Efficacy of CMX001 as a Prophylactic and Presymptomatic Antiviral Agent in New Zealand White Rabbits Infected with Rabbitpox Virus, a Model for Orthopoxvirus Infections of Humans

Abstract
:1. Introduction
2. Results and Discussion
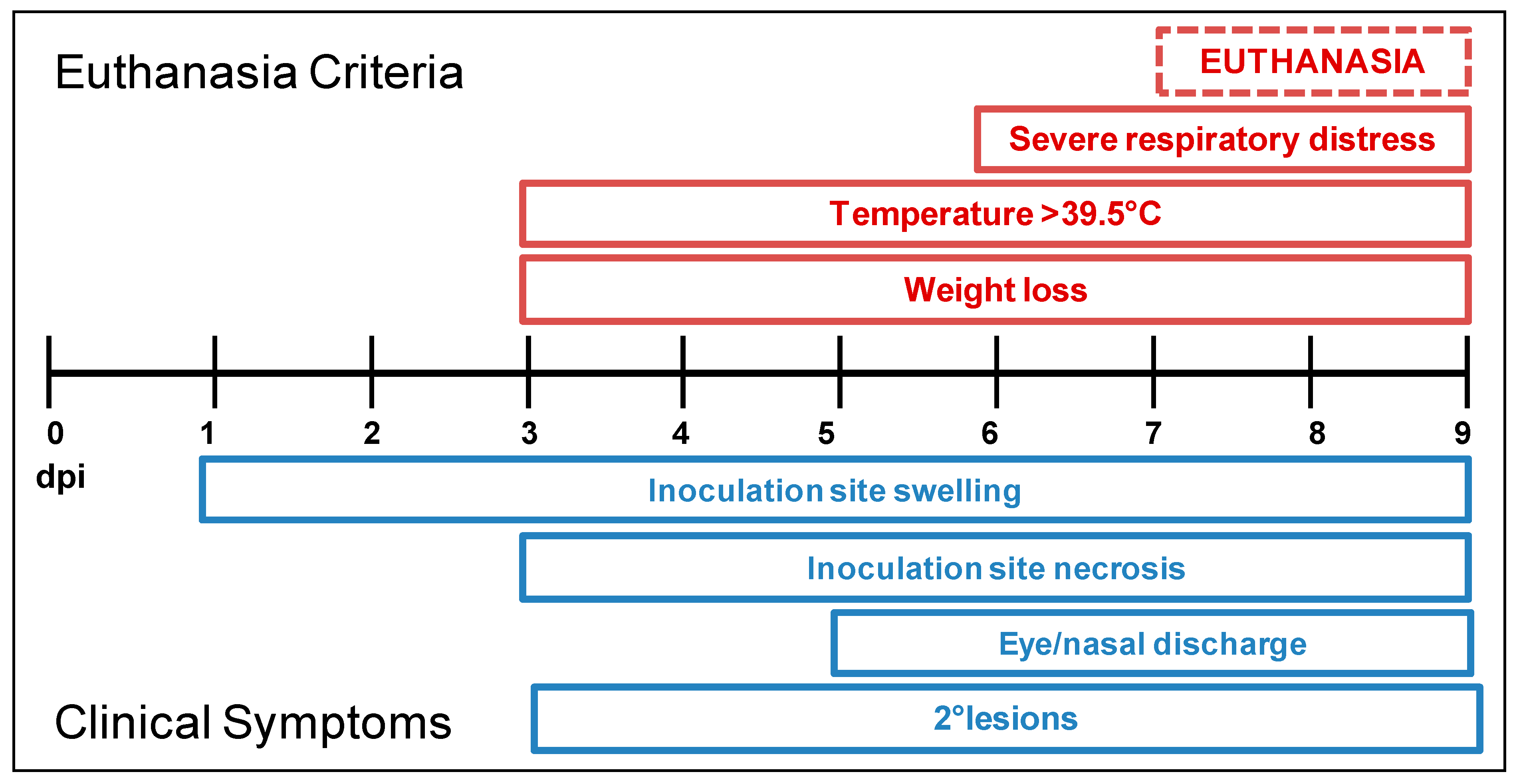
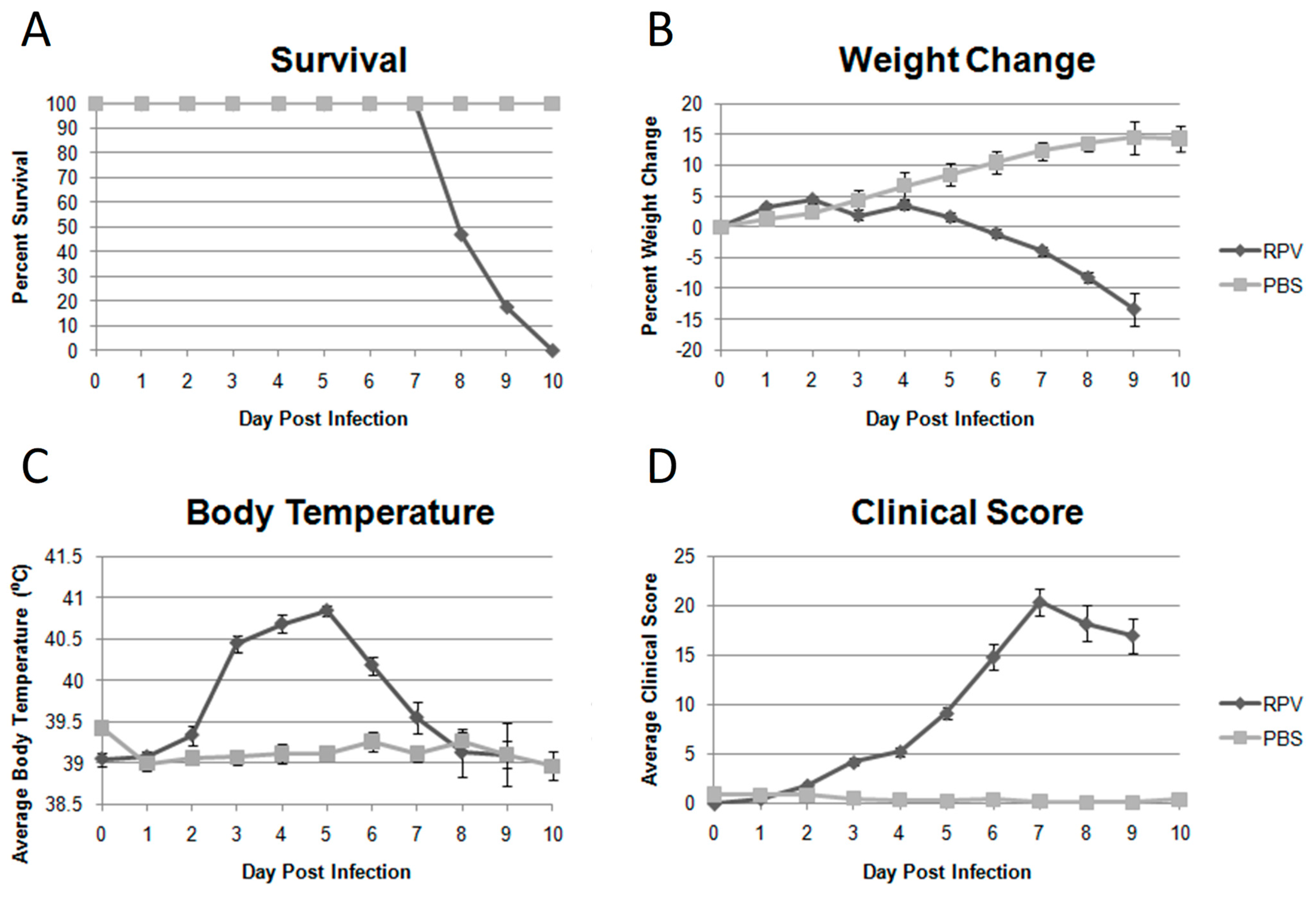
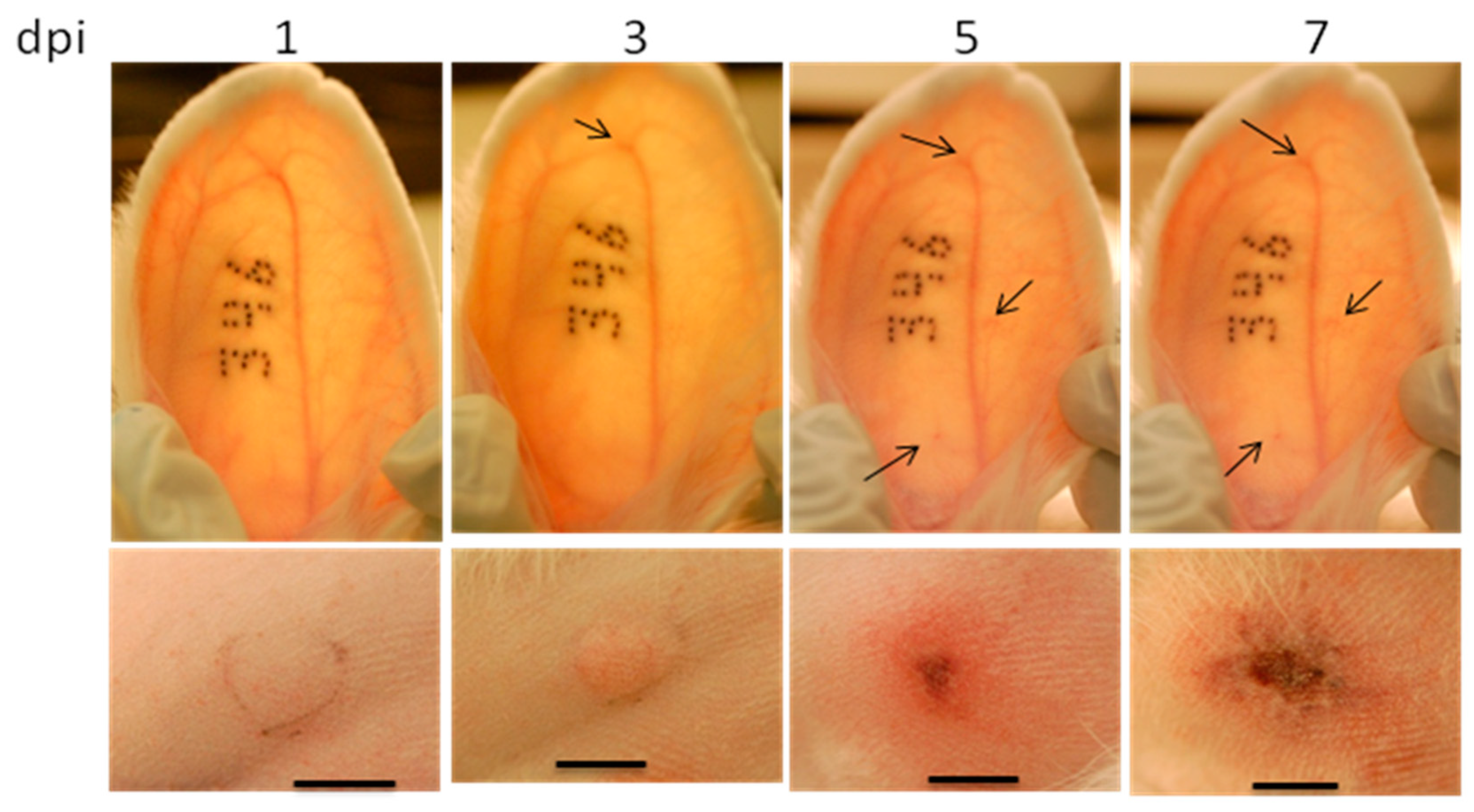
2.1. The Infection of Rabbits by Rabbitpox Virus: Model Review
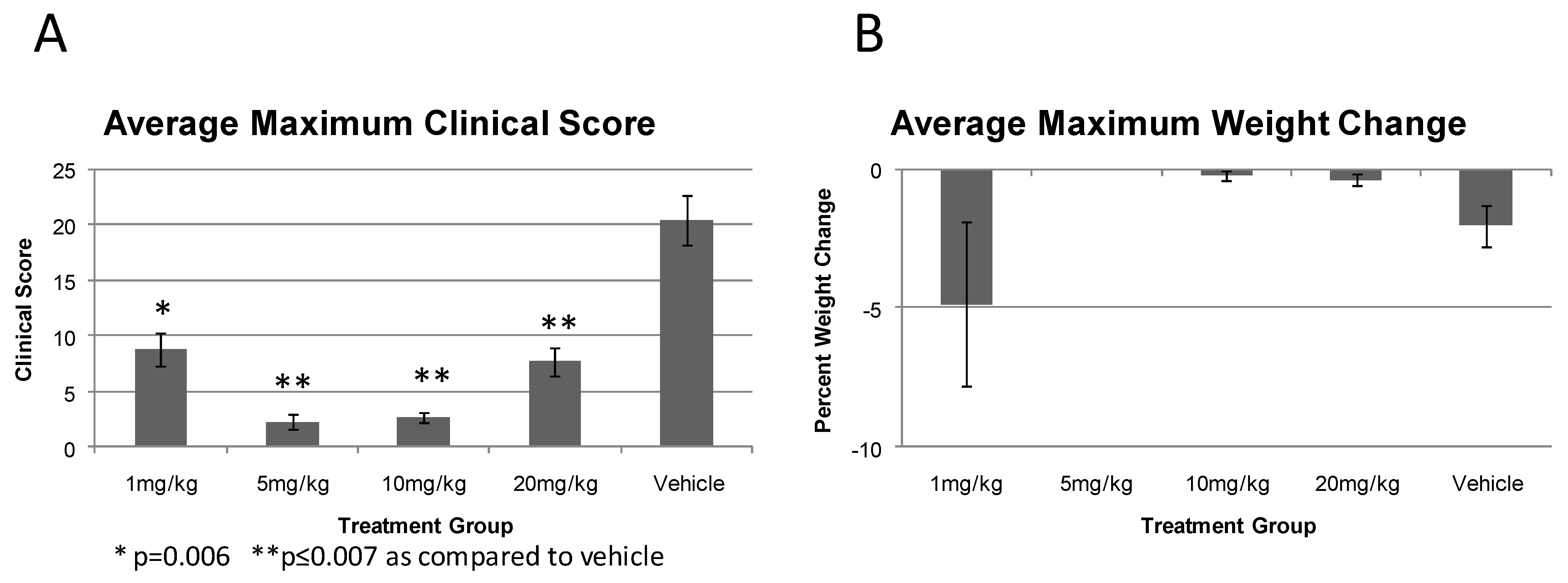
2.2. Efficacy of Prophylactic administration of CMX001 in Preventing RPV Induced Disease
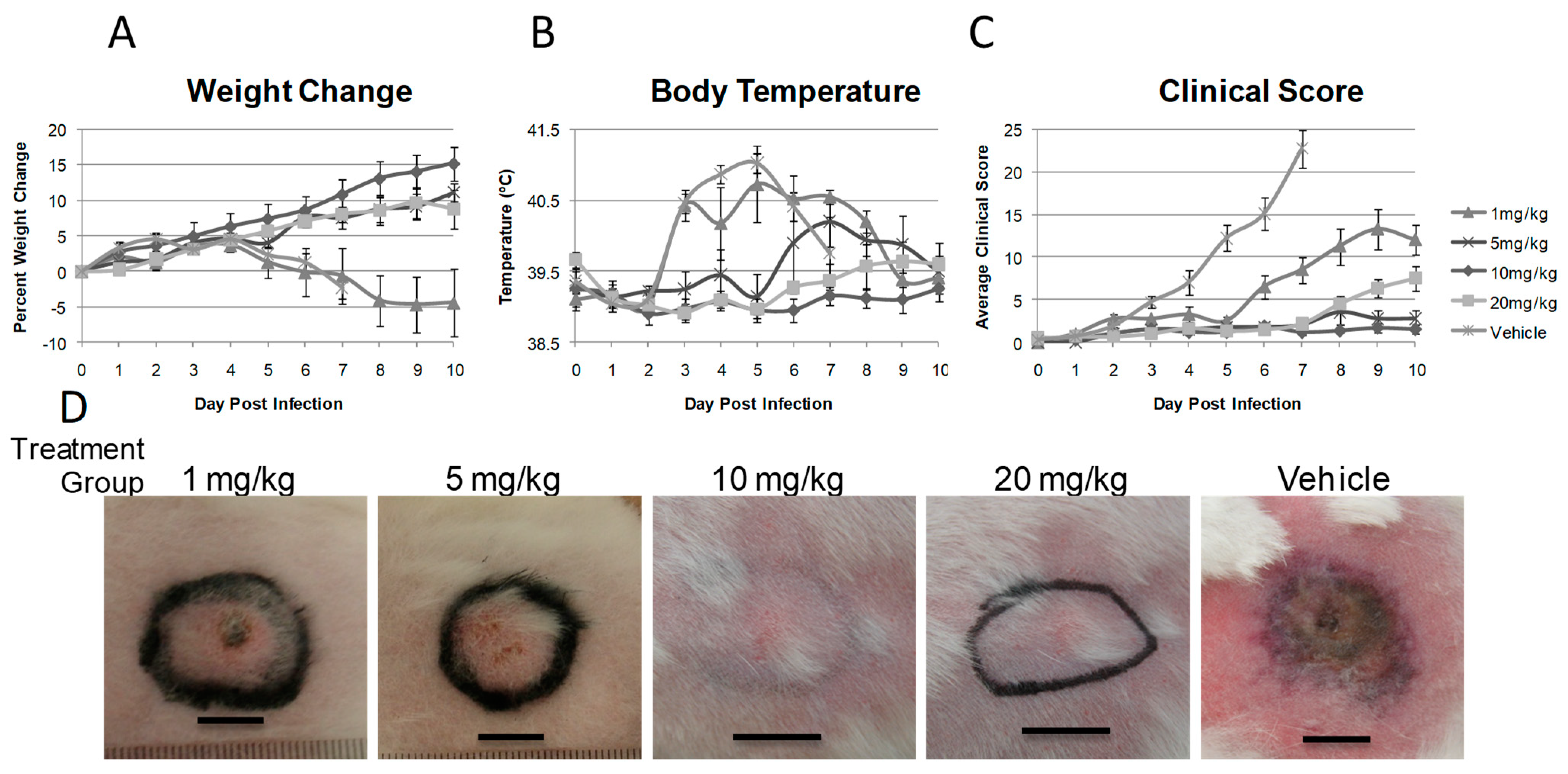
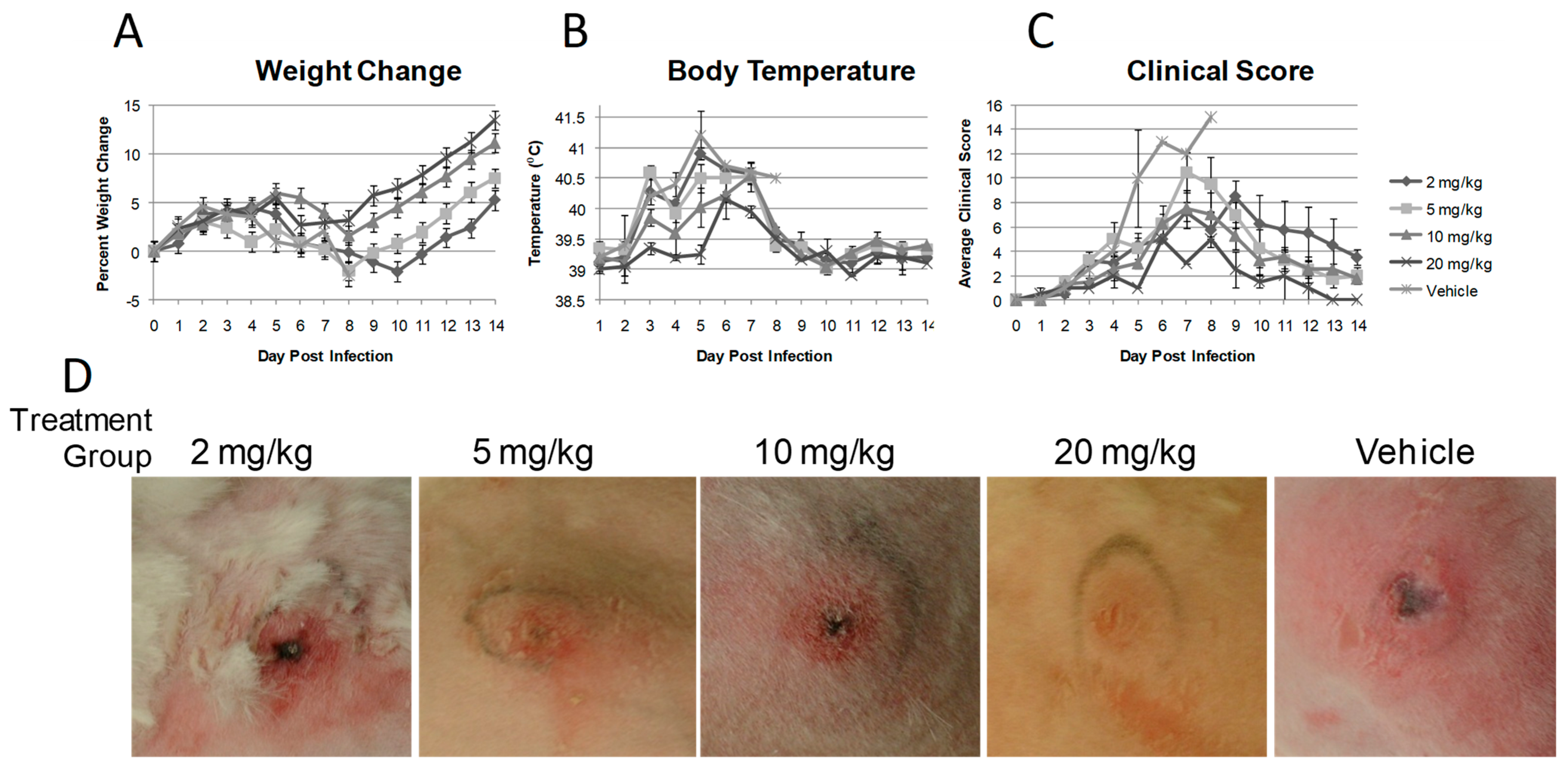
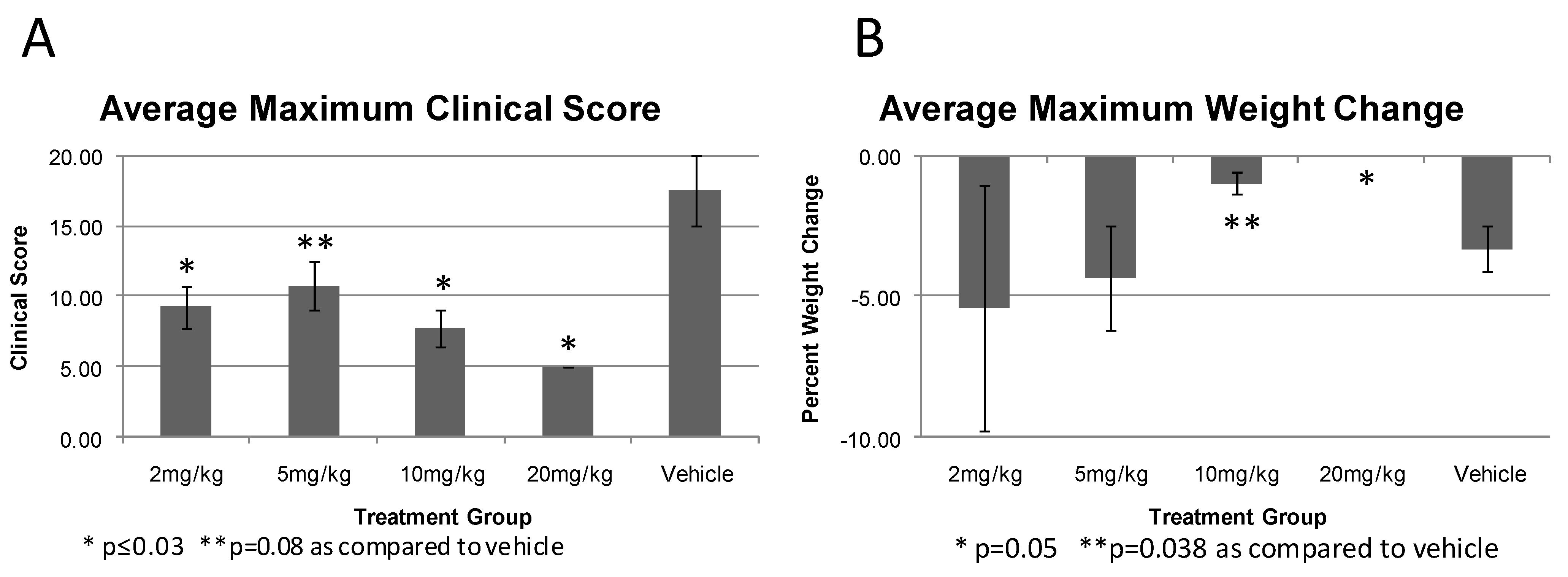
2.3. CMX001 Dose Response against RPV Infection
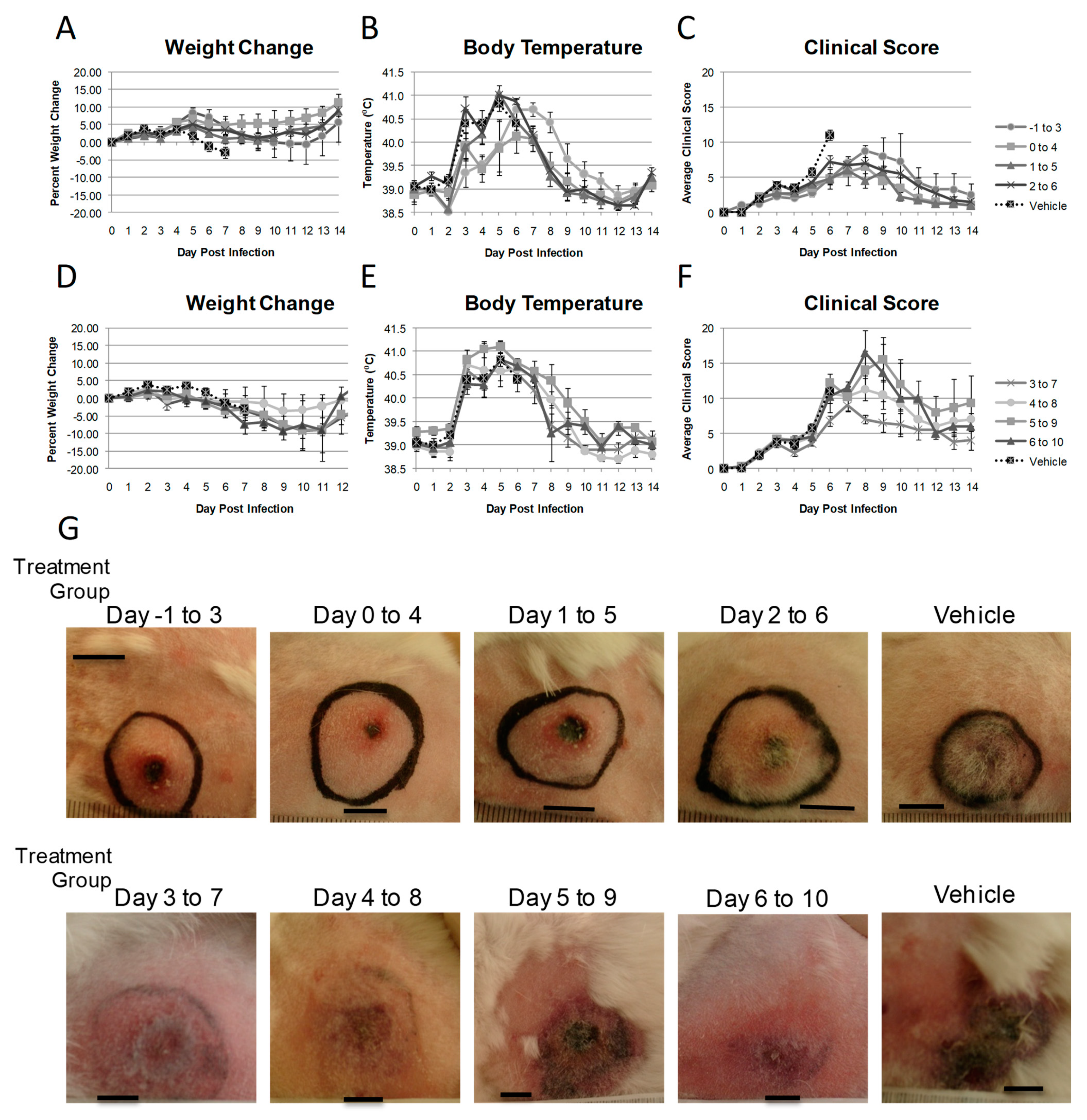
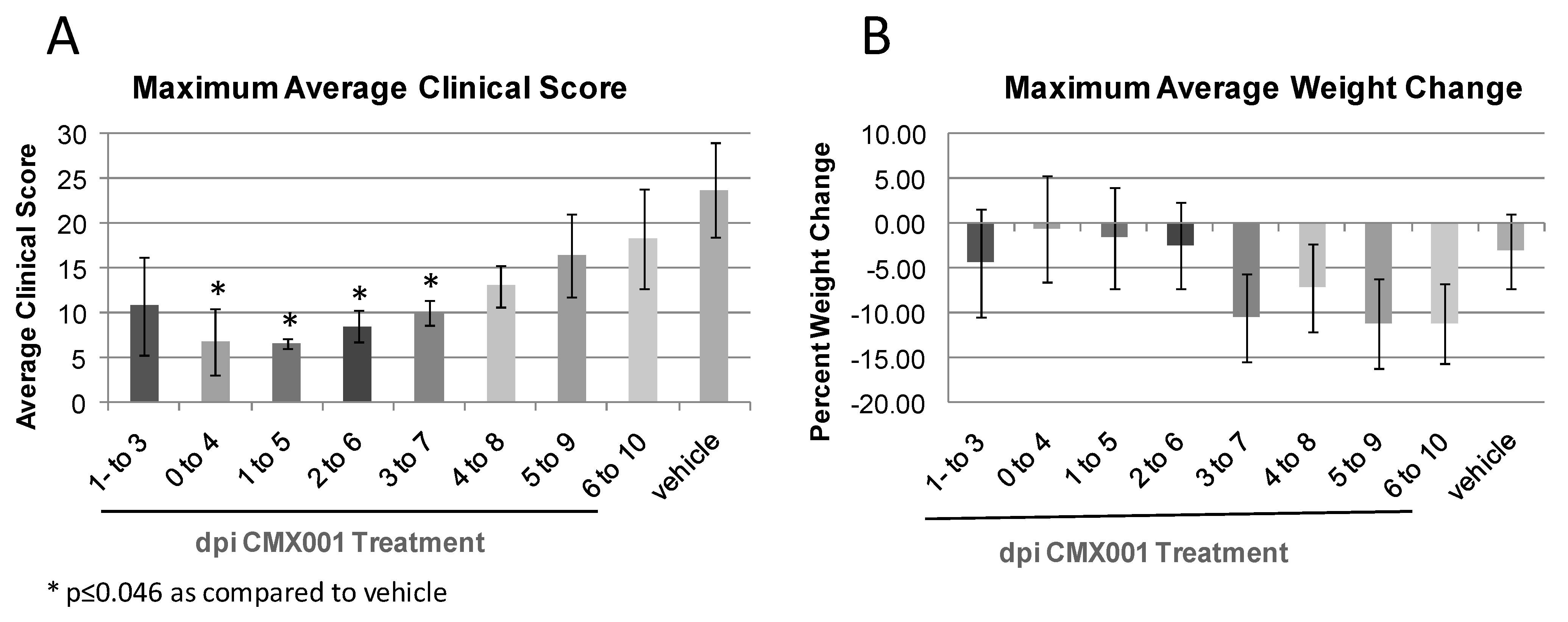
2.4. Comparison of CMX001 Treatment Time of Initiation
3. Experimental Section
3.1. Cell and Virus Growth
3.2. Housing of Animals
3.3. Animal Infections
3.4. Monitoring of Animals
3.5. CMX001 Dosing of Animals
4. Conclusions
Acknowledgements
References and Notes
- Henderson, D.A. Bioterrorism as a public health threat. Emerg. Infect. Dis. 1998, 4, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Henderson, D.A. Biopreparedness and public health. Am. J. Public Health 2001, 91, 1917–1919. [Google Scholar] [CrossRef] [PubMed]
- Bronze, M.S.; Huycke, M.M.; Machado, L.J.; Voskuhl, G.W.; Greenfield, R.A. Viral agents as biological weapons and agents of bioterrorism. Am. J. Med. Sci. 2002, 323, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration, HHS. New drug and biological drug products; evidence needed to demonstrate effectiveness of new drugs when human efficacy studies are not ethical or feasible. Final rule. Fed. Regist. 2002, 67, 37988–37998. [Google Scholar]
- Esposito, J.; Fenner, F. Poxviruses. In Fields Virology, 4th ed.; Knipe, D.E., Howley, P.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001; pp. 2885–2922. [Google Scholar]
- Jansen, J. Eperimenteel onderzoek van Kon-. ijnensterfte door een filtreebaar virus. Tijdschr. Diergeneeskd. 1942, 69, 505–514. [Google Scholar]
- Xing, K.; Deng, R.; Wang, J.; Feng, J.; Huang, M.; Wang, X. Genome-based phylogeny of poxvirus. Intervirology 2006, 49, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Gubser, C.; Hue, S.; Kellam, P.; Smith, G.L. Poxvirus genomes: A phylogenetic analysis. J. Gen. Virol. 2004, 85, 105–117. [Google Scholar] [CrossRef]
- Moss, B. Poxviridae and Their Replication. In Virology, 2nd ed.; Fields, B.N., Knipe, D.E., Eds.; Raven Press: New York, NY, USA, 1990; pp. 2079–2112. [Google Scholar]
- Moss, B. Poxviridae: The viruses and their replication. In Fields Virology, 3rd ed.; Fields, B.N., Knipe, D.M., Howley, P.M., Eds.; Lippincott-Reven: Philadelphia, PA, USA, 1996; Volume 2, pp. 2637–2672. [Google Scholar]
- Werden, S.J.; Rahman, M.M.; McFadden, G. Poxvirus host range genes. Adv. Virus Res. 2008, 71, 135–171. [Google Scholar]
- Li, Y.; Carroll, D.S.; Gardner, S.N.; Walsh, M.C.; Vitalis, E.A.; Damon, I.K. On the origin of smallpox: correlating variola phylogenics with historical smallpox records. Proc. Natl. Acad. Sci. U. S. A. 2007, 104, 15787–15792. [Google Scholar] [CrossRef]
- Chen, W.; Drillien, R.; Spehner, D.; Buller, R.M. Restricted replication of ectromelia virus in cell culture correlates with mutations in virus-encoded host range gene. Virology 1992, 187, 433–442. [Google Scholar] [CrossRef]
- Perkus, M.E.; Goebel, S.J.; Davis, S.W.; Johnson, G.P.; Limbach, K.; Norton, E.K.; Paoletti, E. Vaccinia virus host range genes. Virology 1990, 179, 276–286. [Google Scholar] [CrossRef]
- Fenner, F.; Henderson, D.A.; Arita, I.; Jezek, Z.; Ladnyi, I.D. The pathogenesis, pathology and immunology of smallpox and vaccinia. In Smallpox and Its Eradication; World Health Organization: Geneva, Switzerland, 1988; pp. 121–168. [Google Scholar]
- Fenner, F.; Henderson, D.A.; Arita, I.; Jezek, Z.; Ladnyi, I.D. Variola virus and the other orthopoxviruses. In Smallpox and its Eradication; World Health Organization: Geneva, Switzerland, 1988; pp. 69–120. [Google Scholar]
- Li, G.; Chen, N.; Roper, R.L.; Feng, Z.; Hunter, A.; Danila, M.; Lefkowitz, E.J.; Buller, R.M.; Upton, C. Complete coding sequences of the rabbitpox virus genome. J. Gen. Virol. 2005, 86, 2969–2977. [Google Scholar] [CrossRef] [PubMed]
- Bedson, H.S.; Duckworth, M.J. Rabbit pox: An experimental study of the pathways of infection in rabbits. J. Pathol. Bacteriol. 1963, 85, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.M.; Rice, A.D.; Moyer, R.W. Rabbitpox virus and vaccinia virus infection of rabbits as a model for human smallpox. J.Virol. 2007, 81, 11084–11095. [Google Scholar] [CrossRef]
- Westwood, J.C.; Boulter, E.A.; Bowen, E.T.; Maber, H.B. Experimental respiratory infection with poxviruses. I. Clinical virological and epidemiological studies. Br. J. Exp. Pathol. 1966, 47, 453–465. [Google Scholar]
- Wehrle, P.F.; Posch, J.; Richter, K.H.; Henderson, D.A. An airborne outbreak of smallpox in a German hospital and its significance with respect to other recent outbreaks in Europe. Bull. World Health Organ. 1970, 43, 669–679. [Google Scholar]
- Nalca, A.; Hatkin, J.M.; Garza, N.L.; Nichols, D.K.; Norris, S.W.; Hruby, D.E.; Jordan, R. Evaluation of orally delivered ST-246 as postexposure prophylactic and antiviral therapeutic in an aerosolized rabbitpox rabbit model. Antivir. Res. 2008, 79, 121–127. [Google Scholar] [CrossRef]
- Garza, N.L.; Hatkin, J.M.; Livingston, V.; Nichols, D.K.; Chaplin, P.J.; Volkmann, A.; Fisher, D.; Nalca, A. Evaluation of the efficacy of modified vaccinia Ankara (MVA)/IMVAMUNE against aerosolized rabbitpox virus in a rabbit model. Vaccine 2009, 27, 5496–5504. [Google Scholar] [CrossRef] [PubMed]
- FDA grants marketing clearance of Vistide for the treatment of CMV retinitis. AIDS Patient Care STDS 1996, 10, 383–384.
- Food and Drug Administration. FDA approves cidofovir for treatment of CMV retinitis. J. Int. Assoc. Physicians AIDS Care 1996, 2, 30. [Google Scholar]
- Bray, M.; Martinez, M.; Smee, D.F.; Kefauver, D.; Thompson, E.; Huggins, J.W. Cidofovir protects mice against lethal aerosol or intranasal cowpox virus challenge. J. Infect. Dis. 2000, 181, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Smee, D.F.; Sidwell, R.W.; Kefauver, D.; Bray, M.; Huggins, J.W. Characterization of wild-type and cidofovir-resistant strains of camelpox, cowpox, monkeypox, and vaccinia viruses. Antimicrob. Agents Chemother. 2002, 46, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Bray, M.; Huggins, J.W. Potential antiviral therapeutics for smallpox, monkeypox and other orthopoxvirus infections. Antivir. Res. 2003, 57, 13–23. [Google Scholar] [CrossRef]
- Kornbluth, R.S.; Smee, D.F.; Sidwell, R.W.; Snarsky, V.; Evans, D.H.; Hostetler, K.Y. Mutations in the E9L polymerase gene of cidofovir-resistant vaccinia virus strain WR are associated with the drug resistance phenotype. Antimicrob. Agents Chemother. 2006, 50, 4038–4043. [Google Scholar] [CrossRef]
- Magee, W.C.; Hostetler, K.Y.; Evans, D.H. Mechanism of inhibition of vaccinia virus DNA polymerase by cidofovir diphosphate. Antimicrob. Agents Chemother. 2005, 49, 3153–3162. [Google Scholar] [CrossRef]
- Araya, C.E.; Lew, J.F.; Fennell, R.S.; Neiberger, R.E.; Dharnidharka, V.R. Intermediate dose cidofovir does not cause additive nephrotoxicity in BK virus allograft nephropathy. Pediatr. Transplant. 2008, 12, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Ciesla, S.L.; Trahan, J.; Wan, W.B.; Beadle, J.R.; Aldern, K.A.; Painter, G.R.; Hostetler, K.Y. Esterification of cidofovir with alkoxyalkanols increases oral bioavailability and diminishes drug accumulation in kidney. Antivir. Res. 2003, 59, 163–171. [Google Scholar] [CrossRef]
- Painter, G.R.; Hostetler, K.Y. Design and development of oral drugs for the prophylaxis and treatment of smallpox infection. Trends Biotechnol. 2004, 22, 423–427. [Google Scholar] [CrossRef]
- Foster, S. Chimerix, Inc: Durham, NC, USA, Unpublished work. 2010.
- Hostetler, K.Y. Alkoxyalkyl prodrugs of acyclic nucleoside phosphonates enhance oral antiviral activity and reduce toxicity: current state of the art. Antivir. Res. 2009, 82, A84–A98. [Google Scholar] [CrossRef]
- Hostetler, K.Y.; Beadle, J.R.; Trahan, J.; Aldern, K.A.; Owens, G.; Schriewer, J.; Melman, L.; Buller, R.M. Oral 1-O-octadecyl-2-O-benzyl-sn-glycero-3-cidofovir targets the lung and is effective against a lethal respiratory challenge with ectromelia virus in mice. Antivir. Res. 2007, 73, 212–218. [Google Scholar] [CrossRef]
- Quenelle, D.C.; Collins, D.J.; Wan, W.B.; Beadle, J.R.; Hostetler, K.Y.; Kern, E.R. Oral treatment of cowpox and vaccinia virus infections in mice with ether lipid esters of cidofovir. Antimicrob. Agents Chemother. 2004, 48, 404–412. [Google Scholar] [CrossRef]
- Smee, D.F.; Wong, M.H.; Bailey, K.W.; Beadle, J.R.; Hostetler, K.Y.; Sidwell, R.W. Effects of four antiviral substances on lethal vaccinia virus (IHD strain) respiratory infections in mice. Int. J. Antimicrob. Agents 2004, 23, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.R. Smallpox; The Kothari Book Depot: Bombay, India, 1972. [Google Scholar]
- Martin, D.B. The cause of death in smallpox: An examination of the pathology record. Mil. Med. 2002, 167, 546. [Google Scholar] [CrossRef] [PubMed]
- Jahrling, P.B.; Hensley, L.E.; Martinez, M.J.; Leduc, J.W.; Rubins, K.H.; Relman, D.A.; Huggins, J.W. Exploring the potential of variola virus infection of cynomolgus macaques as a model for human smallpox. Proc. Natl. Acad. Sci. U. S. A. 2004, 101, 15196–15200. [Google Scholar] [CrossRef] [PubMed]
- Stanford, M.M.; McFadden, G.; Karupiah, G.; Chaudhri, G. Immunopathogenesis of poxvirus infections: forecasting the impending storm. Immunol. Cell Biol. 2007, 85, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Boulter, E.A.; Maber, H.B.; Bowen, E.T. Studies on the physiological disturbances occurring in experimental rabbit pox: an approach to rational therapy. Br. J. Exp. Pathol. 1961, 42, 433–444. [Google Scholar] [PubMed]
- Boulter, E.A.; Westwood, J.C.; Maber, H.B. Value of serotherapy in a virus disease (rabbit pox). Lancet 1961, 2, 1012–1015. [Google Scholar] [CrossRef]
- Condit, R.C.; Motyczka, A. Isolation and preliminary characterization of temperature-sensitive mutants of vaccinia virus. Virology 1981, 113, 224–241. [Google Scholar] [CrossRef]
- Condit, R.C.; Motyczka, A.; Spizz, G. Isolation, characterization, and physical mapping of temperature-sensitive mutants of vaccinia virus. Virology 1983, 128, 429–443. [Google Scholar] [CrossRef]
- Jordon, R.; Leeds, J.M.; Tyavanagimatt, S.; Hruby, D.E. Development of ST-246 for Treatment of Poxvirus Infections. Viruses 2010, 2, 2409–2435. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CMX001 Dose (mg/kg) | Dosing Frequency | Day of Dosing (dpi) | Mean Time to Death ± SEM | Survival at Day 14PI |
|---|---|---|---|---|
| 1 | BID | −1 to 3 | NA | 4/4 (100%)* |
| 5 | BID | −1 to 3 | NA | 4/4 (100%)* |
| 10 | BID | −1 to 3 | NA | 6/6 (100%)** |
| 20 | QD | −1 to 3 | NA | 6/6 (100%)** |
| Vehicle | BID | −1 to 3 | 6.6 ± 0.16 | 0/10 (0%) |
| CMX001 Dose (mg/kg) | Dosing Frequency | Day of Dosing (dpi) | Mean Time to Death ± SEM | Survival at Day 14PI |
|---|---|---|---|---|
| 2 | QD | 1 to 5 | NA | 4/4 (100%)* |
| 5 | QD | 1 to 5 | NA | 4/4 (100%)* |
| 10 | QD | 1 to 5 | NA | 4/4 (100%)* |
| 20 | QD | 1 to 5 | NA | 2/2 (100%)** |
| Vehicle | QD | 1 to 5 | 7±1 | 0/2 (0%) |
| CMX001 Dose (mg/kg) | Frequency of Dosing | Day of Dosing (dpi) | Mean Time to Death ± SEM | Survival at Day 14PI |
|---|---|---|---|---|
| 5 | BID | −1 to 3 | NA | 4/4 (100%) |
| 5 | BID | 0 to 4 | NA | 4/4 (100%) |
| 5 | BID | 1 to 5 | NA | 4/4 (100%) |
| 5 | BID | 2 to 6 | NA | 4/4 (100%) |
| 5 | BID | 3 to 7 | NA | 4/4 (100%) |
| 5 | BID | 4 to 8 | NA | 4/4 (100%) |
| 5 | BID | 5 to 9 | 9 ± 0 | 3/4 (75%) |
| 5 | BID | 6 to 10 | 9.3 ± 0.9 | 1/4 (25%) |
| Vehicle | BID | Vehicle | 7 ± 0 | 0/4 (0%) |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rice, A.D.; Adams, M.M.; Lampert, B.; Foster, S.; Lanier, R.; Robertson, A.; Painter, G.; Moyer, R.W. Efficacy of CMX001 as a Prophylactic and Presymptomatic Antiviral Agent in New Zealand White Rabbits Infected with Rabbitpox Virus, a Model for Orthopoxvirus Infections of Humans. Viruses 2011, 3, 63-82. https://doi.org/10.3390/v3020063
Rice AD, Adams MM, Lampert B, Foster S, Lanier R, Robertson A, Painter G, Moyer RW. Efficacy of CMX001 as a Prophylactic and Presymptomatic Antiviral Agent in New Zealand White Rabbits Infected with Rabbitpox Virus, a Model for Orthopoxvirus Infections of Humans. Viruses. 2011; 3(2):63-82. https://doi.org/10.3390/v3020063
Chicago/Turabian StyleRice, Amanda D., Mathew M. Adams, Bernhard Lampert, Scott Foster, Randall Lanier, Alice Robertson, George Painter, and Richard W. Moyer. 2011. "Efficacy of CMX001 as a Prophylactic and Presymptomatic Antiviral Agent in New Zealand White Rabbits Infected with Rabbitpox Virus, a Model for Orthopoxvirus Infections of Humans" Viruses 3, no. 2: 63-82. https://doi.org/10.3390/v3020063
APA StyleRice, A. D., Adams, M. M., Lampert, B., Foster, S., Lanier, R., Robertson, A., Painter, G., & Moyer, R. W. (2011). Efficacy of CMX001 as a Prophylactic and Presymptomatic Antiviral Agent in New Zealand White Rabbits Infected with Rabbitpox Virus, a Model for Orthopoxvirus Infections of Humans. Viruses, 3(2), 63-82. https://doi.org/10.3390/v3020063