Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects—Impact on Glycaemia

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Interventions
2.3. Randomisation and Blinding
2.4. Measurement of Gastric Emptying
2.5. Measurements of Blood Glucose and Plasma Insulin
2.6. Statistical Analysis
3. Results
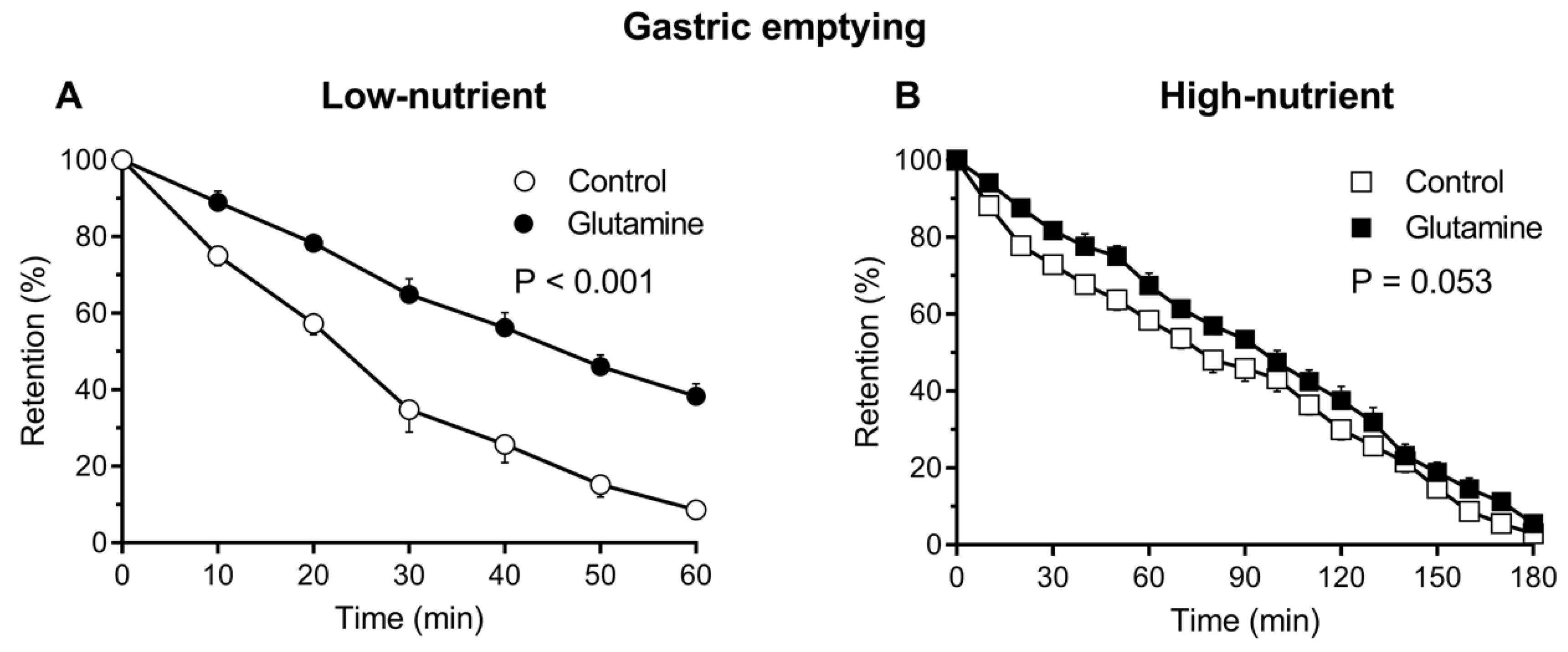
3.1. Gastric Emptying
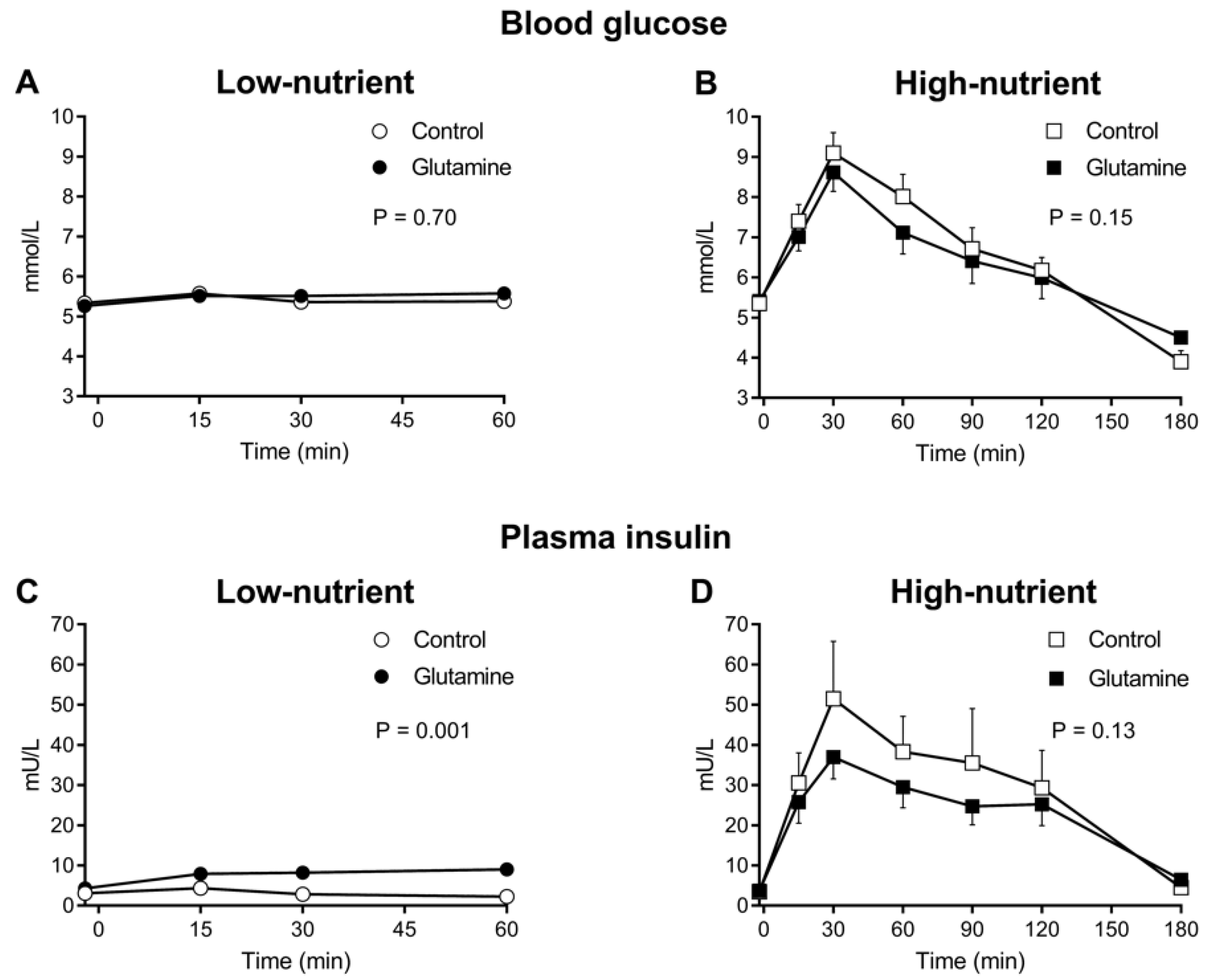
3.2. Blood Glucose
3.3. Plasma Insulin
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Monnier, L.; Lapinski, H.; Colette, C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: Variations with increasing levels of HbA(1c). Diabetes Care 2003, 26, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Ratner, R.E. Controlling postprandial hyperglycemia. Am. J. Cardiol. 2001, 88, 26H–31H. [Google Scholar] [CrossRef]
- Borch-Johnsen, K.; Neil, A.; Balkau, B.; Larsen, S.; Nissinen, A.; Pekkanen, J.; Tuomilehto, J.; Jousilahti, P.; Lindstrom, J.; Pyorala, M.; et al. Glucose tolerance and cardiovascular mortality: Comparison of fasting and 2-hour diagnostic criteria. Arch. Intern. Med. 2001, 161, 397–405. [Google Scholar]
- Horowitz, M.; Dent, J. Disordered gastric emptying: Mechanical basis, assessment and treatment. Baillieres Clin. Gastroenterol. 1991, 5, 371–407. [Google Scholar] [CrossRef]
- Horowitz, M.; Edelbroek, M.A.; Wishart, J.M.; Straathof, J.W. Relationship between oral glucose tolerance and gastric emptying in normal healthy subjects. Diabetologia 1993, 36, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.L.; Horowitz, M.; Carney, B.I.; Wishart, J.M.; Guha, S.; Green, L. Gastric emptying in early noninsulin-dependent diabetes mellitus. J. Nucl. Med. 1996, 37, 1643–1648. [Google Scholar] [PubMed]
- Vuksan, V.; Rogovik, A.L.; Jovanovski, E.; Jenkins, A.L. Fiber facts: Benefits and recommendations for individuals with type 2 diabetes. Curr. Diabetes Rep. 2009, 9, 405–411. [Google Scholar] [CrossRef]
- Gentilcore, D.; Chaikomin, R.; Jones, K.L.; Russo, A.; Feinle-Bisset, C.; Wishart, J.M.; Rayner, C.K.; Horowitz, M. Effects of fat on gastric emptying of and the glycemic, insulin, and incretin responses to a carbohydrate meal in type 2 diabetes. J. Clin. Endocrinol. Metab. 2006, 91, 2062–2067. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.K. Type 2 diabetes: Where we are today: An overview of disease burden, current treatments, and treatment strategies. J. Am. Pharm. Assoc. 2009, 49 (Suppl. 1), S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Kolterman, O.G.; Buse, J.B.; Fineman, M.S.; Gaines, E.; Heintz, S.; Bicsak, T.A.; Taylor, K.; Kim, D.; Aisporna, M.; Wang, Y.; et al. Synthetic exendin-4 (exenatide) significantly reduces postprandial and fasting plasma glucose in subjects with type 2 diabetes. J. Clin. Endocrinol. Metab. 2003, 88, 3082–3089. [Google Scholar] [CrossRef] [PubMed]
- Vella, A.; Lee, J.S.; Camilleri, M.; Szarka, L.A.; Burton, D.D.; Zinsmeister, A.R.; Rizza, R.A.; Klein, P.D. Effects of pramlintide, an amylin analogue, on gastric emptying in type 1 and 2 diabetes mellitus. Neurogastroenterol. Motil. 2002, 14, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Galera, S.C.; Fechine, F.V.; Teixeira, M.J.; Coelho, Z.C.; de Vasconcelos, R.C.; de Vasconcelos, P.R. The safety of oral use of l-glutamine in middle-aged and elderly individuals. Nutrition 2010, 26, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Menge, B.A.; Schrader, H.; Ritter, P.R.; Ellrichmann, M.; Uhl, W.; Schmidt, W.E.; Meier, J.J. Selective amino acid deficiency in patients with impaired glucose tolerance and type 2 diabetes. Regul. Pept. 2010, 160, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Samocha-Bonet, D.; Wong, O.; Synnott, E.L.; Piyaratna, N.; Douglas, A.; Gribble, F.M.; Holst, J.J.; Chisholm, D.J.; Greenfield, J.R. Glutamine reduces postprandial glycemia and augments the glucagon-like peptide-1 response in type 2 diabetes patients. J. Nutr. 2011, 141, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Samocha-Bonet, D.; Chisholm, D.J.; Gribble, F.M.; Coster, A.C.; Carpenter, K.H.; Jones, G.R.; Holst, J.J.; Greenfield, J.R. Glycemic effects and safety of L-Glutamine supplementation with or without sitagliptin in type 2 diabetes patients—A randomized study. PLoS ONE 2014, 9, e113366. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, J.R.; Farooqi, I.S.; Keogh, J.M.; Henning, E.; Habib, A.M.; Blackwood, A.; Reimann, F.; Holst, J.J.; Gribble, F.M. Oral glutamine increases circulating glucagon-like peptide 1, glucagon, and insulin concentrations in lean, obese, and type 2 diabetic subjects. Am. J. Clin. Nutr. 2009, 89, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; Picton, S.; Reid, U.; Thomas, D.; Gardener, C.; Smith, M.; Henderson, M.; Holden, V.; Kinsey, S.; Lewis, I.; et al. Oral glutamine in paediatric oncology patients: A dose finding study. Eur. J. Clin. Nutr. 2003, 57, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Reimann, F.; Williams, L.; da Silva Xavier, G.; Rutter, G.A.; Gribble, F.M. Glutamine potently stimulates glucagon-like peptide-1 secretion from glutag cells. Diabetologia 2004, 47, 1592–1601. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. The biology of incretin hormones. Cell Metab. 2006, 3, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Holst, J.J. The physiology of glucagon-like peptide 1. Physiol. Rev. 2007, 87, 1409–1439. [Google Scholar] [CrossRef] [PubMed]
- Deane, A.M.; Nguyen, N.Q.; Stevens, J.E.; Fraser, R.J.; Holloway, R.H.; Besanko, L.K.; Burgstad, C.; Jones, K.L.; Chapman, M.J.; Rayner, C.K.; et al. Endogenous glucagon-like peptide-1 slows gastric emptying in healthy subjects, attenuating postprandial glycemia. J. Clin. Endocrinol. Metab. 2010, 95, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Batterham, R.L.; Cowley, M.A.; Small, C.J.; Herzog, H.; Cohen, M.A.; Dakin, C.L.; Wren, A.M.; Brynes, A.E.; Low, M.J.; Ghatei, M.A.; et al. Gut hormone pyy(3-36) physiologically inhibits food intake. Nature 2002, 418, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Wynne, K.; Bloom, S.R. The role of oxyntomodulin and peptide tyrosine-tyrosine (PYY) in appetite control. Nat. Clin. Pract. Endocrinol. Metab. 2006, 2, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Wallis, K.; Walters, J.R.; Forbes, A. Review article: Glucagon-like peptide 2—Current applications and future directions. Aliment. Pharmacol. Ther. 2007, 25, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.N.; Hendry, P.O.; Rodrigues, G.; Marciani, L.; Totman, J.J.; Wright, J.W.; Preston, T.; Gowland, P.; Spiller, R.C.; Fearon, K.C. Gastric emptying of three liquid oral preoperative metabolic preconditioning regimens measured by magnetic resonance imaging in healthy adult volunteers: A randomised double-blind, crossover study. Clin. Nutr. 2009, 28, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Blackshaw, P.E.; Wright, J.W.; Macdonald, I.A.; Perkins, A.C.; Lobo, D.N. A randomized crossover study of the effects of glutamine and lipid on the gastric emptying time of a preoperative carbohydrate drink. Clin. Nutr. 2011, 30, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Wu, T.; Greenfield, J.R.; Samocha-Bonet, D.; Horowitz, M.; Rayner, C.K. Effects of intraduodenal glutamine on incretin hormone and insulin release, the glycemic response to an intraduodenal glucose infusion, and antropyloroduodenal motility in health and type 2 diabetes. Diabetes Care 2013, 36, 2262–2265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horowitz, M.; O’Donovan, D.; Jones, K.L.; Feinle, C.; Rayner, C.K.; Samsom, M. Gastric emptying in diabetes: Clinical significance and treatment. Diabet. Med. 2002, 19, 177–194. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Dent, J.; Fraser, R.; Sun, W.; Hebbard, G. Role and integration of mechanisms controlling gastric emptying. Dig. Dis. Sci. 1994, 39, 7S–13S. [Google Scholar] [CrossRef] [PubMed]
- Marathe, C.S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. Relationships between gastric emptying, postprandial glycemia, and incretin hormones. Diabetes Care 2013, 36, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- Hveem, K.; Jones, K.L.; Chatterton, B.E.; Horowitz, M. Scintigraphic measurement of gastric emptying and ultrasonographic assessment of antral area: Relation to appetite. Gut 1996, 38, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore, D.; Hausken, T.; Horowitz, M.; Jones, K.L. Measurements of gastric emptying of low- and high-nutrient liquids using 3d ultrasonography and scintigraphy in healthy subjects. Neurogastroenterol. Motil. 2006, 18, 1062–1068. [Google Scholar] [CrossRef] [PubMed]
- RANDOM.ORG. Available online: http://www.random.org/ (accessed on 30 March 2011).
- Jones, K.L.; O’Donovan, D.; Horowitz, M.; Russo, A.; Lei, Y.; Hausken, T. Effects of posture on gastric emptying, transpyloric flow, and hunger after a glucose drink in healthy humans. Dig. Dis. Sci. 2006, 51, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Mercodia Insulin ELISA. Version 4.0 ed.; Vol. Article No 32-4143. 2016. Available online: https://www.mercodia.com/assets/upload/files/Product%20sheets/10-1113-01_10%20Insulin%204_0.pdf (accessed on 4 April 2018).
- Marathe, C.S.; Rayner, C.K.; Lange, K.; Bound, M.; Wishart, J.; Jones, K.L.; Kahn, S.E.; Horowitz, M. Relationships of the early insulin secretory response and oral disposition index with gastric emptying in subjects with normal glucose tolerance. Physiol. Rep. 2017, 5, e13122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, J.M.; Spector, A.C.; Grill, H.J. Dynamics of gastric emptying during and after stomach fill. Am. J. Physiol. 1992, 263, R813–R819. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Doty, J.E.; Reedy, T.J.; Meyer, J.H. Inhibition of gastric emptying by glucose depends on length of intestine exposed to nutrient. Am. J. Physiol. 1989, 256, G404–G411. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Cunningham, K.M.; Wishart, J.M.; Jones, K.L.; Read, N.W. The effect of short-term dietary supplementation with glucose on gastric emptying of glucose and fructose and oral glucose tolerance in normal subjects. Diabetologia 1996, 39, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Brener, W.; Hendrix, T.R.; McHugh, P.R. Regulation of the gastric emptying of glucose. Gastroenterology 1983, 85, 76–82. [Google Scholar] [PubMed]
- Grau, T.; Bonet, A.; Minambres, E.; Pineiro, L.; Irles, J.A.; Robles, A.; Acosta, J.; Herrero, I.; Palacios, V.; Lopez, J.; et al. The effect of L-alanyl-L-glutamine dipeptide supplemented total parenteral nutrition on infectious morbidity and insulin sensitivity in critically ill patients. Crit. Care Med. 2011, 39, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Niedereichholz, U.; Ettler, R.; Holst, J.J.; Orskov, C.; Ritzel, R.; Schmiegel, W.H. Glucagon-like peptide 1 inhibition of gastric emptying outweighs its insulinotropic effects in healthy humans. Am. J. Physiol. 1997, 273, E981–E988. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A. Is glucagon-like peptide 1 an incretin hormone? Diabetologia 1999, 42, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, J.J.; Kemmeries, G.; Holst, J.J.; Nauck, M.A. Erythromycin antagonizes the deceleration of gastric emptying by glucagon-like peptide 1 and unmasks its insulinotropic effect in healthy subjects. Diabetes 2005, 54, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Iwashita, S.; Mikus, C.; Baier, S.; Flakoll, P.J. Glutamine supplementation increases postprandial energy expenditure and fat oxidation in humans. J. Parenter. Enter. Nutr. 2006, 30, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Borel, M.J.; Williams, P.E.; Jabbour, K.; Levenhagen, D.; Kaizer, E.; Flakoll, P.J. Parenteral glutamine infusion alters insulin-mediated glucose metabolism. J. Parenter. Enter. Nutr. 1998, 22, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, B.H. Factors affecting blood glucose monitoring: Sources of errors in measurement. J. Diabetes Sci. Technol. 2009, 3, 903–913. [Google Scholar] [CrossRef] [PubMed]
- De Schepper, H.U.; Cremonini, F.; Chitkara, D.; Camilleri, M. Assessment of gastric accommodation: Overview and evaluation of current methods. Neurogastroenterol. Motil. 2004, 16, 275–285. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Low-Nutrient Soup | Low-Nutrient Soup with Glutamine | High-Nutrient Glucose | High-Nutrient Glucose with Glutamine | |
|---|---|---|---|---|
| Volume (mL) | 300 | 300 | 300 | 300 |
| Calories (kCal) | 18 | 138 | 255 | 375 |
| Carbohydrate (g) | 2.2 | 2.2 | 75 | 75 |
| Fat (g) | 0.8 | 0.8 | 0 | 0 |
| Protein (g) | 0.4 | 0.4 | 0 | 0 |
| Glutamine (g) | 0 | 30 | 0 | 30 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, Y.T.; Piscitelli, D.; Ahmad, S.; Trahair, L.G.; Greenfield, J.R.; Samocha-Bonet, D.; Rayner, C.K.; Horowitz, M.; Jones, K.L. Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects—Impact on Glycaemia. Nutrients 2018, 10, 739. https://doi.org/10.3390/nu10060739
Du YT, Piscitelli D, Ahmad S, Trahair LG, Greenfield JR, Samocha-Bonet D, Rayner CK, Horowitz M, Jones KL. Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects—Impact on Glycaemia. Nutrients. 2018; 10(6):739. https://doi.org/10.3390/nu10060739
Chicago/Turabian StyleDu, Yang T., Diana Piscitelli, Saima Ahmad, Laurence G. Trahair, Jerry R. Greenfield, Dorit Samocha-Bonet, Christopher K. Rayner, Michael Horowitz, and Karen L. Jones. 2018. "Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects—Impact on Glycaemia" Nutrients 10, no. 6: 739. https://doi.org/10.3390/nu10060739