | Bike | Environment Health | Local community | Quasi-experimental Quantitative Controlled Intervention | 909 | 24 months | Australia | Biking | Increased biking | Tailored intervention | Stage of change transition Increased biking |
| Rose & Marfurt (2007) [34] | Bike | Environment Sustainability | Local community | Quasi-experimental Quantitative Survey Intervention | 1952 | 1 day + 5-day follow-up | Australia | Car, public transport, biking, walking | Increased biking | Predictive and analytical tool | Stage of change transition |
| Wen et al. (2016) [35] | Public Transport Bike Walk | Health Physical activity | Work place Health care | Quasi-experimental Mixed Controlled Intervention | 68 | 12 months | Australia | Car, active transport (public transport, biking, walking) | Increased physical activity levels Increased biking Increased walking | Tailored intervention | Increased use of active transport. Commuting and leisure activities |
| Wilson et al. (2011) [36] | Bike | Physical activity | University | Descriptive Quantitative Observational intervention-based study | 280 followers | 12 months | USA | Not measured | Increased physical activity levels | Tailored intervention | Increased social media use |
| Stages of the TTM | Processes (Total 28) | Stages of the TTM | Undefined Stage | Process Not Supported | ||||
|---|---|---|---|---|---|---|---|---|
| Precontemplation | Contemplation | Preparation | Action | Maintenance | ||||
| Precontemplation | Consciousness raising | 2 | 11 | 25 | 3 | 3 | 15 | |
| Dramatic relief | 3 | 7 | 5 | |||||
| Environmental reevaluation | 1 | 6 | 5 | |||||
| Risk Assessment | 2 | 3 | 1 | |||||
| Positive framing | 3 | 3 | 1 | |||||
| Reevaluation of outcomes | 2 | 2 | ||||||
| Perception of benefits | 1 | 1 | 1 | |||||
| Contemplation | Self-Reevaluation | 3 | 2 | |||||
| Self-Efficacy and Social Support | 3 | 12 | 7 | |||||
| Decision-Making Perspective | x | |||||||
| Tailoring Time Horizons | 1 | |||||||
| Focus on Important Factors | 1 | 1 | ||||||
| Trying New Behavior | 1 | 6 | 4 | |||||
| Persuasion of Positive Outcomes | 2 | 7 | 3 | |||||
| Modeling to Overcome Barriers | x | |||||||
| Preparation | Self-Liberation | 1 | 5 | 2 | ||||
| Skill Improvement | 7 | 16 | 8 | |||||
| Coping with Barriers | 1 | |||||||
| Goal Setting | 1 | 1 | 1 | |||||
| Modeling Perception/Social Reinforcement | x | |||||||
| Action | Helping Relationships | 1 | 1 | 1 | 1 | |||
| Counterconditioning | 2 | 2 | 1 | 1 | ||||
| Contingency Management | 2 | 2 | ||||||
| Stimulus Control | x | |||||||
| Skill Enhancement | x | |||||||
| Dealing with Barriers | x | |||||||
| Self-Rewards for Success | 1 | |||||||
| Maintenance | Coping Skills | x | ||||||
| Summary | 2 | 44 | 100 | 7 | 7 | 57 | 7 | |
| Car | Public Transport | Bicycle | Walk | Car Pool | Active Transport | |
|---|---|---|---|---|---|---|
| % change in willingness to use a specific mode (n = 4) | ||||||
| n a | 0 | 0 | 2 | 1 | 0 | 1 |
| M | 48% | 72% | 19% | |||
| SD | 20% | na | na | |||
| Min/Max | 29/68 | na | na | |||
| % change in number of trips (n = 4) | ||||||
| n a | 3 | 2 | 2 | 1 | 1 | 0 |
| M | −16.73 | 29.15 | 50.45 | 41 | 44 | |
| SD | 7.56 | 19.15 | 30.55 | na | na | |
| Min/Max | −27.3/−10 | 10/48.3 | 19.9/81 | na | na | |
| % change in main transport mode use (yes/no) (n = 5) | ||||||
| n a | 3 | 2 | 4 | 2 | 0 | 1 |
| M | −6.97 | -14.80 | 10.93 | 8.30 | 7.8 | |
| SD | 0.05 | 0.1 | 0.12 | 0.09 | na | |
| Min/Max | −13.1/0 | −25/−4.6 | −0.6/29.4 | −0.5/17.1 | na | |
| % change in time travelled per transport mode (minutes/day/person) (n = 2) | ||||||
| n a | 0 | 0 | 2 | 1 | 0 | 0 |
| M | 11.75 | 52 | ||||
| SD | 0.12 | na | ||||
| Min/Max | 0/23.5 | na | ||||
| % change in distance traveled per transport mode (meters/day/person) (n = 2) | ||||||
| n a | 1 | 0 | 1 | 2 | 0 | 0 |
| M | −54 | 38 | 153.21 | |||
| SD | na | na | 1.37 | |||
| Min/Max | na | na | 16.53/289.9 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friman, M.; Huck, J.; Olsson, L.E. Transtheoretical Model of Change during Travel Behavior Interventions: An Integrative Review. Int. J. Environ. Res. Public Health 2017, 14, 581. https://doi.org/10.3390/ijerph14060581
Friman M, Huck J, Olsson LE. Transtheoretical Model of Change during Travel Behavior Interventions: An Integrative Review. International Journal of Environmental Research and Public Health. 2017; 14(6):581. https://doi.org/10.3390/ijerph14060581
Chicago/Turabian StyleFriman, Margareta, Jana Huck, and Lars E. Olsson. 2017. "Transtheoretical Model of Change during Travel Behavior Interventions: An Integrative Review" International Journal of Environmental Research and Public Health 14, no. 6: 581. https://doi.org/10.3390/ijerph14060581
APA StyleFriman, M., Huck, J., & Olsson, L. E. (2017). Transtheoretical Model of Change during Travel Behavior Interventions: An Integrative Review. International Journal of Environmental Research and Public Health, 14(6), 581. https://doi.org/10.3390/ijerph14060581