Bone-Healing Pattern on the Surface of Titanium Implants at Cortical and Marrow Compartments in Two Topographic Sites: an Experimental Study in Rabbits

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Design and Experimental Animals
2.3. Randomization and Allocation Concealment
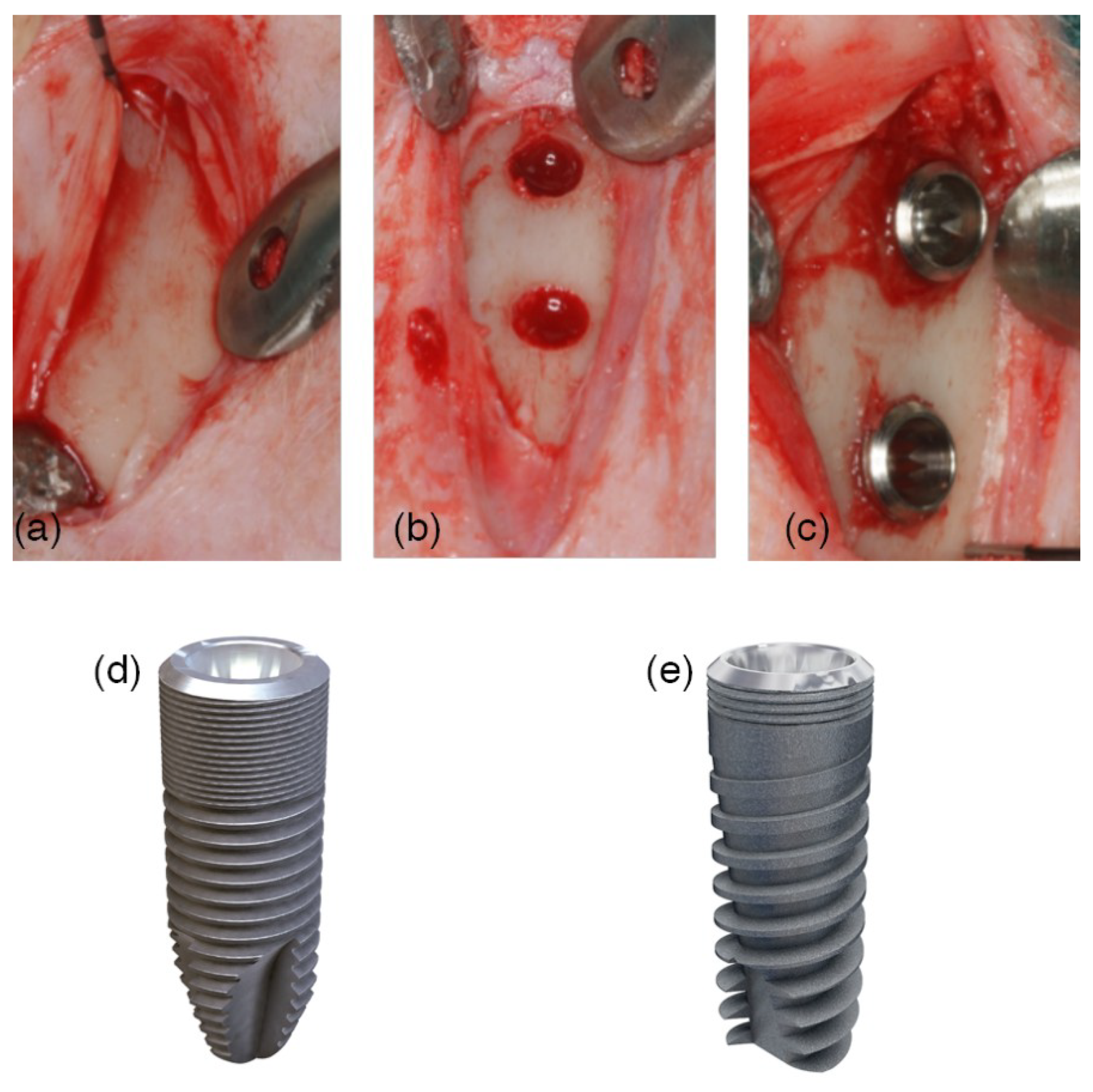
2.4. Implant Features
2.5. Surgical Procedures
2.6. Post-Operative Care, Housing and Husbandry
2.7. Euthanasia
2.8. Histological Preparation
2.9. Histological Examination
2.10. Data Analysis
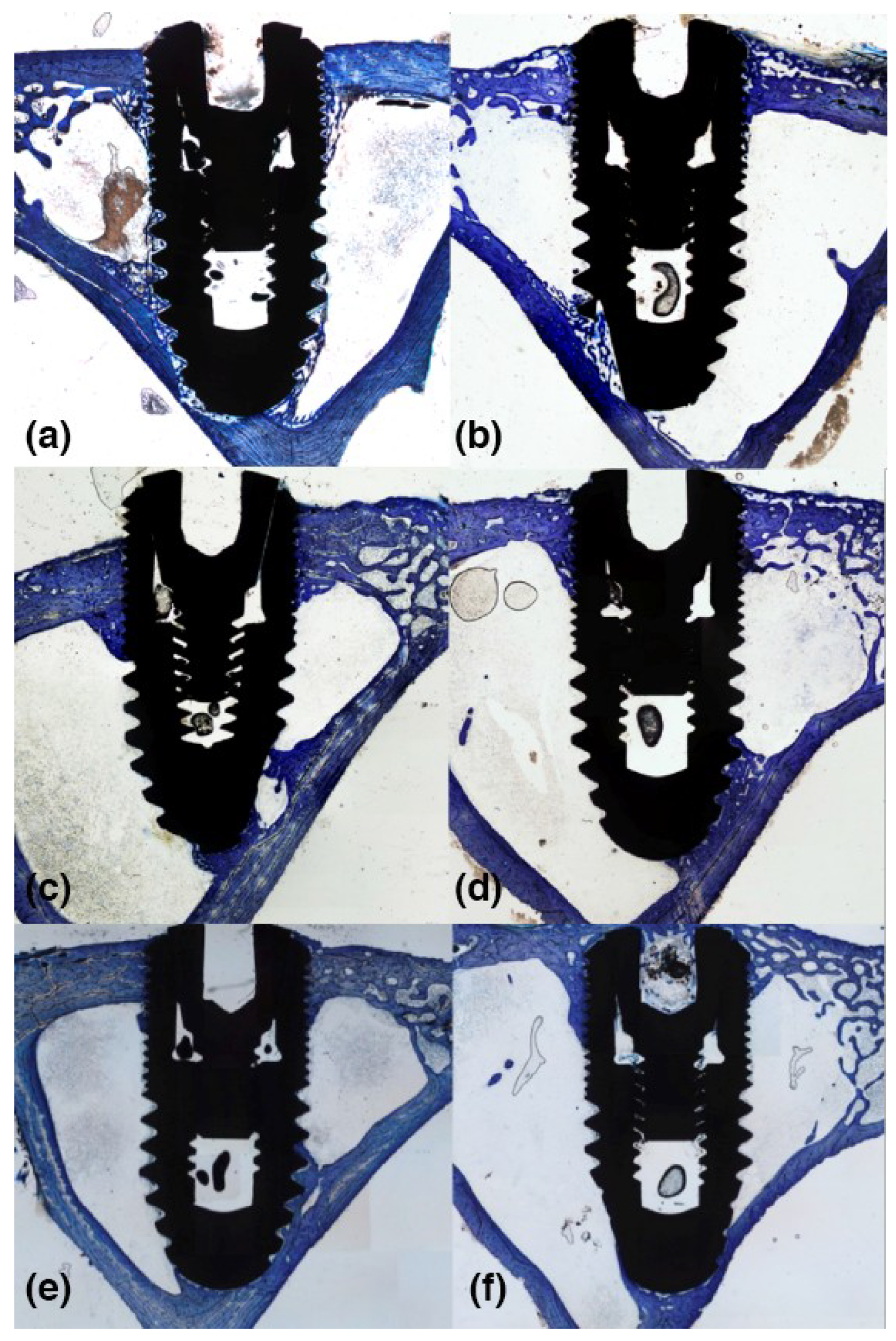
3. Results
3.1. Clinical and Histological Outcomes
3.2. 2-Weeks of Healing
3.3. 4-Weeks of Healing
3.4. 8-Weeks of Healing
4. Discussion
5. Conclusions
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BIC | bone to implant contact |
| RBM | resorbable blasted media |
| CaP | calcium phosphate bioceramic |
| NB | new bone |
| ST | soft tissue |
| OB | old bone |
References
- Abrahamsson, I.; Linder, E.; Lang, N.P.; Berglundh, T.; Linder, E.; Lang, N.P.; Lindhe, J. Early bone formation adjacent to rough and tumed endosseous implant surfaces An experimental study in the dog. Clin. Oral Implants Res. 2003, 15, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Persson, L.G.; Lindhe, J. Bone regeneration at implants with turned or rough surfaces in self-contained defects. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Lang, N.P. Dynamics of osseointegration in various human and animal models—A comparative analysis. Clin. Oral Implants Res. 2017, 28, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.B.; Campos, F.E.; Marin, C.; Teixeira, H.S.; Bonfante, E.A.; Suzuki, M.; Witek, L.; Zanetta-Barbosa, D.; Coelho, P.G. Implant Biomechanical Stability Variation at Early Implantation Times in Vivo: An Experimental Study in Dogs. Int. J. Oral Maxillofac. Implants 2013, 28, e128–e134. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Eriksson, A.R.; Friberg, B.; Lekholm, U.; Lindahl, L.; Nevins, M.; Oikarinen, V.; Roos, J.; Sennerby, L.; Astrand, P. Histologic investigations on 33 retrieved Nobelpharma implants. Clin. Mater. 1993, 12, 1–9. [Google Scholar] [CrossRef]
- Kumar, G.; Narayan, B. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Class Pap. Orthop. 2014, 52, 507–509. [Google Scholar]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implants Res. 2006, 17, 244–250. [Google Scholar] [CrossRef]
- Marco, F.; Milena, F.; Gianluca, G.; Vittoria, O. Peri-implant osteogenesis in health and osteoporosis. Micron 2005, 36, 630–644. [Google Scholar] [CrossRef]
- Falco, A.; Berardini, M.; Trisi, P. Correlation Between Implant Geometry, Implant Surface, Insertion Torque, and Primary Stability: In Vitro Biomechanical Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, 824–830. [Google Scholar] [CrossRef]
- Sela, M.N.; Badihi, L.; Rosen, G.; Steinberg, D.; Kohavi, D. Adsorption of human plasma proteins to modified titanium surfaces. Clin. Oral Implants Res. 2007, 18, 630–638. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implants Res. 2009, 20, 172–184. [Google Scholar] [CrossRef]
- Park, J.Y.; Gemmell, C.H.; Davies, J.E. Platelet interactions with titanium: Modulation of platelet activity by surface topography. Biomaterials 2001, 22, 2671–2682. [Google Scholar] [CrossRef]
- Koh, J.-W.; Yang, J.-H.; Han, J.-S.; Lee, J.-B.; Kim, S.-H. Biomechanical evaluation of dental implants with different surfaces: Removal torque and resonance frequency analysis in rabbits. J. Adv. Prosthodont. 2009, 1, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Davies, J. Understanding peri-implant endosseous healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [PubMed]
- Spriano, S.; Yamaguchi, S.; Baino, F.; Ferraris, S. A critical review of multifunctional titanium surfaces: New frontiers for improving osseointegration and host response, avoiding bacteria contamination. Acta Biomater. 2018, 79, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Barfeie, A.; Wilson, J.; Rees, J. Implant surface characteristics and their effect on osseointegration. Br. Dent. J. 2015, 218, E9. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.-S. Reality of dental implant surface modification: A short literature review. Open Biomed. Eng. J. 2014, 8, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, M.; Scarano, A.; Paolantonio, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Bone response to machined and resorbable blast material titanium implants: An experimental study in rabbits. J. Oral Implantol. 2002, 28, 2–8. [Google Scholar] [CrossRef]
- Coelho, P.G.; Bonfante, E.A.; Pessoa, R.S.; Marin, C.; Granato, R.; Giro, G.; Witek, L.; Suzuki, M. Characterization of five different implant surfaces and their effect on osseointegration: A study in dogs. J. Periodontol. 2011, 82, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.-S.; Han, J.-S.; Yang, J.-H. Biomechanical and histomorphometric study of dental implants with different surface characteristics. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 87, 303–311. [Google Scholar] [CrossRef]
- Müeller, W.-D.; Gross, U.; Fritz, T.; Voigt, C.; Fischer, P.; Berger, G.; Rogaschewski, S.; Lange, K.P. Evaluation of the interface between bone and titanium surfaces being blasted by aluminium oxide or bioceramic particles. Clin. Oral Implants Res. 2003, 14, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-G.; Jeong, Y.-S.; Huh, Y.-H.; Park, C.-J.; Cho, L.-R. Impact of Surface Chemistry Modifications on Speed and Strength of Osseointegration. Int. J. Oral Maxillofac. Implants 2018, 33, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Lang, N.P.; De Santis, E.; Morelli, F.; Favero, G.; Botticelli, D. Bone-healing pattern at the surface of titanium implants: An experimental study in the dog. Clin. Oral Implants Res. 2014, 25, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Morelli, F.; Lang, N.P.; Bengazi, F.; Baffone, D.; Dadonim Vila Morales, C.; Botticelli, D. Influence of bone marrow on osseointegration in long bones: An experimental study in sheep. Clin. Oral Implants Res. 2015, 26, 300–306. [Google Scholar] [CrossRef]
- Caneva, M.; Lang, N.P.; Calvo Guirado, J.L.; Spriano, S.; Iezzi, G.; Botticelli, D. Bone healing at bicortically installed implants with different surface configurations. An experimental study in rabbits. Clin. Oral Implants Res. 2015, 26, 293–299. [Google Scholar] [CrossRef]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implants 2005, 20, 425–431. [Google Scholar]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. The ARRIVE Guidelines Checklist Animal Research: Reporting In Vivo Experiments. Br. J. Pharmacol. 2010, 8, 8–9. [Google Scholar]
- Bosshardt, D.D.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Lang, N.P. The role of bone debris in early healing adjacent to hydrophilic and hydrophobic implant surfaces in man. Clin. Oral Implants Res. 2011, 22, 357–364. [Google Scholar] [CrossRef]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implants Res. 2011, 22, 349–356. [Google Scholar] [CrossRef]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants: A model study in the dog. Clin. Oral Implants Res. 2003, 14, 251–262. [Google Scholar] [CrossRef]
- Gottlow, J.; Barkamo, S.; Sennerby, L. An Experimental Comparison of Two Different Clinically Used Implant Designs and Surfaces. Clin. Implant Dent. Relat. Res. 2012, 14, e204-12. [Google Scholar] [CrossRef] [PubMed]
- Isidor, F. Influence of forces on peri-implant bone. Clin. Oral Implants Res. 2006, 17, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buser, D.; Broggini, N.; Wieland, M.; Schenk, R.K.; Denzer, A.J.; Cochran, D.L.; Hoffmann, B.; Lussi, A.; Steinemann, S.G. Enhanced bone apposition to a chemically modified SLA titanium surface. J. Dent. Res. 2004, 83, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Leonard, G.; Coelho, P.; Polyzois, I.; Stassen, L.; Claffey, N. A study of the bone healing kinetics of plateau versus screw root design titanium dental implants. Clin. Oral Implants Res. 2009, 20, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Suzuki, M.; Guimaraes, M.V.M.; Marin, C.; Granato, R.; Gil, J.N.; Miller, R.J. Early bone healing around different implant bulk designs and surgical techniques: A study in dogs. Clin. Implant Dent. Relat. Res. Can. 2010, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compartment | Follow-up | Topographic Site | Statistic | New Bone | Soft Tissue | Old Bone |
|---|---|---|---|---|---|---|
| Cortical compartment | 2 w | Cort-dia | Mean | 17.8 | 70.0 | 12.2 |
| SD | 10.6 | 8.9 | 6.6 | |||
| Median | 14.0 | 68.2 | 8.3 | |||
| Cort-meta | Mean | 15.1 | 76.3 | 8.5 | ||
| SD | 5.8 | 6.4 | 6.5 | |||
| Median | 14.8 | 78.9 | 6.2 | |||
| Differences | p | 0.39 | 0.09 | 0.11 | ||
| 4 w | Cort-dia | Mean | 21.4 | 74.6 | 4.0 *,# | |
| SD | 6.9 | 7.8 | 3.2 | |||
| Median | 21.6 | 74.6 | 3.0 | |||
| Cort-meta | Mean | 19.7 * | 78.6 * | 1.7 # | ||
| SD | 8.3 | 8.0 | 1.5 | |||
| Median | 17.3 | 79.3 | 1.5 | |||
| Differences | p | 0.57 | 0.26 | 0.04 | ||
| 8 w | Cort-dia | Mean | 37.0 * | 58.9 * | 4.1 | |
| SD | 5.7 | 6.8 | 2.6 | |||
| Median | 37.3 | 58.5 | 4.3 | |||
| Cort-meta | Mean | 35.5 * | 61.3 * | 3.2 * | ||
| SD | 8.7 | 9.8 | 3.4 | |||
| Median | 33.8 | 60.9 | 2.6 | |||
| Differences | p | 0.63 | 0.62 | 0.88 | ||
| Marrow compartment | 2 w | Marrow-dia | Mean | 13.8 | 78.9 | 7.3 |
| SD | 9.2 | 12.3 | 8.9 | |||
| Median | 13.2 | 82.8 | 2.9 | |||
| Marrow-meta | Mean | 10.3 | 86.1 | 3.6 | ||
| SD | 8.2 | 8.0 | 5.1 | |||
| Median | 9.3 | 89.5 | 0.5 | |||
| Differences | p | 0.18 | 0.07 | 0.23 | ||
| 4 w | Marrow-dia | Mean | 20.4 # | 77.9 # | 1.7 * | |
| SD | 6.8 | 6.9 | 2.3 | |||
| Median | 19.7 | 79.4 | 0.4 | |||
| Marrow-meta | Mean | 13.0 *,# | 86.4 *,# | 0.6 | ||
| SD | 8.2 | 8.5 | 0.8 | |||
| Median | 13.3 | 86.7 | 0.0 | |||
| Differences | p | 0.02 | 0.01 | 0.16 | ||
| 8 w | Marrow-dia | Mean | 24.6 * | 73.6 | 1.8 | |
| SD | 12.9 | 16.3 | 3.8 | |||
| Median | 21.6 | 78.5 | 0.0 | |||
| Marrow-meta | Mean | 25.1 * | 74.7 * | 0.2 * | ||
| SD | 9.6 | 9.7 | 0.4 | |||
| Median | 23.2 | 75.9 | 0.0 | |||
| Differences | p | 0.878 | 0.79 | 0.25 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soto-Peñaloza, D.; Caneva, M.; Viña-Almunia, J.; Martín-de-Llano, J.J.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Bone-Healing Pattern on the Surface of Titanium Implants at Cortical and Marrow Compartments in Two Topographic Sites: an Experimental Study in Rabbits. Materials 2019, 12, 85. https://doi.org/10.3390/ma12010085
Soto-Peñaloza D, Caneva M, Viña-Almunia J, Martín-de-Llano JJ, Peñarrocha-Oltra D, Peñarrocha-Diago M. Bone-Healing Pattern on the Surface of Titanium Implants at Cortical and Marrow Compartments in Two Topographic Sites: an Experimental Study in Rabbits. Materials. 2019; 12(1):85. https://doi.org/10.3390/ma12010085
Chicago/Turabian StyleSoto-Peñaloza, David, Marco Caneva, José Viña-Almunia, José Javier Martín-de-Llano, David Peñarrocha-Oltra, and Miguel Peñarrocha-Diago. 2019. "Bone-Healing Pattern on the Surface of Titanium Implants at Cortical and Marrow Compartments in Two Topographic Sites: an Experimental Study in Rabbits" Materials 12, no. 1: 85. https://doi.org/10.3390/ma12010085