A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
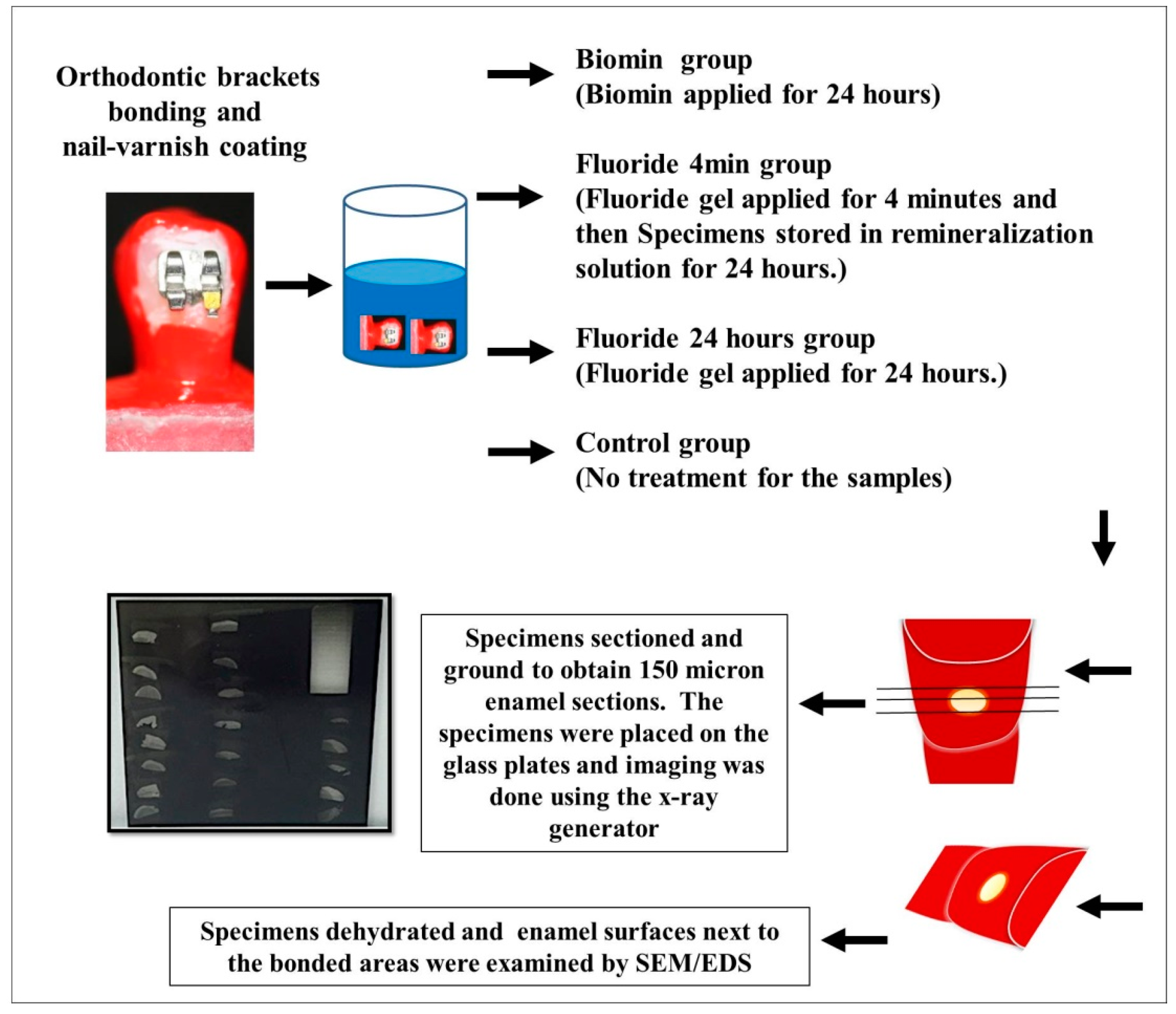
2. Materials and Methods
2.1. Specimens’ Preparation
2.2. Biomin Application
2.3. Application of Bonding Agent
2.4. TMR Analysis
2.5. SEM/EDS Top Surface Examination
2.6. SEM/EDS Interface Preparation
2.7. Statistical Analysis
3. Results
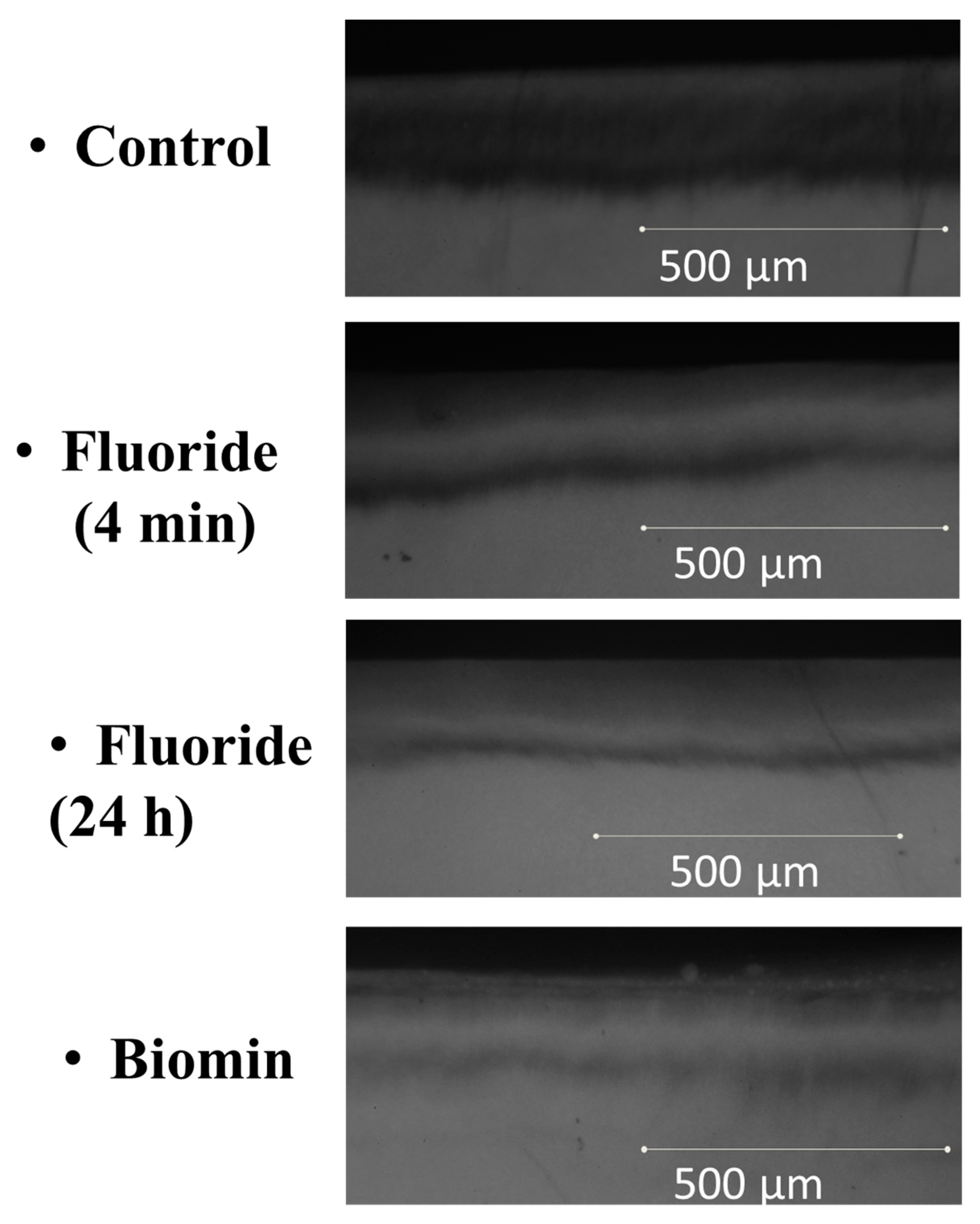
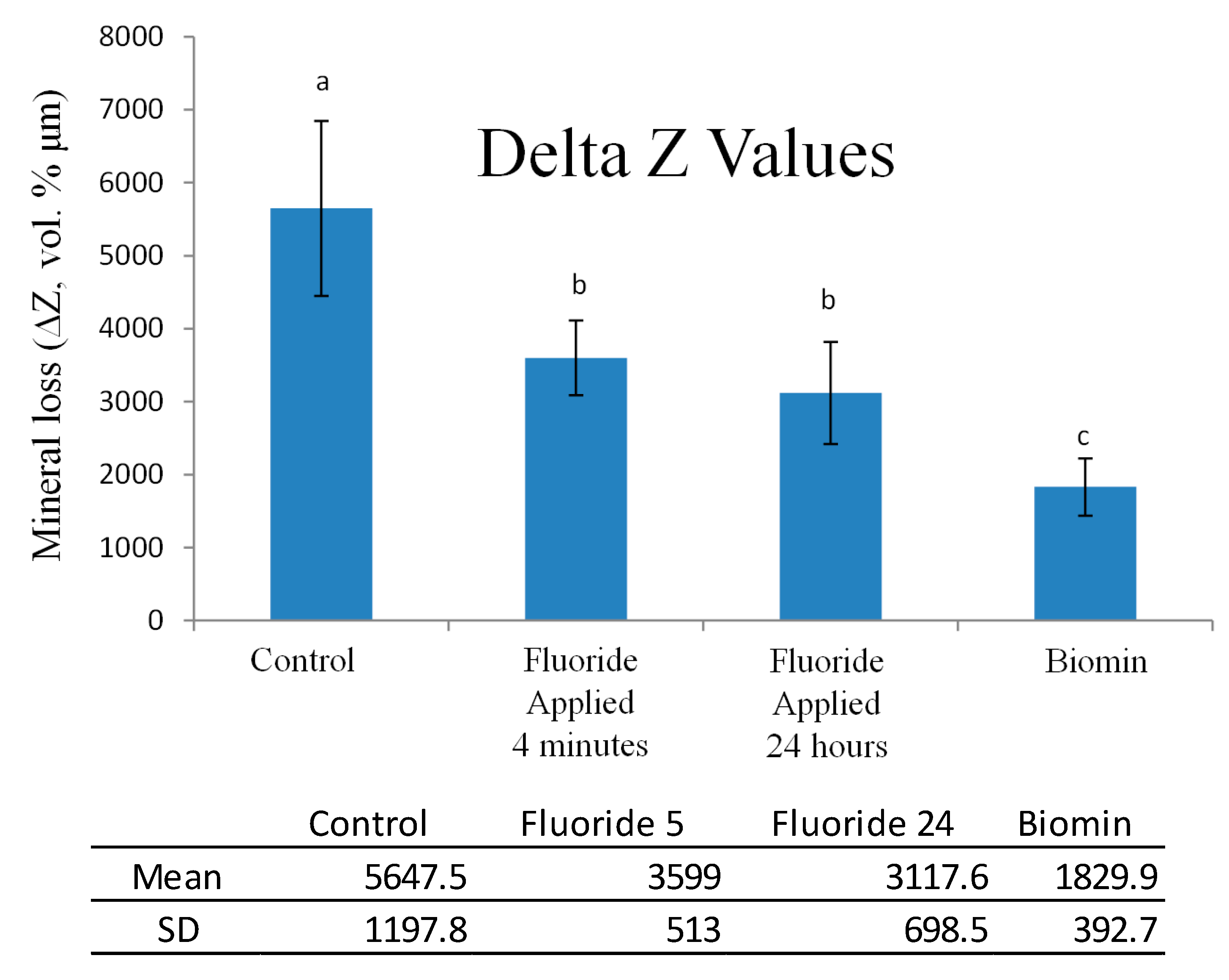
3.1. Transverse Microradiography
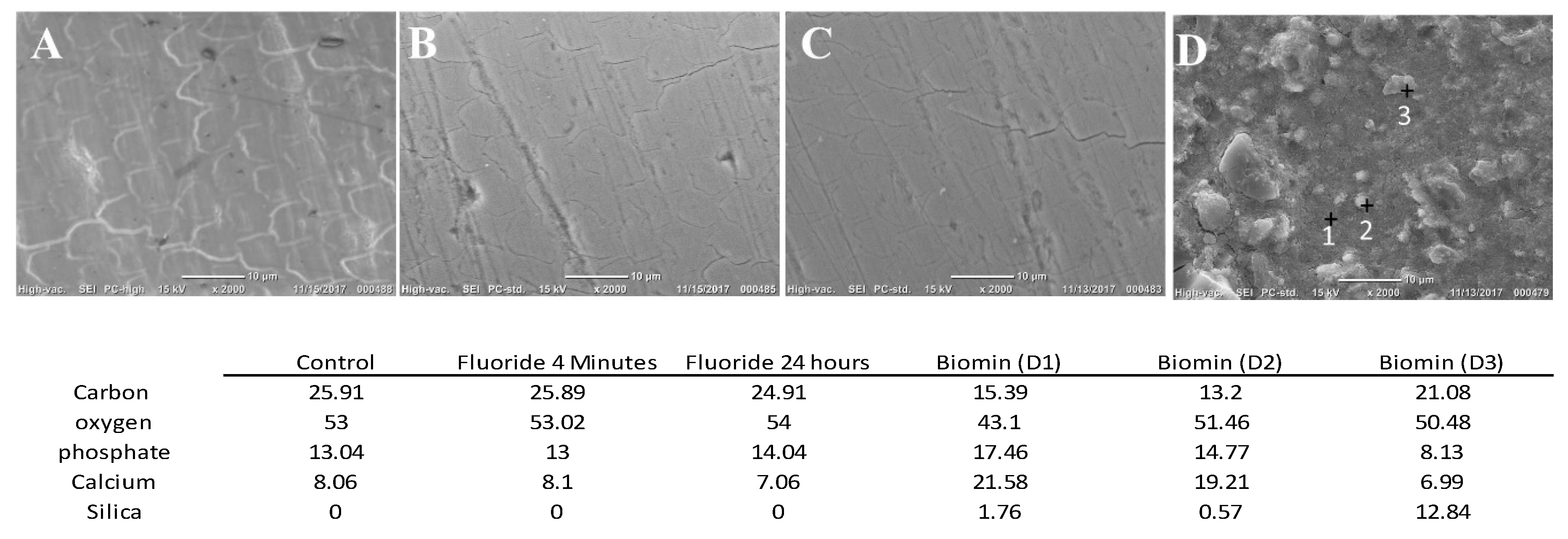
3.2. SEM/EDS Top Surface Examination
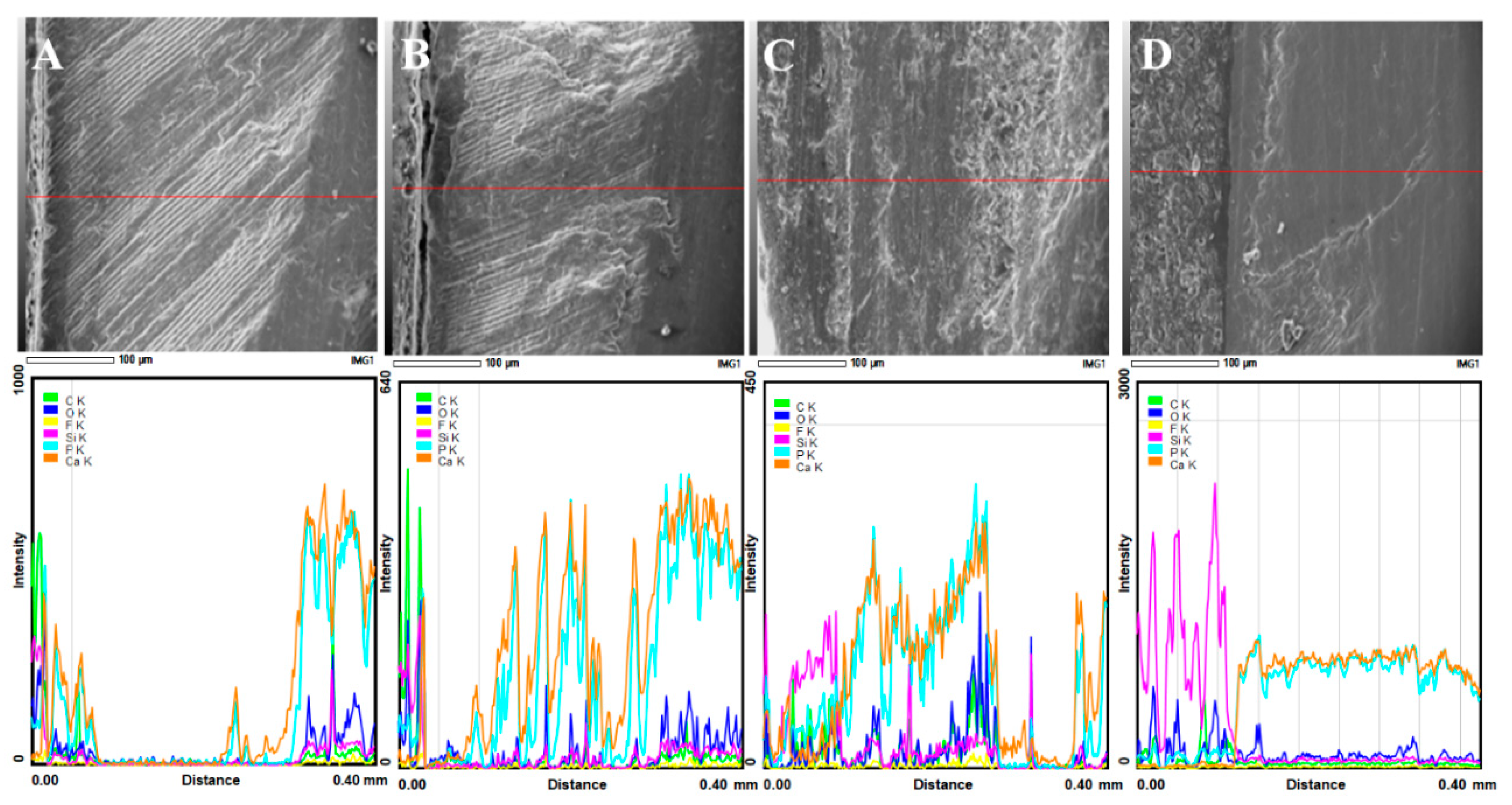
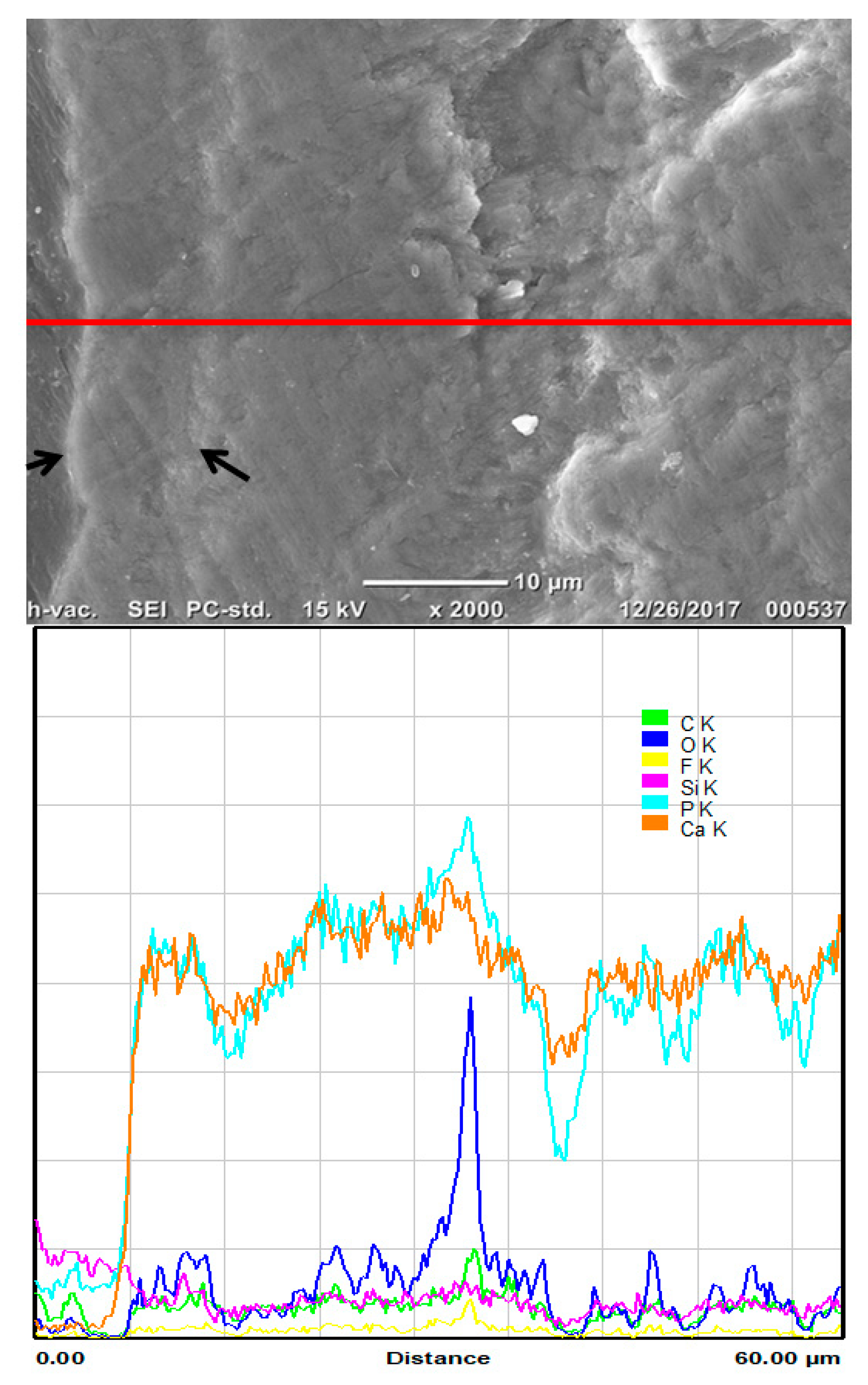
3.3. SEM/EDS Interface Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bakhsh, T.A.; Bakry, A.S.; Mandurah, M.M.; Abbassy, M.A. Novel evaluation and treatment techniques for white spot lesions. An in vitro study. Orthod. Craniofac. Res. 2017, 20, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Al-Bazi, S.M.; Abbassy, M.A.; Bakry, A.S.; Merdad, L.A.; Hassan, A.H. Effects of chlorhexidine (gel) application on bacterial levels and orthodontic brackets during orthodontic treatment. J. Oral Sci. 2016, 58, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klukowska, M.; Bader, A.; Erbe, C.; Bellamy, P.; White, D.J.; Anastasia, M.K.; Wehrbein, H. Plaque levels of patients with fixed orthodontic appliances measured by digital plaque image analysis. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e463–e470. [Google Scholar] [CrossRef] [PubMed]
- Crombie, F.A.; Manton, D.J.; Palamara, J.E.; Zalizniak, I.; Cochrane, N.J.; Reynolds, E.C. Characterisation of developmentally hypomineralised human enamel. J. Dent. 2013, 41, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Bernardi, S.; Pasini, M.; Giuca, M.R.; Docimo, R.; Continenza, M.A.; Gatto, R. The process of mineralisation in the development of human tooth. Eur. J. Paediatr. Dent. 2016, 17, 322–326. [Google Scholar] [PubMed]
- Pasini, M.; Giuca, M.R.; Scatena, M.; Gatto, R.; Caruso, S. Molar incisor hypomineralization treatment with casein phosphopeptide and amorphous calcium phosphate in children. Minerva Stomatol. 2018, 67, 20–25. [Google Scholar]
- Atar, M.; Korperich, E.J. Systemic disorders and their influence on the development of dental hard tissues: A literature review. J. Dent. 2010, 38, 296–306. [Google Scholar] [CrossRef]
- Walsh, L.J.; Brostek, A.M. Minimum intervention dentistry principles and objectives. Aust. Dent. J. 2013, 58 (Suppl. 1), 3–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakry, A.S.; Marghalani, H.Y.; Amin, O.A.; Tagami, J. The effect of a bioglass paste on enamel exposed to erosive challenge. J. Dent. 2014, 42, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Takahashi, H.; Otsuki, M.; Tagami, J. Evaluation of new treatment for incipient enamel demineralization using 45S5 bioglass. Dent. Mater. 2014, 30, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Takahashi, H.; Otsuki, M.; Sadr, A.; Yamashita, K.; Tagami, J. CO2 laser improves 45S5 bioglass interaction with dentin. J. Dent. Res. 2011, 90, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Takahashi, H.; Otsuki, M.; Tagami, J. The durability of phosphoric acid promoted bioglass-dentin interaction layer. Dent. Mater. 2013, 29, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Brauer, D.S.; Karpukhina, N.; O’Donnell, M.D.; Law, R.V.; Hill, R.G. Fluoride-containing bioactive glasses: Effect of glass design and structure on degradation, pH and apatite formation in simulated body fluid. Acta Biomater. 2010, 6, 3275–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakry, A.S.; Al-Hadeethi, Y.; Razvi, M.A. The durability of a hydroxyapatite paste used in decreasing the permeability of hypersensitive dentin. J. Dent. 2016, 51, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Tamura, Y.; Otsuki, M.; Kasugai, S.; Ohya, K.; Tagami, J. Cytotoxicity of 45S5 bioglass paste used for dentine hypersensitivity treatment. J. Dent. 2011, 39, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Nakajima, M.; Otsuki, M.; Tagami, J. Effect of Er:YAG laser on dentin bonding durability under simulated pulpal pressure. J. Adhes. Dent. 2009, 11, 361–368. [Google Scholar] [PubMed]
- Bakry, A.S.; Sadr, A.; Inoue, G.; Otsuki, M.; Tagami, J. Effect of Er:YAG laser treatment on the microstructure of the dentin/adhesive interface after acid-base challenge. J. Adhes. Dent. 2007, 9, 513–520. [Google Scholar] [PubMed]
- Bakry, A.S.; Sadr, A.; Takahashi, H.; Otsuki, M.; Tagami, J. Analysis of Er:YAG lased dentin using attenuated total reflectance Fourier transform infrared and X-ray diffraction techniques. Dent. Mater. J. 2007, 26, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Hamba, H.; Nikaido, T.; Sadr, A.; Nakashima, S.; Tagami, J. Enamel lesion parameter correlations between polychromatic micro-CT and TMR. J. Dent. Res. 2012, 91, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Kitasako, Y.; Sadr, A.; Hamba, H.; Ikeda, M.; Tagami, J. Gum containing calcium fluoride reinforces enamel subsurface lesions in situ. J. Dent. Res. 2012, 91, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Bakry, A.S.; Abbassy, M.A. Increasing the efficiency of CPP-ACP to remineralize enamel white spot lesions. J. Dent. 2018, 76, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.C.; Cai, F.; Cochrane, N.J.; Shen, P.; Walker, G.D.; Morgan, M.V.; Reynolds, C. Fluoride and casein phosphopeptide-amorphous calcium phosphate. J. Dent. Res. 2008, 87, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Tschoppe, P.; Meyer-Lueckel, H. Effects of regular and highly fluoridated toothpastes in combination with saliva substitutes on artificial enamel caries lesions differing in mineral content. Arch. Oral Biol. 2012, 57, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Baysan, A.; Lynch, E.; Ellwood, R.; Davies, R.; Petersson, L.; Borsboom, P. Reversal of primary root caries using dentifrices containing 5000 and 1100 ppm fluoride. Caries Res. 2001, 35, 41–46. [Google Scholar] [PubMed]
- Amaechi, B.T.; Higham, S.M. In vitro remineralisation of eroded enamel lesions by saliva. J. Dent. 2001, 29, 371–376. [Google Scholar] [CrossRef]
- Liu, J.; Rawlinson, S.C.; Hill, R.G.; Fortune, F. Fluoride incorporation in high phosphate containing bioactive glasses and in vitro osteogenic, angiogenic and antibacterial effects. Dent. Mater. 2016, 32, e221–e237. [Google Scholar] [CrossRef] [PubMed]
- Iijima, M.; Onuma, K. Roles of Fluoride on Octacalcium Phosphate and Apatite Formation on Amorphous Calcium Phosphate Substrate. Cryst. Growth Des. 2018, 18, 2279–2288. [Google Scholar] [CrossRef]
- Mneimne, M.; Hill, R.G.; Bushby, A.J.; Brauer, D.S. High phosphate content significantly increases apatite formation of fluoride-containing bioactive glasses. Acta Biomater. 2011, 7, 1827–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiura, M.; Kitasako, Y.; Sadr, A.; Shimada, Y.; Sumi, Y.; Tagami, J. White spot lesion remineralization by sugar-free chewing gum containing bio-available calcium and fluoride: A double-blind randomized controlled trial. J. Dent. 2016, 54, 86–91. [Google Scholar] [CrossRef] [PubMed]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakry, A.S.; Abbassy, M.A.; Alharkan, H.F.; Basuhail, S.; Al-Ghamdi, K.; Hill, R. A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions. Materials 2018, 11, 1636. https://doi.org/10.3390/ma11091636
Bakry AS, Abbassy MA, Alharkan HF, Basuhail S, Al-Ghamdi K, Hill R. A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions. Materials. 2018; 11(9):1636. https://doi.org/10.3390/ma11091636
Chicago/Turabian StyleBakry, Ahmed Samir, Mona Aly Abbassy, Hanin Fahad Alharkan, Sara Basuhail, Khalil Al-Ghamdi, and Robert Hill. 2018. "A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions" Materials 11, no. 9: 1636. https://doi.org/10.3390/ma11091636
APA StyleBakry, A. S., Abbassy, M. A., Alharkan, H. F., Basuhail, S., Al-Ghamdi, K., & Hill, R. (2018). A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions. Materials, 11(9), 1636. https://doi.org/10.3390/ma11091636