Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Group A (Drill)
2.1.1. Clinical Observation
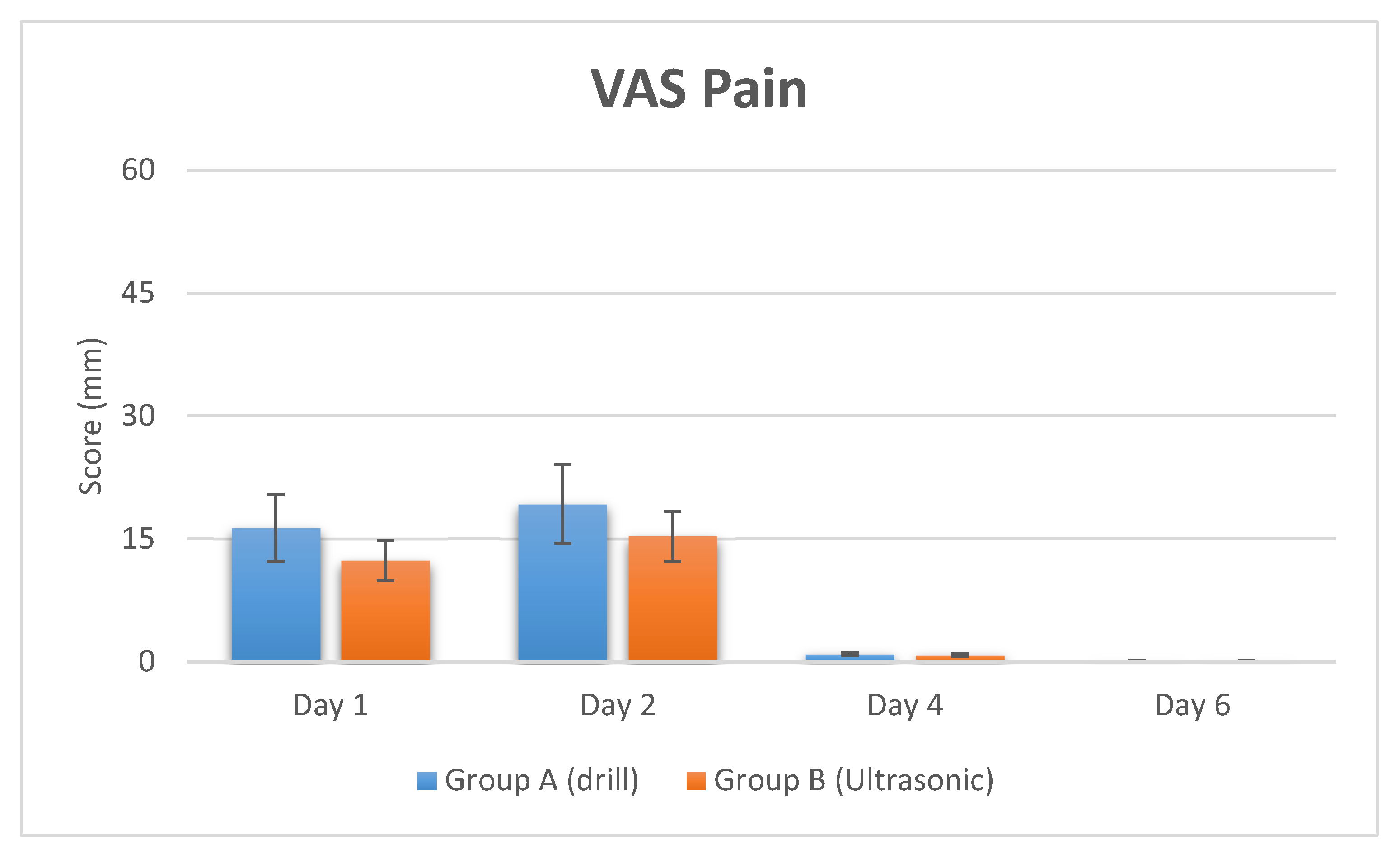
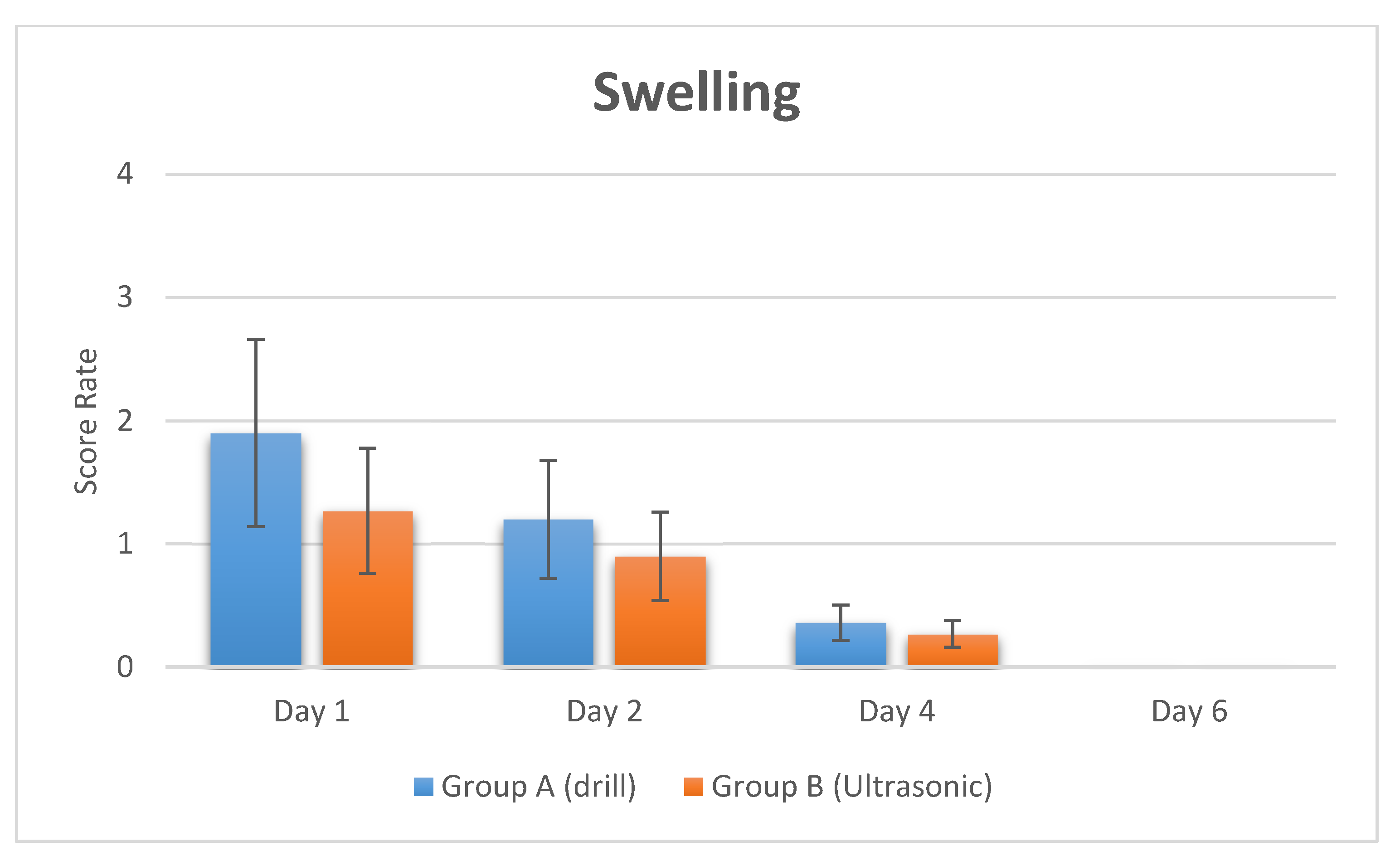
2.1.2. Pain and Swelling Intensity Evaluation
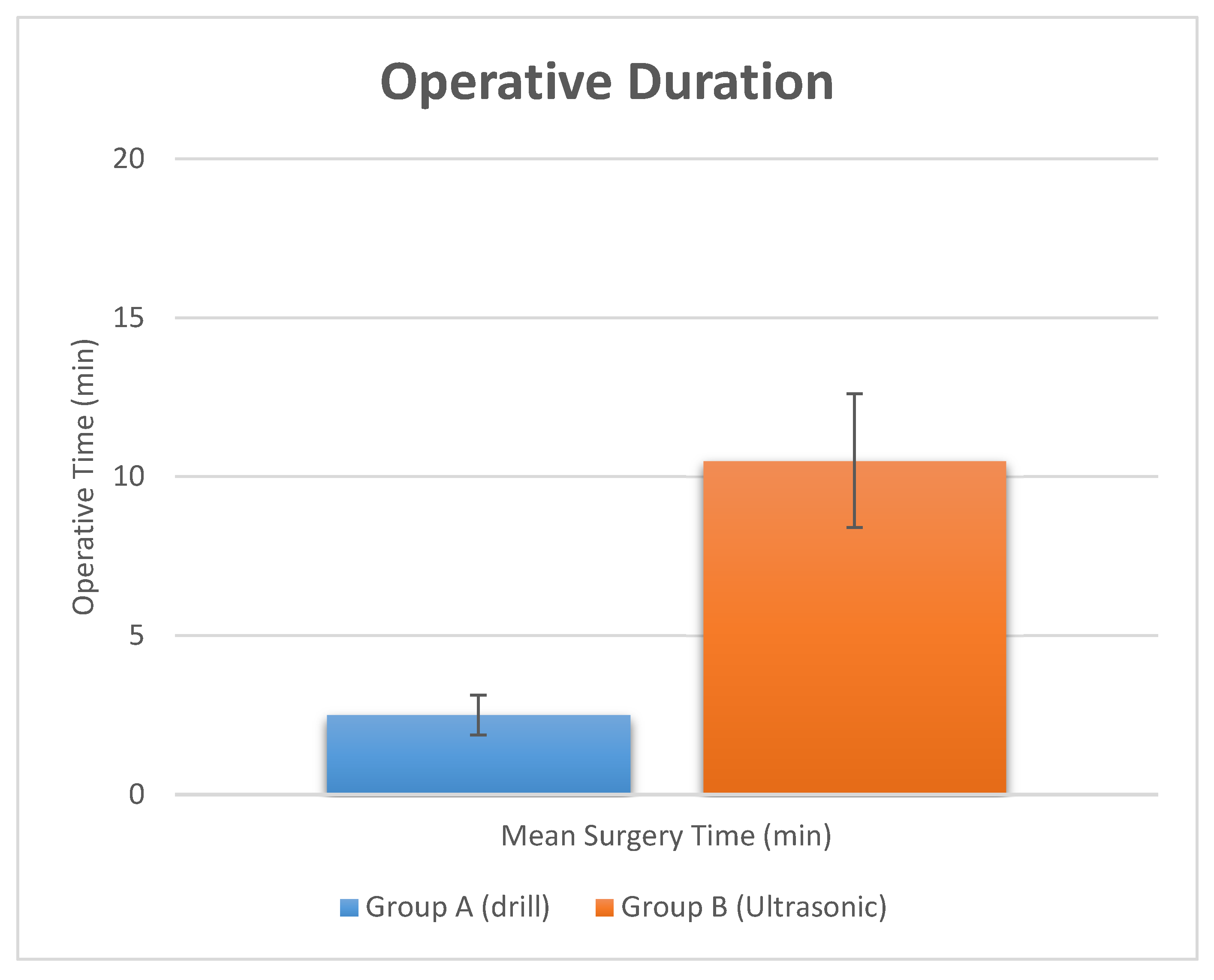
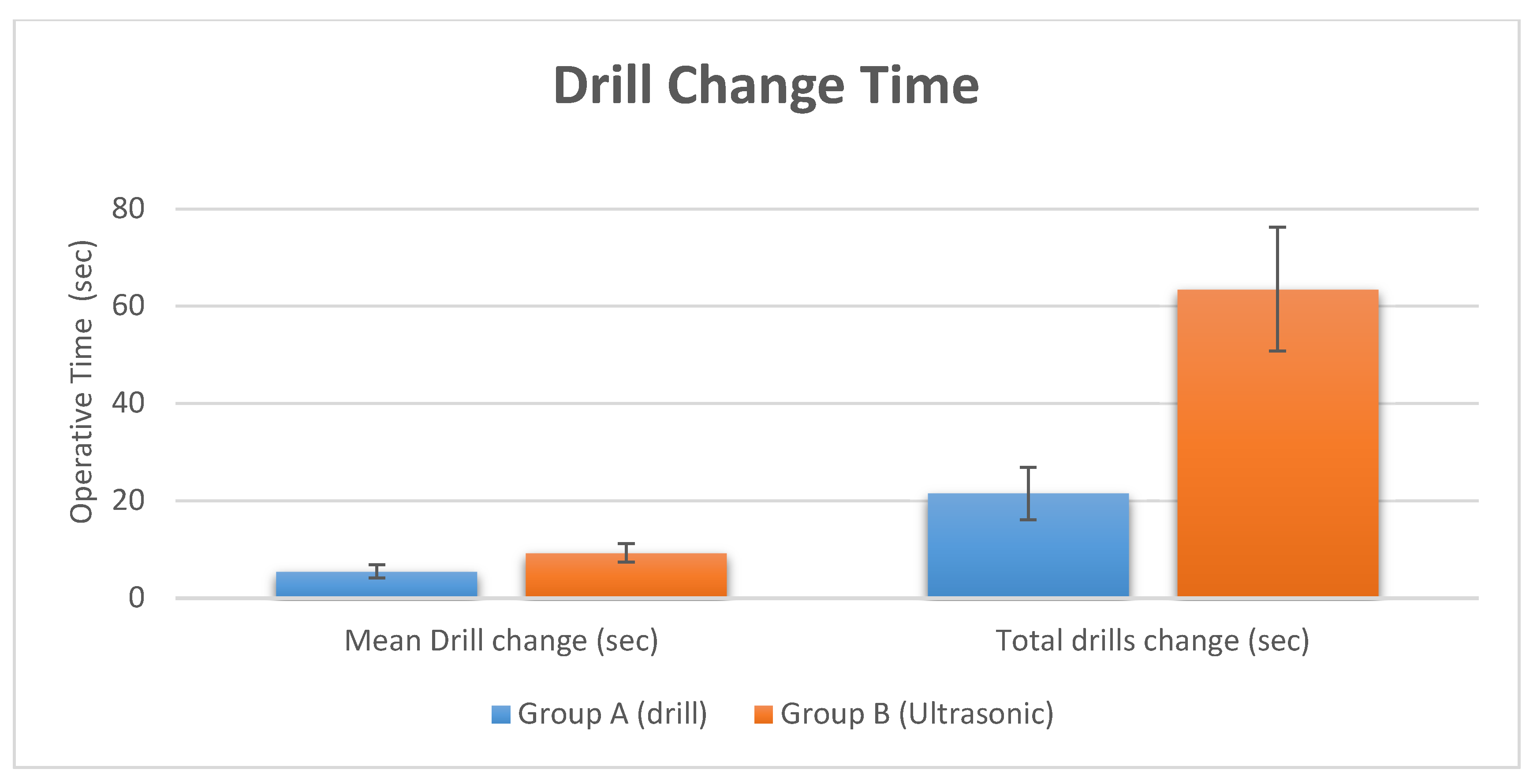
2.1.3. Operative Duration and Crestal Bone Level Measurement
2.2. Group B (Ultrasonic Instruments)
2.2.1. Clinical Observations
2.2.2. Pain and Swelling Intensity Evaluation.
2.2.3. Operative Duration and Crestal Bone Level Measurement
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Randomization and Study Design
4.3. Surgical Procedures
4.4. Pain and Swelling Intensity Evaluation
4.5. Crestal Bone Level Measurement
4.6. Statistical Evaluation
Author Contributions
Funding
Acknowledgments
Conflict of Interest
References
- Albrektsson, T.; Lekholm, U. Osseointegration: Current state of the art. Dent. Clin. North Am. 1989, 33, 537–554. [Google Scholar] [PubMed]
- Isola, G.; Matarese, G.; Williams, R.C.; Siciliano, V.I.; Alibrandi, A.; Cordasco, G.; Ramaglia, L. The effects of a desiccant agent in the treatment of chronic periodontitis: A randomized, controlled clinical trial. Clin. Oral Investig. 2018, 22, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Ramaglia, L.; Cicciù, M.; Cordasco, G.; Isola, G. The Effects of diode laser therapy as an adjunct to scaling and root planing in the treatment of aggressive periodontitis: A 1-year randomized controlled clinical trial. Photomed. Laser Surg. 2017, 35, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.E.; Auschill, T.M.; Sculean, A.; Arweiler, N.B. Clinical evaluation of non-surgical cleaning modalities on titanium dental implants during maintenance care: A 1-year follow-up on prosthodontic superstructures. Clin. Oral Investig. 2018. [Google Scholar] [CrossRef] [PubMed]
- Burgos, P.M.; Meirelles, L.; Sennerby, L. Early bone formation in furrows at titanium implants. A study in the rabbit tibia. J. Osseointegration 2010, 2, 15–22. [Google Scholar]
- Scarano, A.; Crocetta, E.; Quaranta, A.; Lorusso, F. Influence of the thermal treatment to address a better osseointegration of Ti6Al4V dental implants: Histological and histomorphometrical study in a rabbit model. Biomed. Res. Int. 2018, 2018, 2349698. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Degidi, M.; Perrotti, V.; Degidi, D.; Piattelli, A.; Iezzi, G. Experimental evaluation in rabbits of the effects of thread concavities in bone formation with different titanium implant surfaces. Clin. Implant Dent. Relat. Res. 2014, 16, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Perrotti, V.; Artese, L.; Degidi, M.; Degidi, D.; Piattelli, A.; Iezzi, G. Blood vessels are concentrated within the implant surface concavities: A histologic study in rabbit tibia. Odontology 2014, 102, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Carinci, F.; Quaranta, A.; Iezzi, G.; Piattelli, M.; Piattelli, A. Correlation between implant stability quotient (ISQ) with clinical and histological aspects of dental implants removed for mobility. Int. J. Immunopathol. Pharmacol. 2007, 20, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Degidi, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Correlation between implant stability quotient and bone-implant contact: A retrospective histological and histomorphometrical study of seven titanium implants retrieved from humans. Clin. Implant Dent. Relat. Res. 2006, 8, 218–222. [Google Scholar] [CrossRef]
- Salami, A.; Mora, R.; Dellepiane, M. Piezosurgery in the exeresis of glomus tympanicum tumours. Eur Arch Otorhinolaryngol. 2008, 265, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Salami, A.; Dellepiane, M.; Proto, E.; Mora, R. Piezosurgery in otologic surgery: Four years of experience. Otolaryngol. Head Neck Surg. 2009, 140, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, R.A.; Albrektsson, T.; Magnusson, B. Assessment of bone viability after heat trauma: A histological, histochemical and vital microscopic study in the rabbit. Scand. J. Plast. Reconstruct. Surg. 1984, 18, 261–268. [Google Scholar] [CrossRef]
- Sharawy, M.; Misch, C.E.; Weller, N.; Tehemar, S. Heat generation during implant drilling: The significance of motor speed. J. Oral Maxillofac. Surg. 2002, 60, 1160–1169. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Assenza, B.; Carinci, F.; Di Donato, L.; Romani, G.L.; Merla, A. Infrared thermographic evaluation of temperature modifications induced during implant site preparation with cylindrical versus conical drills. Clin. Implant Dent. Relat. Res. 2011, 13, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Vercellotti, T. Piezoelectric surgery in implantology: A case report--a new piezoelectric ridge expansion technique. Int. J. Periodontics Restorative Dent. 2000, 20, 358–365. [Google Scholar]
- De Campos, J.R.M.; Wolosker, N.; Yazbek, G.; Munia, M.A.; Kauffman, P.; Puech-Leao, P.; Jatene, F.B. Comparison of pain severity following video-assisted thoracoscopic sympathectomy: Electric versus harmonic scalpels. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Preti, G.; Martinasso, G.; Peirone, B.; Navone, R.; Manzella, C.; Muzio, G.; Russo, C.; Canuto, R.A.; Schierano, G. Cytokines and growth factors involved in the osseointegration of oral titanium implants positioned using piezoelectric bone surgery versus a drill technique: A pilot study in minipigs. J. Periodontol. 2007, 78, 716–722. [Google Scholar] [CrossRef]
- Schwarz, F.; Olivier, W.; Herten, M.; Sager, M.; Chaker, A.; Becker, J. Influence of implant bed preparation using an Er: YAG laser on the osseointegration of titanium implants: A histomorphometrical study in dogs. J. Oral Rehabil. 2007, 34, 273–281. [Google Scholar] [CrossRef]
- Horton, J.E.; Tarpley, T.M.; Wood, L.D. The healing of surgical defects in alveolar bone produced with ultrasonic instrumentation, chisel, and rotary bur. Oral Surg. Oral Med. Oral Pathol. 1975, 39, 536–546. [Google Scholar] [CrossRef]
- Vercellotti, T.; Nevins, M.L.; Kim, D.M.; Nevins, M.; Wada, K.; Schenk, R.K.; Fiorellini, J.P. Osseous response following resective therapy with piezosurgery. Int. J. Periodontics Restorative Dent. 2005, 25, 543–549. [Google Scholar]
- Chiriac, G.; Herten, M.; Schwarz, F.; Rothamel, D.; Becker, J. Autogenous bone chips: Influence of a new piezoelectric device (Piezosurgery®) on chip morphology, cell viability and differentiation. J. Clin. Periodontal. 2005, 32, 994–999. [Google Scholar] [CrossRef]
- Ramli, R.; Reher, P.; Harris, M.; Meghji, S. The effect of ultrasound on angiogenesis: An in vivo study using the chick chorioallantoic membrane. Int. J. Oral Maxillofac. Implants 2009, 24, 591–596. [Google Scholar]
- Landes, C.A.; Stübinger, S.; Rieger, J.; Williger, B.; Ha, T.K.L.; Sader, R. Critical evaluation of piezoelectric osteotomy in orthognathic surgery: Operative technique, blood loss, time requirement, nerve and vessel integrity. J. Oral Maxillofac. Surg. 2008, 66, 657–674. [Google Scholar] [CrossRef]
- Scarano, A.; Iezzi, G.; Perrotti, V.; Tetè, S.; Staiti, G.; Mortellaro, C.; Cappucci, C. Ultrasonic versus drills implant site preparation: A histologic analysis in bovine ribs. J. Craniofac. Surg. 2014, 25, 814–817. [Google Scholar] [CrossRef]
- Scarano, A.; Sinjari, B.; Murmura, G.; Lorusso, F. Neurosensory disturbance of the inferior alveolar nerve after 3025 implant placements. Implant Den. 2017, 26, 735–743. [Google Scholar] [CrossRef]
- Eltayeb, A.S.; Ahmad, A.G. Piezosurgery: A safe technique for inferior alveolar nerve mobilization in surgical correction of hemimandibular hyperplasia—Review of the literature and case report. Int. J. Surg. Case Rep. 2017, 31, 51–53. [Google Scholar] [CrossRef]
- Rude, K.; Svensson, P.; Starch-Jensen, T. Neurosensory Disturbances after Bilateral Sagittal Split Osteotomy using Piezoelectric Surgery: A Systematic Review. J. Oral Maxillofac. Surg. 2018. [Google Scholar] [CrossRef]
- Sirolli, M.; Mafra, C.E.S.; Santos, R.A.B.D.; Holzhausen, L.S.; Neto, C.; Batista, J. Influence of piezosurgery on bone healing around titanium implants: A histological study in rats. Braz. Dent. J. 2016, 27, 278–283. [Google Scholar] [CrossRef]
- Di Alberti, L.; Donnini, F.; Di Alberti, C.; Camerino, M. A comparative study of bone densitometry during osseointegration: Piezoelectric surgery versus rotary protocols. Quintessence Int. 2010, 41. [Google Scholar]
- Büchter, A.; Kleinheinz, J.; Wiesmann, H.P.; Kersken, J.; Nienkemper, M.; Weyhrother, H.V.; Meyer, U. Biological and biomechanical evaluation of bone remodelling and implant stability after using an osteotome technique. Clin. Oral Implants Res. 2005, 16, 1–8. [Google Scholar] [CrossRef]
- Shalabi, M.M.; Wolke, J.G.; De Ruijter, A.J.; Jansen, J.A. Histological evaluation of oral implants inserted with different surgical techniques into the trabecular bone of goats. Clin. Oral Implants Res. 2007, 18, 489–495. [Google Scholar] [CrossRef]
- Iyer, S.; Weiss, C.; Mehta, A. Effects of drill speed on heat production and the rate and quality of bone formation in dental implant osteotomies. Part I: Relationship between drill speed and heat production. Int. J. Prosthodont. 1997, 10, 411–414. [Google Scholar]
- Schlegel, K.A.; Kloss, F.R.; Kessler, P.; Schultze-Mosgau, S.; Nkenke, E.; Wiltfang, J. Bone conditioning to enhance implant osseointegration: An experimental study in pigs. Int. J. Oral Maxillofac. Implants 2003, 18, 505–511. [Google Scholar]
- Salami, A.; Dellepiane, M.; Salzano, F.A.; Mora, R. Piezosurgery in the excision of middle-ear tumors: Effects on mineralized and non-mineralized tissues. Med. Sci. Monit. 2007, 13, 25–29. [Google Scholar]
- Frost, H.M. Bone microdamage: Factors that impair its repair. In Current Concepts of Bone Fragility; Springer: Berlin/Heidelberg, Germany, 1986; pp. 123–146. [Google Scholar]
- Parfitt, A.M. Targeted and nontargeted bone remodeling: Relationship to basic multicellular unit origination and progression. Bone 2002, 30, 5–7. [Google Scholar] [CrossRef]
- Noble, B.S.; Peet, N.; Stevens, H.Y.; Brabbs, A.; Mosley, J.R.; Reilly, G.C.; Reeve, J.; Skerry, T.M.; Lanyon, L.E. Mechanical loading: Biphasic osteocyte survival and targeting of osteoclasts for bone destruction in rat cortical bone. Am. J. Physiol. Cell Physiol. 2003, 284, 934–943. [Google Scholar] [CrossRef]
- García-Moreno, S.; González-Serrano, J.; López-Pintor, R.M.; Pardal-Peláez, B.; Hernández, G.; Martínez-González, J.M. Implant stability using piezoelectric bone surgery compared with conventional drilling: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 1453–1464. [Google Scholar] [CrossRef]
- Sendyk, D.I.; Oliveira, N.K.; Pannuti, C.M.; Naclério-Homem, M. da G.; Wennerberg, A.; Zindel Deboni, M.C. Conventional drilling versus piezosurgery for implant site preparation: A meta-analysis. J. Oral Implantol. 2018, 44, 400–405. [Google Scholar] [CrossRef]
- Salami, A.; Mora, R.; Dellepiane, M.; Crippa, B.; Santomauro, V.; Guastini, L. Piezosurgery versus microdrill in intact canal wall mastoidectomy. Eur. Arch. Otorhinolaryngol. 2010, 267, 1705–1711. [Google Scholar] [CrossRef]
- Salami, A.; Vercellotti, T.; Mora, R.; Dellepiane, M. Piezoelectric bone surgery in otologic surgery. Otolaryngol. Head Neck Surg. 2007, 136, 484–485. [Google Scholar] [CrossRef]
- Scarano, A. Traditional Postextractive implant site preparation compared with pre-extractive interradicular implant bed preparation in the mandibular molar region, using an ultrasonic device: A randomized pilot study. Int. J. Oral Maxillofac. Implants 2017, 32, 655–660. [Google Scholar] [CrossRef]
- Carini, F.; Saggese, V.; Porcaro, G.; Baldoni, M. Piezolelectric surgery in dentistry: A review. Minerva Stomatol. 2014, 63, 7–34. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Groups | Pain (VAS Score) | Swelling (VRS Score) | ||||||
|---|---|---|---|---|---|---|---|---|
| Group A (Drill) | Day 1 | Day 2 | Day 4 | Day 6 | Day 1 | Day 2 | Day 4 | Day 6 |
| Mean Rate (SD) | 16.33 ± 4.12 | 19.22 ± 2.22 | 0.92 ± 0.3 | 0.11 ± 0.02 | 1.9 ± 0.8 | 1.2 ± 0.4 | 0.36 ± 0.31 | - |
| Group B (Ultrasonic) | Day 1 | Day 2 | Day 4 | Day 6 | Day 1 | Day 2 | Day 4 | Day 6 |
| Mean Rate (SD) | 12.33 ± 2.32 | 15.32 ± 3.34 | 0.82 ± 0.01 | 0.1 ± 0.01 | 1.27 ± 0.6 | 0.9 ± 0.58 | 0.27 ± 0.14 | - |
| p value | p = 0.003 (**) | p = 0.04 (*) | p = 0.66 | p = 0.57 | p = 0.046 (*) | p = 0.28 | p = 0.8 | |
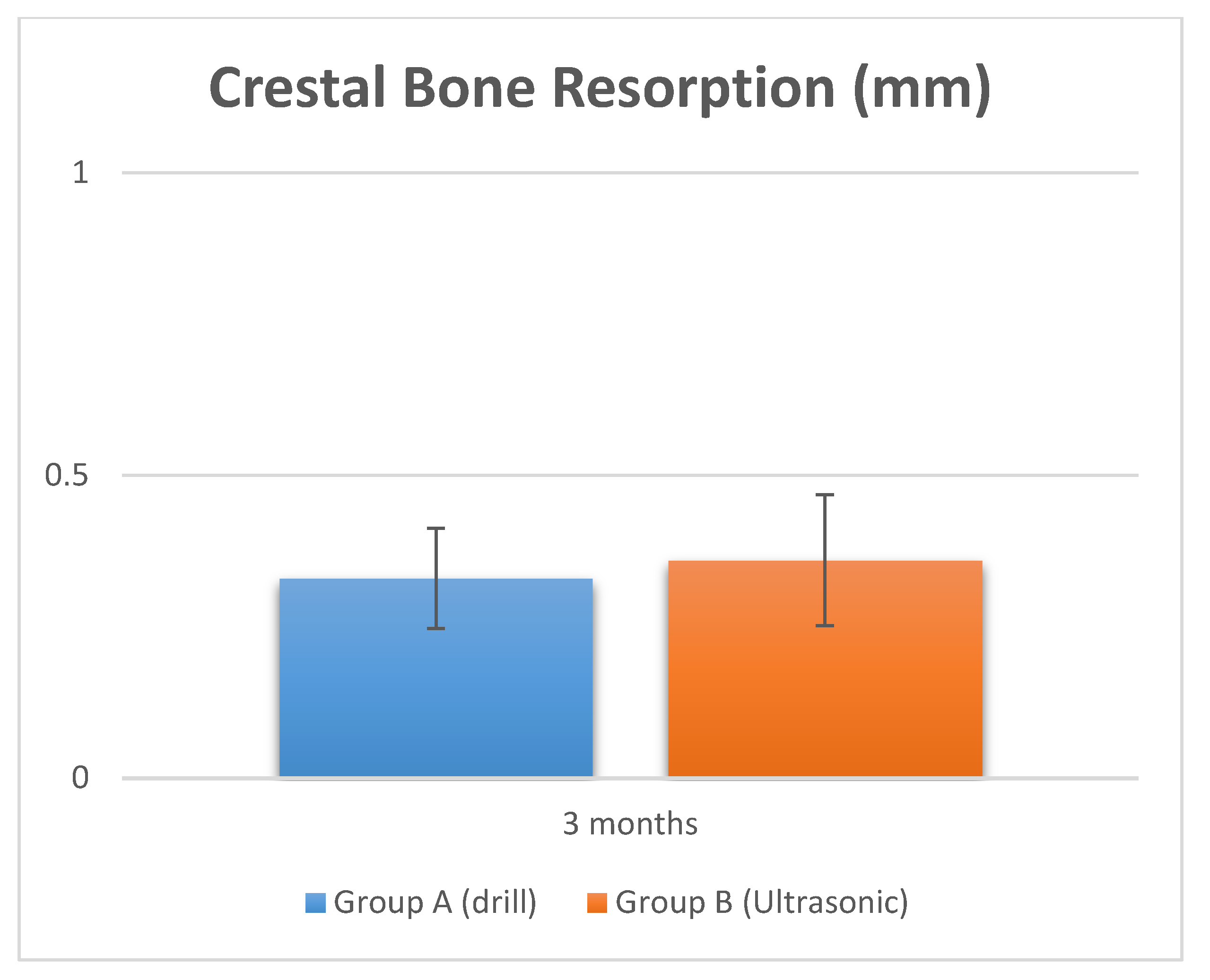
| Study Groups | Surgical Time | Crestal Bone Resorption | ||
|---|---|---|---|---|
| Group A (Drill) | Operative Duration | Drill Change | Total time drill change | At 3 months |
| Mean (SD) | 2.5 ± 0.34 min | 5.5 ± 2.1 s | 21.5 ± 2.1 s | 0.03 ± 0.001 mm |
| Group B (Ultrasonic) | Operative Duration | Drill Change | Total time drill change | At 3 months |
| Mean (SD) | 10.5 ± 3.1 min | 9.3 ± 3.2 s | 63.5 ± 2.1 s | 0.036 ± 0.001 mm |
| p value | p = 0.00002 (**) | p = 0.00023 (**) | p = 0.00006 (**) | p = 0.8 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Carinci, F.; Lorusso, F.; Festa, F.; Bevilacqua, L.; Santos de Oliveira, P.; Maglione, M. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Materials 2018, 11, 2516. https://doi.org/10.3390/ma11122516
Scarano A, Carinci F, Lorusso F, Festa F, Bevilacqua L, Santos de Oliveira P, Maglione M. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Materials. 2018; 11(12):2516. https://doi.org/10.3390/ma11122516
Chicago/Turabian StyleScarano, Antonio, Francesco Carinci, Felice Lorusso, Felice Festa, Lorenzo Bevilacqua, Pablo Santos de Oliveira, and Michele Maglione. 2018. "Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study" Materials 11, no. 12: 2516. https://doi.org/10.3390/ma11122516