
The Effectiveness of Educational Interventions in Improving Waste Management Knowledge, Attitudes, and Practices among Healthcare Workers: A Systematic Review and Meta-Analysis

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Article Screening and Study Selection
2.5. Quality Appraisal
2.6. Data Extraction
2.7. Interventions and Assessment Methods
2.8. Data Synthesis and Statistical Analysis
3. Results
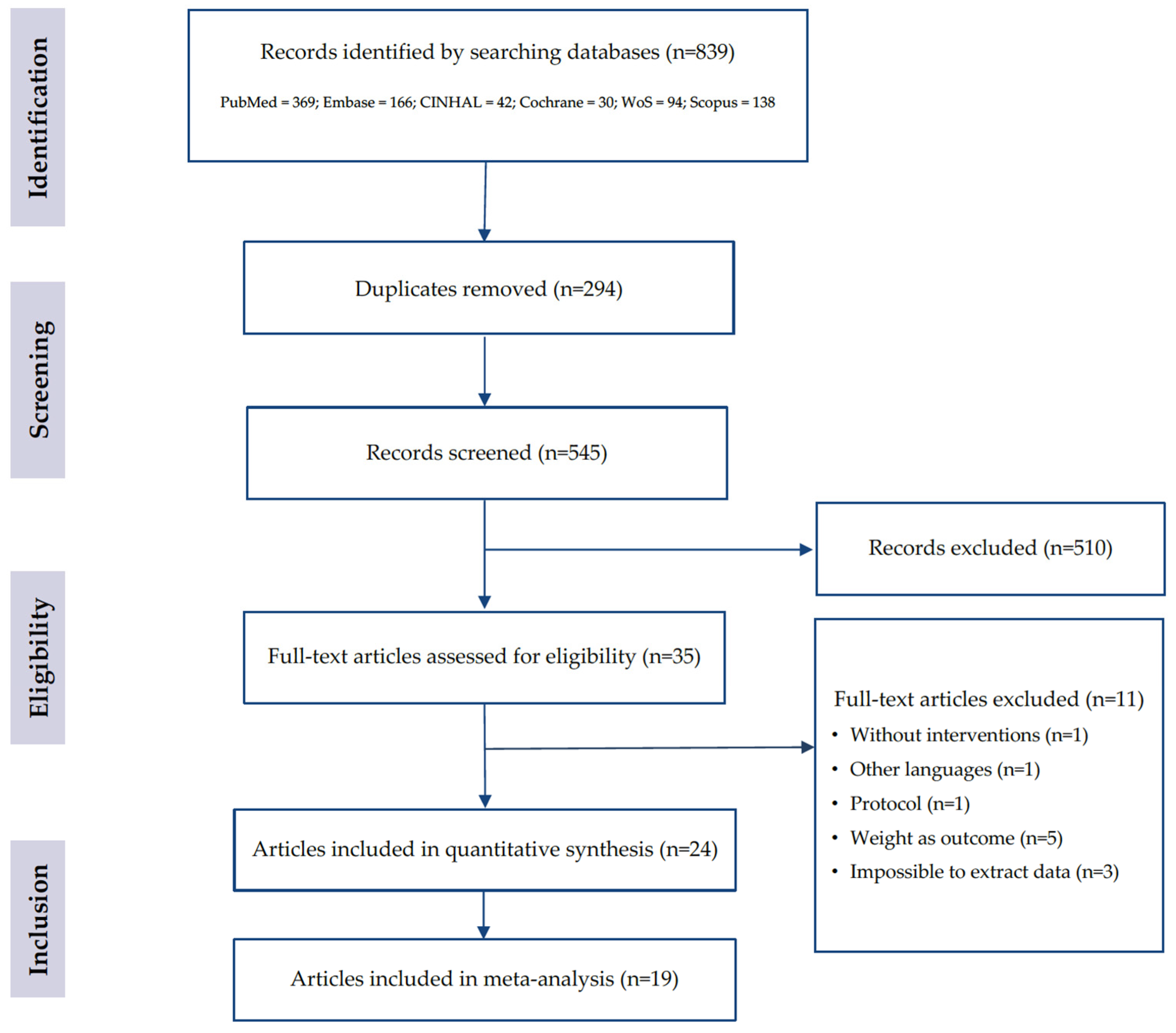
3.1. Articles Included
3.2. Characteristics of Studies Included
3.3. Types of Educational Interventions to Improve Waste Management among HCWs
3.3.1. Mono-Component Educational Interventions
Lessons
Audits
Technology
3.3.2. Multi-Component Educational Interventions
Lessons and Training
Lessons/Audits and System Change
Lessons, Training, and Reminders
Lessons, Training, System Change, and Reminders
3.4. Assessment of Educational Interventions to Improve Waste Management among HCWs
3.5. Study Quality
3.6. Efficacy of Educational Interventions to Improve Waste Management among HCWs
3.6.1. Efficacy of Educational Interventions in Improving Knowledge among HCWs
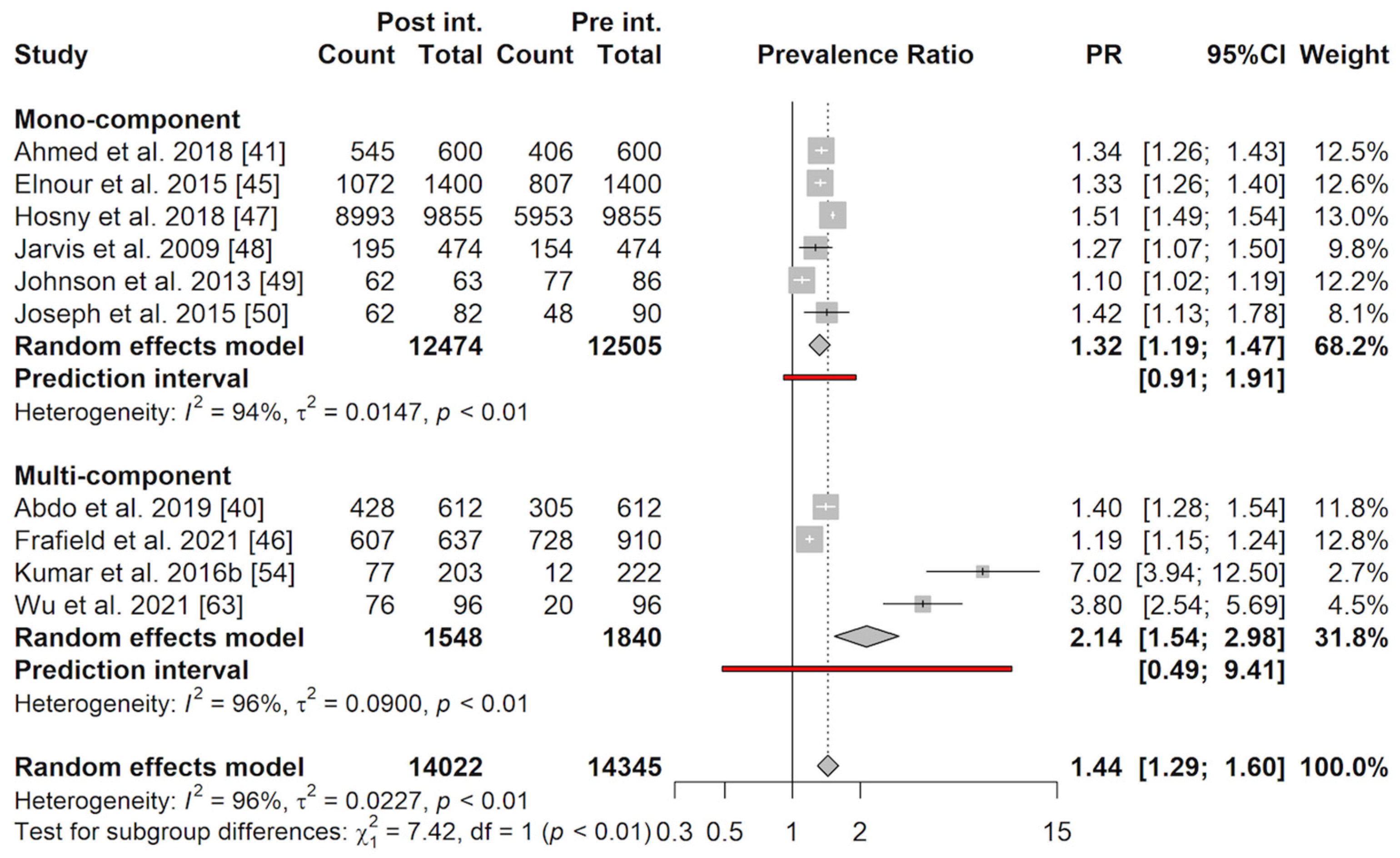
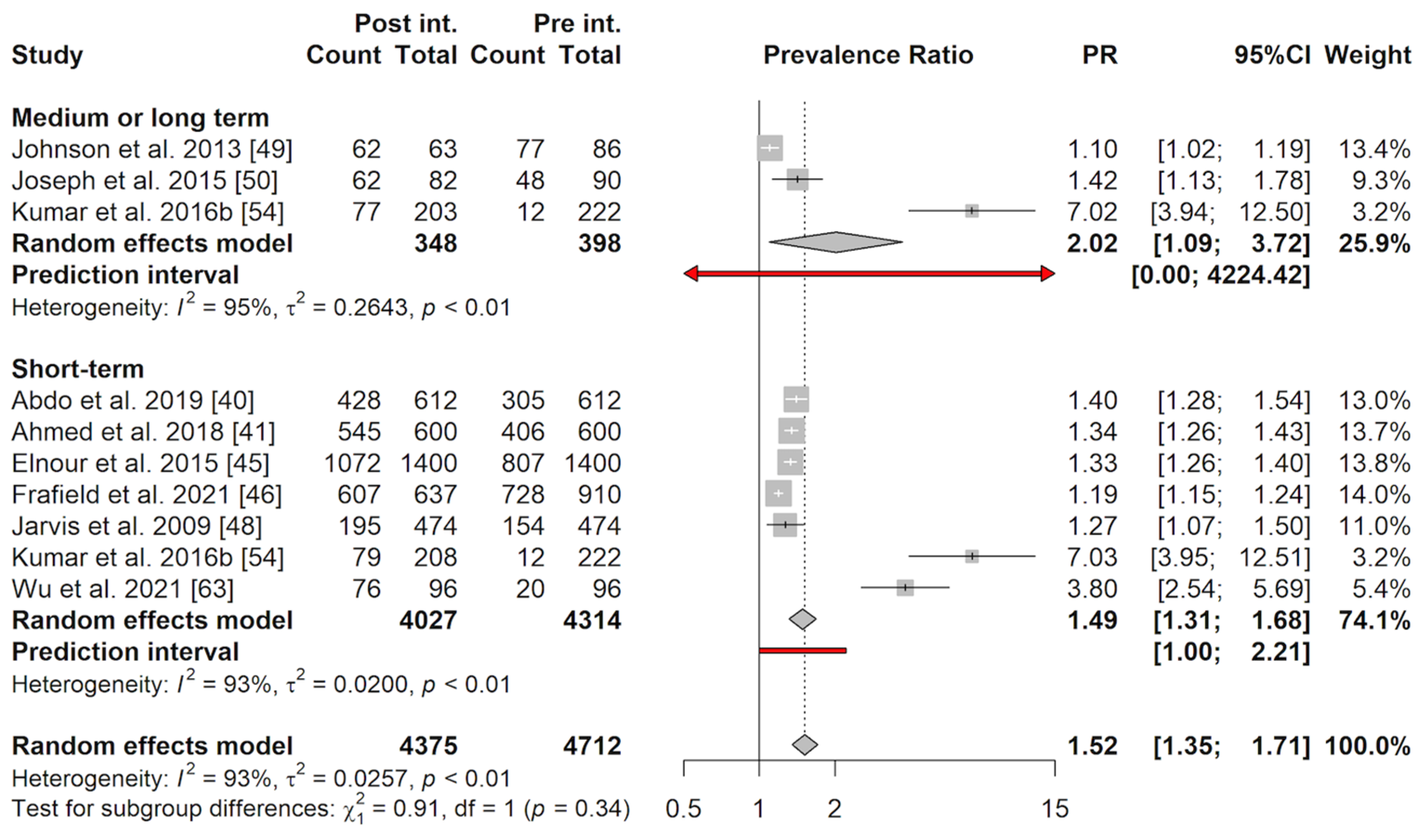
3.6.2. Efficacy of Educational Interventions in Improving Practices among HCWs
3.6.3. Efficacy of Educational Interventions in Improving Attitudes among HCWs
3.7. Publication Bias and Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Health Care without Harm. Arup Health Care Climate Footprint Report—How the Health Sector Contributes to the Global Climate Crisis and Opportunities for Action; Climate-Smart Health Care Series; Health Care without Harm: Washington, DC, USA, 2019. [Google Scholar]
- Lattanzio, S.; Stefanizzi, P.; D’ambrosio, M.; Cuscianna, E.; Riformato, G.; Migliore, G.; Tafuri, S.; Bianchi, F.P. Waste Management and the Perspective of a Green Hospital—A Systematic Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 15812. [Google Scholar] [CrossRef] [PubMed]
- United Nations Environment Programme (UNEP). Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and Their Disposal. Available online: https://eur-lex.europa.eu/EN/legal-content/summary/basel-convention-on-the-control-of-transboundary-movements-of-hazardous-wastes-and-their-disposal.html (accessed on 6 February 2024).
- U.S. Environmental Protection Agency. EPA’s Report on the Environment (ROE) (2008 Final Report); U.S. Environmental Protection Agency: Washington, DC, USA, 2008. [Google Scholar]
- World Health Organization. Safe Management of Wastes from Health-Care Activities, 2nd ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Health-Care Waste. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 6 February 2024).
- World Health Organization. Global Analysis of Health Care Waste in the Context of COVID-19: Status, Impacts and Recommendations; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Andeobu, L.; Wibowo, S.; Grandhi, S. Medical Waste from COVID-19 Pandemic—A Systematic Review of Management and Environmental Impacts in Australia. Int. J. Environ. Res. Public Health 2022, 19, 1381. [Google Scholar] [CrossRef] [PubMed]
- United Nations Environment Programme. Compendium of Technologies for Treatment/Destruction of Healthcare Waste; United Nations Environment Programme: Nairobi, Kenya, 2012. [Google Scholar]
- World Health Organization. Safe Management of Wastes from Health-Care Activities: A Summary; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Anåker, A.; Elf, M. Sustainability in Nursing: A Concept Analysis. Scand. J. Caring Sci. 2014, 28, 381–389. [Google Scholar] [CrossRef] [PubMed]
- McMillan, K. Sustainability: An Evolutionary Concept Analysis. Exploring Nursing’s Role within the Sustainability Movement. J. Adv. Nurs. 2014, 70, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Fields, L.; Moroney, T.; Perkiss, S.; Dean, B.A. Enlightening and Empowering Students to Take Action: Embedding Sustainability into Nursing Curriculum. J. Prof. Nurs. 2023, 49, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Caniato, M.; Tudor, T.; Vaccari, M. International Governance Structures for Health-Care Waste Management: A Systematic Review of Scientific Literature. J. Environ. Manag. 2015, 153, 93–107. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, D. Effective Medical Waste Management for Sustainable Green Healthcare. Int. J. Environ. Res. Public Health 2022, 19, 14820. [Google Scholar] [CrossRef] [PubMed]
- Torres-Pereda, P.; Parra-Tapia, E.; Rodríguez, M.A.; Félix-Arellano, E.; Riojas-Rodríguez, H. Impact of an Intervention for Reducing Waste through Educational Strategy: A Mexican Case Study, What Works, and Why? Waste Manag. 2020, 114, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Kenny, C.; Priyadarshini, A. Review of Current Healthcare Waste Management Methods and Their Effect on Global Health. Healthcare 2021, 9, 284. [Google Scholar] [CrossRef]
- Thakur, V.; Ramesh, A. Healthcare Waste Management Research: A Structured Analysis and Review (2005–2014). Waste Manag. Res. 2015, 33, 855–870. [Google Scholar] [CrossRef]
- McGain, F.; Naylor, C. Environmental Sustainability in Hospitals—A Systematic Review and Research Agenda. J. Health Serv. Res. Policy 2014, 19, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Barnett-Itzhaki, Z.; Berman, T.; Grotto, I.; Schwartzberg, E. Household Medical Waste Disposal Policy in Israel. Isr. J. Health Policy Res. 2016, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Capoor, M.R.; Bhowmik, K.T. Current Perspectives on Biomedical Waste Management: Rules, Conventions and Treatment Technologies. Indian J. Med. Microbiol. 2017, 35, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Fadaei, A. Comparison of Medical Waste Management Methods in Different Countries: A Systematic Review. Rev. Environ. Health 2023, 38, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.A.; Parvin, F. Examining Challenges and Multi-Strategic Approaches in Waste Management during the COVID-19 Pandemic: A Systematic Review. Waste Manag. Res. 2022, 40, 1356–1380. [Google Scholar] [CrossRef] [PubMed]
- Yazie, T.D.; Tebeje, M.G.; Chufa, K.A. Healthcare Waste Management Current Status and Potential Challenges in Ethiopia: A Systematic Review. BMC Res. Notes 2019, 12, 285. [Google Scholar] [CrossRef] [PubMed]
- Cutter, J.; Gammon, J. Review of Standard Precautions and Sharps Management in the Community. Br. J. Community Nurs. 2007, 12, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.; Menon, V.; Ameen, S.; Kumar Praharaj, S. Designing and Conducting Knowledge, Attitude, and Practice Surveys in Psychiatry: Practical Guidance. Indian J. Psychol. Med. 2020, 42, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.H. Introduction to Health Research Methods: A Practical Guide; Jones & Bartlett Learning: Burlington, MA, USA, 2020; ISBN 978-1-284-19756-3. [Google Scholar]
- World Health Organization. Stop TB Partnership Advocacy, Communication and Social Mobilization (ACSM) for Tuberculosis Control. Available online: https://www.who.int/publications-detail-redirect/9789241596183 (accessed on 6 February 2024).
- Ashtari, A.; Sadegh Tabrizi, J.; Rezapour, R.; Rashidian Maleki, M.; Azami-Aghdash, S. Health Care Waste Management Improvement Interventions Specifications and Results: A Systematic Review and Meta-Analysis. Iran J. Public Health 2020, 49, 1611–1621. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid.-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of Study Quality for Systematic Reviews: A Comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological Research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.; Sakarovitch, C. Evaluating Non-Randomised Intervention Studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Clopper, C.J.; Pearson, E.S. The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and Influence Diagnostics for Meta-Analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 6 February 2024).
- Abdo, N.M.; Hamza, W.S.; Al-Fadhli, M.A. Effectiveness of Education Program on Hospital Waste Management. Int. J. Workplace Health Manag. 2019, 12, 457–468. [Google Scholar] [CrossRef]
- Ahmed, M.D.M.; Usman, S.T.S.; Abida, H. Impact of Biomedical Waste Management Training Intervention on Knowledge, Attitude and Practices of Health Care Workers in Telangana. Indian J. Public Health Res. Dev. 2018, 9, 46–49. [Google Scholar] [CrossRef]
- Ara, L.; Vashkar, S.M.K.; Mowla, S.M.N.; Hossain, D. Role of Education in Improving Competencies of Nurses to Infection Control, Delivering Healthcare and Decreasing Occupational Hazards in Bangladesh. Am. J. Infect. Control 2015, 43, S4. [Google Scholar] [CrossRef]
- Ara, L.; Billah, W.; Bashar, F.; Mahmud, S.; Amin, A.; Iqbal, R.; Rahman, T.; Alam, N.H.; Sarker, S.A. Effectiveness of a Multi-Modal Capacity-Building Initiative for Upgrading Biomedical Waste Management Practices at Healthcare Facilities in Bangladesh: A 21st Century Challenge for Developing Countries. J. Hosp. Infect. 2022, 121, 49–56. [Google Scholar] [CrossRef] [PubMed]
- El-Gilany, A.-H.; El-Shaer, S.; Khashaba, E.; El-Dakroory, S.A.; Omar, N. Knowledge, Attitude, and Practice (KAP) of “teaching Laboratory” Technicians towards Laboratory Safety and Waste Management: A Pilot Interventional Study. J. Hosp. Infect. 2017, 96, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Elnour, A.M.; Moussa, M.M.R.; El-Borgy, M.D.; Fadelella, N.E.E.; Mahmoud, A.H. Impacts of Health Education on Knowledge and Practice of Hospital Staff with Regard to Healthcare Waste Management at White Nile State Main Hospitals, Sudan. Int. J. Health Sci. 2015, 9, 315–331. [Google Scholar] [CrossRef]
- Fraifeld, A.; Rice, A.N.; Stamper, M.J.; Muckler, V.C. Intraoperative Waste Segregation Initiative among Anesthesia Personnel to Contain Disposal Costs. Waste Manag. 2021, 122, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Hosny, G.; Samir, S.; El-Sharkawy, R. An Intervention Significantly Improve Medical Waste Handling and Management: A Consequence of Raising Knowledge and Practical Skills of Health Care Workers. Int. J. Health Sci. 2018, 12, 56–66. [Google Scholar]
- Jarvis, C.I.; Seed, S.M.; Silva, M.; Sullivan, K.M. Educational Campaign for Proper Medication Disposal. J. Am. Pharm. Assoc. 2009, 49, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.M.; González, M.L.; Dueñas, L.; Gamero, M.; Relyea, G.; Luque, L.E.; Caniza, M.A. Improving Waste Segregation While Reducing Costs in a Tertiary-Care Hospital in a Lower-Middle-Income Country in Central America. Waste Manag. Res. 2013, 31, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Joseph, L.; Paul, H.; Premkumar, J.; Rabindranath; Paul, R.; Michael, J.S. Biomedical Waste Management: Study on the Awareness and Practice among Healthcare Workers in a Tertiary Teaching Hospital. Indian J. Med. Microbiol. 2015, 33, 129–131. [Google Scholar] [CrossRef]
- Krishnan, K.U.; Devamani, T.S.D.; Jayalakshmi, G. On the Path of Continual Improvement: An Evaluation of Biomedical Waste Management Training. Indian J. Med. Microbiol. 2015, 33, S119–S121. [Google Scholar] [CrossRef]
- Kumar, R.; Somrongthong, R.; Shaikh, B.T. Effectiveness of Intensive Healthcare Waste Management Training Model among Health Professionals at Teaching Hospitals of Pakistan: A Quasi-Experimental Study. BMC Health Serv. Res. 2015, 15, 81. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Somrongthong, R.; Ahmed, J. Impact of Waste Management Training Intervention on Knowledge, Attitude and Practices of Teaching Hospital Workers in Pakistan. Pak. J. Med. Sci. 2016, 32, 705–710. [Google Scholar] [CrossRef]
- Kumar, R.; Somrongthong, R.; Ahmed, J. Effect of Medical Waste Management Trainings on Behavior Change among Doctors versus Nurses and Paramedical Staff in Pakistan. J. Ayub Med. Coll. Abbottabad. 2016, 28, 493–496. [Google Scholar] [PubMed]
- Ozder, A.; Teker, B.; Eker, H.H.; Altındis, S.; Kocaakman, M.; Karabay, O. Medical Waste Management Training for Healthcare Managers—A Necessity? J. Environ. Health Sci. Eng. 2013, 11, 20. [Google Scholar] [CrossRef] [PubMed]
- Robat, D.S.; Sany, S.B.T.; Siuki, H.A.; Peyman, N.; Ferns, G. Impact of an Educational Training on Behavioral Intention for Healthcare Waste Management: Application of Health Action Model. Community Health Equity Res. Policy 2022, 42, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Rohilla, R.; Gupta, P.K.; Narula, H.; Sharma, A.K.; Mehta, V.; Rao, S.; Gupta, J.; Gupta, P. Assessment of Cognitive and Psychomotor Domains Regarding Biomedical Waste Management and Hand Hygiene among Various Categories of Health-Care Professionals at a Tertiary Care Center in Northern India. J. Educ. Health Promot. 2021, 10, 186. [Google Scholar] [CrossRef] [PubMed]
- Sapkota, B.; Gupta, G.K.; Mainali, D. Impact of Intervention on Healthcare Waste Management Practices in a Tertiary Care Governmental Hospital of Nepal. BMC Public Health 2014, 14, 1005. [Google Scholar] [CrossRef]
- Shaheen, T.; Ghani, M.; Kausar, S. Gauging the Effectiveness of Training Sessions among Nurses Regarding Biomedical Waste Management: A Quasi-Experimental Study from a Developing Country. Cureus 2020, 12, e12196. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Dhillon, B.S.; Shrivastava, A.K.; Kumar, B.; Bhattacharya, S. Effectiveness of a Training Program about Bio-Medical Waste Management on the Knowledge and Practices of Health-Care Professionals at a Tertiary Care Teaching Institute of North India. J. Educ. Health Promot. 2020, 9, 127. [Google Scholar] [CrossRef]
- Tabash, M.I.; Hussein, R.A.; Mahmoud, A.H.; El-Borgy, M.D.; Abu-Hamad, B.A. Impact of an Intervention Programme on Knowledge, Attitude and Practice of Healthcare Staff Regarding Pharmaceutical Waste Management, Gaza, Palestine. Public Health 2016, 138, 127–137. [Google Scholar] [CrossRef]
- Tabrizi, J.S.; Saadati, M.; Heydari, M.; Rezapour, R.; Zamanpour, R. Medical Waste Management Improvement in Community Health Centers: An Interventional Study in Iran. Prim. Health Care Res. Dev. 2018, 20, e66. [Google Scholar] [CrossRef]
- Wu, S.-H.; Yang, Y.-Y.; Huang, C.-C.; Liu, C.-W.; Yang, L.-Y.; Chen, C.-H.; Kao, S.-Y.; Lee, F.-Y. Virtual Reality Simulation Increases Chinese Physicians’ and Lab Technicians’ Familiarity and Confidence Regarding Proper Clinical Wastes Segregation/Disposal: A 2-Year Pilot Study. BMJ Simul. Technol. Enhanc. Learn. 2021, 7, 38–40. [Google Scholar] [CrossRef]
- Lytras, T.; Kopsachilis, F.; Mouratidou, E.; Papamichail, D.; Bonovas, S. Interventions to Increase Seasonal Influenza Vaccine Coverage in Healthcare Workers: A Systematic Review and Meta-Regression Analysis. Hum. Vaccin. Immunother. 2016, 12, 671–681. [Google Scholar] [CrossRef]
- Gomarverdi, S.; Khatiban, M.; Bikmoradi, A.; Soltanian, A.R. Effects of a Multi-Component Educational Intervention on Nurses’ Knowledge and Adherence to Standard Precautions in Intensive Care Units. J. Infect. Prev. 2019, 20, 83–90. [Google Scholar] [CrossRef]
- Drimili, E.; Herrero-Martin, R.; Suardiaz-Muro, J.; Zervas, E. Public Views and Attitudes about Municipal Waste Management: Empirical Evidence from Athens, Greece. Waste Manag. Res. 2020, 38, 614–625. [Google Scholar] [CrossRef]
- Swami, V.; Chamorro-Premuzic, T.; Snelgar, R.; Furnham, A. Personality, Individual Differences, and Demographic Antecedents of Self-Reported Household Waste Management Behaviours. J. Environ. Psychol. 2011, 31, 21–26. [Google Scholar] [CrossRef]
- Vassanadumrongdee, S.; Kittipongvises, S. Factors Influencing Source Separation Intention and Willingness to Pay for Improving Waste Management in Bangkok, Thailand. Sustain. Environ. Res. 2018, 28, 90–99. [Google Scholar] [CrossRef]
- Gupta, P.; Sharma, A.; Bhardwaj, L. Solid Waste Management (SWM) and Its Effect on Environment & Human Health. Preprints 2023, 2023090384. [Google Scholar] [CrossRef]
- Albarracin, D.; Shavitt, S. Attitudes and Attitude Change. Annu. Rev. Psychol. 2018, 69, 299–327. [Google Scholar] [CrossRef]
- Steinmetz, H.; Knappstein, M.; Ajzen, I.; Schmidt, P.; Kabst, R. How Effective Are Behavior Change Interventions Based on the Theory of Planned Behavior? A Three-Level Meta-Analysis. Z. Für Psychol. 2016, 224, 216–233. [Google Scholar] [CrossRef]
- Kheirabadi, S.; Sheikhi, A. Recent Advances and Challenges in Recycling and Reusing Biomedical Materials. Curr. Opin. Green Sustain. Chem. 2022, 38, 100695. [Google Scholar] [CrossRef]
- Janik-Karpinska, E.; Brancaleoni, R.; Niemcewicz, M.; Wojtas, W.; Foco, M.; Podogrocki, M.; Bijak, M. Healthcare Waste—A Serious Problem for Global Health. Healthcare 2023, 11, 242. [Google Scholar] [CrossRef]
- Tudor, T.L.; Barr, S.W.; Gilg, A.W. Strategies for Improving Recycling Behaviour within the Cornwall National Health Service (NHS) in the UK. Waste Manag. Res. 2007, 25, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Lally, P.; van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How Are Habits Formed: Modelling Habit Formation in the Real World. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef]
- Mannocci, A.; di Bella, O.; Barbato, D.; Castellani, F.; La Torre, G.; De Giusti, M.; Cimmuto, A.D. Assessing Knowledge, Attitude, and Practice of Healthcare Personnel Regarding Biomedical Waste Management: A Systematic Review of Available Tools. Waste Manag. Res. 2020, 38, 717–725. [Google Scholar] [CrossRef]
- Iyamu, H.O.; Anda, M.; Ho, G. A Review of Municipal Solid Waste Management in the BRIC and High-Income Countries: A Thematic Framework for Low-Income Countries. Habitat Int. 2020, 95, 102097. [Google Scholar] [CrossRef]
- Ferronato, N.; Torretta, V. Waste Mismanagement in Developing Countries: A Review of Global Issues. Int. J. Environ. Res. Public Health 2019, 16, 1060. [Google Scholar] [CrossRef]
- Mukhtar, S.; Khan, H.; Kian, Z.; Nawaz, S.; Zulfiqar, S.; Tabassum, N. Hospital Waste Management: Execution In Pakistan and Environmental Concerns—A Review. Environ. Contam. Rev. (ECR) 2018, 1, 18–23. [Google Scholar] [CrossRef]
- Datta, P.; Mohi, G.K.; Chander, J. Biomedical Waste Management in India: Critical Appraisal. J. Lab. Physicians 2018, 10, 6–14. [Google Scholar] [CrossRef]
- Garlasco, J.; Canepari, A.; Giacobone, G.; Funicelli, G.; Kozel, D.; Bernini, L.; Cotroneo, A. Impact of COVID-19 on Healthcare Waste Generation: Correlations and Trends from a Tertiary Hospital of a Developed Country. Waste Manag. Res. 2022, 40, 1450–1457. [Google Scholar] [CrossRef]
- Capoor, M.R.; Parida, A. Biomedical Waste and Solid Waste Management in the Time of COVID-19: A Comprehensive Review of the National and International Scenario and Guidelines. J. Lab. Physicians 2021, 13, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Al-Omran, K.; Khan, E.; Perna, S.; Ali, N. Factors Associated with Medical Waste under Pandemic Situation: A Case Study of the Kingdom of Bahrain. J. Mater. Cycles Waste Manag. 2023, 25, 2951–2963. [Google Scholar] [CrossRef]
- Singh, N.; Tang, Y.; Ogunseitan, O.A. Environmentally Sustainable Management of Used Personal Protective Equipment. Environ. Sci. Technol. 2020, 54, 8500–8502. [Google Scholar] [CrossRef] [PubMed]
- Al-Omran, K.; Abahussain, A.; Khan, E. Integrated Environmental Assessment of Medical Waste Management in the Kingdom of Bahrain. Sustainability 2023, 15, 2397. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) (Country, Year) Quality | Study Design | Setting (s) | Participants (n) | Intervention (Duration/Time of Assessment) | Assessment Tool or Method (Self-Reported/Observed) | Main Results |
|---|---|---|---|---|---|---|
| Abdo et al. [40] (Kuwait, 2019) Moderate | Pre–post | Tertiary Hospital | Environmental workers (n = 102) | Multi-component (Lessons, training, and reminders) 3 days/3 months | Ad hoc KAP questionnaire Structured checklist (Self-reported and observed) | Improvement in all aspects of KAP regarding infectious and sharps wastes after intervention (p < 0.01) |
| Ahmed et al. [41] (India, 2018) Moderate | Pre–post | Tertiary Hospital | Healthcare workers (n = 100) | Mono-component (Lessons) 1 day/immediate | Ad hoc KAP questionnaire (Self-reported) | Significant improvement in waste management after intervention; BMW disposal improvement was particularly highly significant (p < 0.001) |
| Ara et al. [42] (Bangladesh, 2015) Weak | Pre–post | Community Hospital | Nurses (n = 96) | Multi-component (Lessons and training) Not reported | Ad hoc KAP questionnaire Structured checklist (Self-reported and observed) | Compliance to waste segregation improved significantly after intervention (p < 0.001) |
| Ara et al. [43] (Bangladesh, 2022) Weak | Pre–post | Tertiary Hospital (n = 4) Community Hospital (n = 3) Primary Hospital (n = 2) | Healthcare workers Environmental workers (not reported) | Multi-component (Lessons, training, and system change) 6 months/3 months | Structured checklist (Observed) | Significant improvement in waste segregation, use of PPE during waste transportation, compliance with standardized methods for collection, transportation, and disposal (p < 0.001) |
| El-Gilany et al. [44] (Egypt, 2017) Strong | Pre–post | Tertiary Hospital | Laboratory technicians (n = 20) | Mono-component (Lessons) 3 days/2 months | Ad hoc KAP questionnaire (Self-reported) | Significant improvements in knowledge (p = 0.01), attitudes (p = 0.013), and practices regarding waste management (p = 0.01) |
| Elnour et al. [45] (Sudan, 2015) Strong | Pre–post | Tertiary Hospital (n = 3) | Nurses Environmental workers (n = 100) | Mono-component (Lessons) (15 days/immediate and at 3 months) | Ad hoc KAP questionnaire (Self-reported) | Moderate improvement in knowledge of waste management in immediate post-test period and at three months Scarce improvement in waste management practices in immediate post-test period after intervention, and moderate improvement at three months |
| Fraifeld et al. [46]. (USA, 2021) Weak | Pre–post | Tertiary Hospital | Anesthesia staff (n = 172) | Multi-component (Lessons and system change) (15 min/6 weeks) | Previously used KAP questionnaire Weight of segregated waste (Self-reported and observed) | Significant increase in overall knowledge of waste management (p < 0.001), particularly in vial disposal, medication disposal, and sharps disposal (p < 0.05); significant decrease in overall weight of regulated healthcare waste (p < 0.001) |
| Hosny et al. [47] (Egypt, 2018) Moderate | Pre–post | Tertiary Hospital | Environmental workers (n = 365) | Mono-component (Lessons) (Not reported) | Ad hoc KAP questionnaire Structured checklist (Self-reported and observed) | Significant increase in knowledge was detected (p < 0.001), except for items related to necessity to segregate healthcare waste, color coding system, disposal of general waste, and disposal of infectious waste; significant increase in waste management practices (p < 0.001) |
| Jarvis et al. [48] (USA, 2009) Weak | Pre–post | Mixed (Hospitals and Primary Care) | Pharmacists (n = 158) | Mono-component (Lessons) (1 newsletter/3 months) | Ad hoc KAP questionnaire (Self-reported) | Significant improvement in perception of environmental problems connected to inappropriate medication disposal (p = 0.03) and methods of correct disposal (p < 0.01) |
| Johnson et al. [49] (El Salvador, 2013) Moderate | Pre–post | Tertiary Hospital | Healthcare workers Environmental workers (n = 86) | Mono-component (Lessons) (20 min/1 year) | Ad hoc KAP questionnaire Weight of infectious waste (Self-reported and observed) | Significant improvement in knowledge of waste management (p = 0.012) and significant reduction in infectious waste disposal (p < 0.001) |
| Joseph et al. [50] (India, 2015) Moderate | Pre–post | Tertiary Hospital | Healthcare workers (n = 90) | Mono-component (Audits) (2 months/3 years) | Structured questions (Self-reported and observed) | Improvement in segregation of cytotoxic drugs (p < 0.05), sharps, infectious plastic, and use of color bags for healthcare waste segregation |
| Krishnan et al. [51] (India, 2015) Moderate | Pre–post | Mixed (Hospitals and Primary Care) | Healthcare workers (n = 1083) | Multi-component (Lessons and training) (Not reported/immediate) | Ad hoc KAP questionnaire (Self-reported) | Significant improvement in knowledge of waste management for all participants (p < 0.001) |
| Kumar et al. [52] (Pakistan, 2015) Strong | Case-control | Tertiary Hospital | Healthcare workers Environmental workers (n = 138) | Multi-component (Lessons, training, and reminders) (3 months/3 months) | Modified WHO tool (Self-reported) | Significant improvement in knowledge, attitudes, and practices (p < 0.01) in both healthcare and environmental workers |
| Kumar et al. [53] (Pakistan, 2016a) Weak | Case-control | Tertiary Hospital | Healthcare workers Environmental workers (n = 127) | Multi-component (Lessons, training, and reminders) 3 months/ 3 and 18 months) | Modified WHO tool (Self-reported) | Significant differences in knowledge, attitudes, and practices after 18 months compared to baseline (p < 0.001); these were retained over time by both healthcare and environmental workers |
| Kumar et al. [54] (Pakistan, 2016b) Moderate | Case-control | Tertiary Hospital | Physicians Nurses and paramedics (n = 222) | Multi-component (Lessons, training, and reminders) (3 months/ 3 and 18 months) | Modified WHO tool (Self-reported) | Nurses and paramedics showed better knowledge and practices compared to physicians; they retained higher level of knowledge than physicians, who achieved and retained positive attitudes towards waste management after intervention |
| Ozder et al. [55] (Turkey, 2013) Moderate | Pre–post | Mixed (Hospitals and Primary Care) | Healthcare managers (n = 240) | Multi-component (Lessons and training) (3 days/not reported) | Ad hoc KAP questionnaire (Self-reported) | Significant differences were found among managers who received healthcare waste management training and those who had not (p < 0.01); knowledge of managers who received healthcare waste management training improved significantly after intervention (p < 0.001) |
| Robat et al. [56] (Iran, 2022) Strong | Case-control | Tertiary Hospital | Healthcare workers Environmental workers (n = 128) | Multi-component (Lessons and training) (2 months/3 months) | Ad hoc KAP questionnaire (Self-reported) | Significant changes were shown in knowledge, attitudes, self-efficacy, beliefs, and motivation (p < 0.001); specifically, behavioral intentions toward waste management improved (p = 0.001) |
| Rohilla et al. [57] (India, 2021) Moderate | Retrospective | Tertiary Hospital | Healthcare workers (n = 450) | Multi-component (Lessons and training) (3 h/immediate) | Modified WHO tool Structured checklist (Self-reported and observed) | Significant increase in cognitive domain score from pre-test to post-test periods (p < 0.05) Overall change in psychomotor domains for all healthcare workers involved in intervention (p < 0.05) |
| Sapkota et al. [58] (Nepal, 2014) Strong | Pre–post | Tertiary Hospital | Healthcare workers Environmental workers (n = 40) | Multi-component (Lessons, training, system change, and reminders) (Not reported/8 months) | Individualized Rapid assessment tool (Self-reported and observed) | Significant improvement from 26% pre-test to 86% post-test regarding waste management practices evaluation score |
| Shaheen et al. [59] (Pakistan, 2020) Moderate | Pre–post | Tertiary Hospital | Nurses (n = 64) | Multi-component (Lessons and training) (3 days/1 month) | Ad hoc KAP questionnaire Structured checklist (Self-reported and observed) | Significant improvement in knowledge (p = 0.001) after intervention; one month after training sessions, practices showed significant improvement (p < 0.001) |
| Singh et al. [60] (India, 2020) Weak | Pre–post | Tertiary Hospital | Nurses Laboratory technicians (n = 250) | Multi-component (Lessons and training) (1 day/immediate) | Ad hoc KAP questionnaire (Self-reported) | Significant improvement in knowledge about healthcare waste management and handling (p < 0.001) after intervention |
| Tabash et al. [61] (Palestine, 2016) Moderate | Pre–post | Tertiary Hospital (n = 5) | Healthcare workers Environmental workers (n = 530) | Multi-component (Lessons and training) (3 h/immediate and at 6 months) | Ad hoc KAP questionnaire (Self-reported) | Significant improvement in knowledge, attitudes, and practices of staff regarding pharmaceutical waste management (p < 0.001) |
| Tabrizi et al. [62] (Iran, 2019) Strong | Clinical audit cycle | Primary Care Community Health Centers (n = 87) | Healthcare workers Environmental workers (not reported) | Multi-component (Audits, system change, and reminders) (1 year/4 months) | Adherence of existing status with standards (Observed) | Adherence to healthcare waste management standards experienced 30% improvement after interventions; greatest improvements were for waste management, education, and separation and collection of healthcare waste, increasing from 28 to 30% |
| Wu et al. [63] (Taiwan, 2021) Moderate | Pre–post | Tertiary Hospital | Physicians Laboratory technicians (n = 96) | Mono-component (Technology) (1 day/immediate) | Accuracy rate and time to complete the scenario (Self-reported and observed) | Significant improvement in accuracy as well as shorter time to complete scenario among junior physicians and male trainees compared to junior laboratory technicians |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, A.; Viottini, E.; Comoretto, R.I.; Piovan, C.; Martin, B.; Albanesi, B.; Clari, M.; Dimonte, V.; Campagna, S. The Effectiveness of Educational Interventions in Improving Waste Management Knowledge, Attitudes, and Practices among Healthcare Workers: A Systematic Review and Meta-Analysis. Sustainability 2024, 16, 3513. https://doi.org/10.3390/su16093513
Conti A, Viottini E, Comoretto RI, Piovan C, Martin B, Albanesi B, Clari M, Dimonte V, Campagna S. The Effectiveness of Educational Interventions in Improving Waste Management Knowledge, Attitudes, and Practices among Healthcare Workers: A Systematic Review and Meta-Analysis. Sustainability. 2024; 16(9):3513. https://doi.org/10.3390/su16093513
Chicago/Turabian StyleConti, Alessio, Elena Viottini, Rosanna Irene Comoretto, Chiara Piovan, Barbara Martin, Beatrice Albanesi, Marco Clari, Valerio Dimonte, and Sara Campagna. 2024. "The Effectiveness of Educational Interventions in Improving Waste Management Knowledge, Attitudes, and Practices among Healthcare Workers: A Systematic Review and Meta-Analysis" Sustainability 16, no. 9: 3513. https://doi.org/10.3390/su16093513