A Pilot Randomized Trial of Oral Magnesium Supplementation on Supraventricular Arrhythmias

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Intervention and Blinding
2.3. Measurements
2.4. Statistical Analysis
3. Results
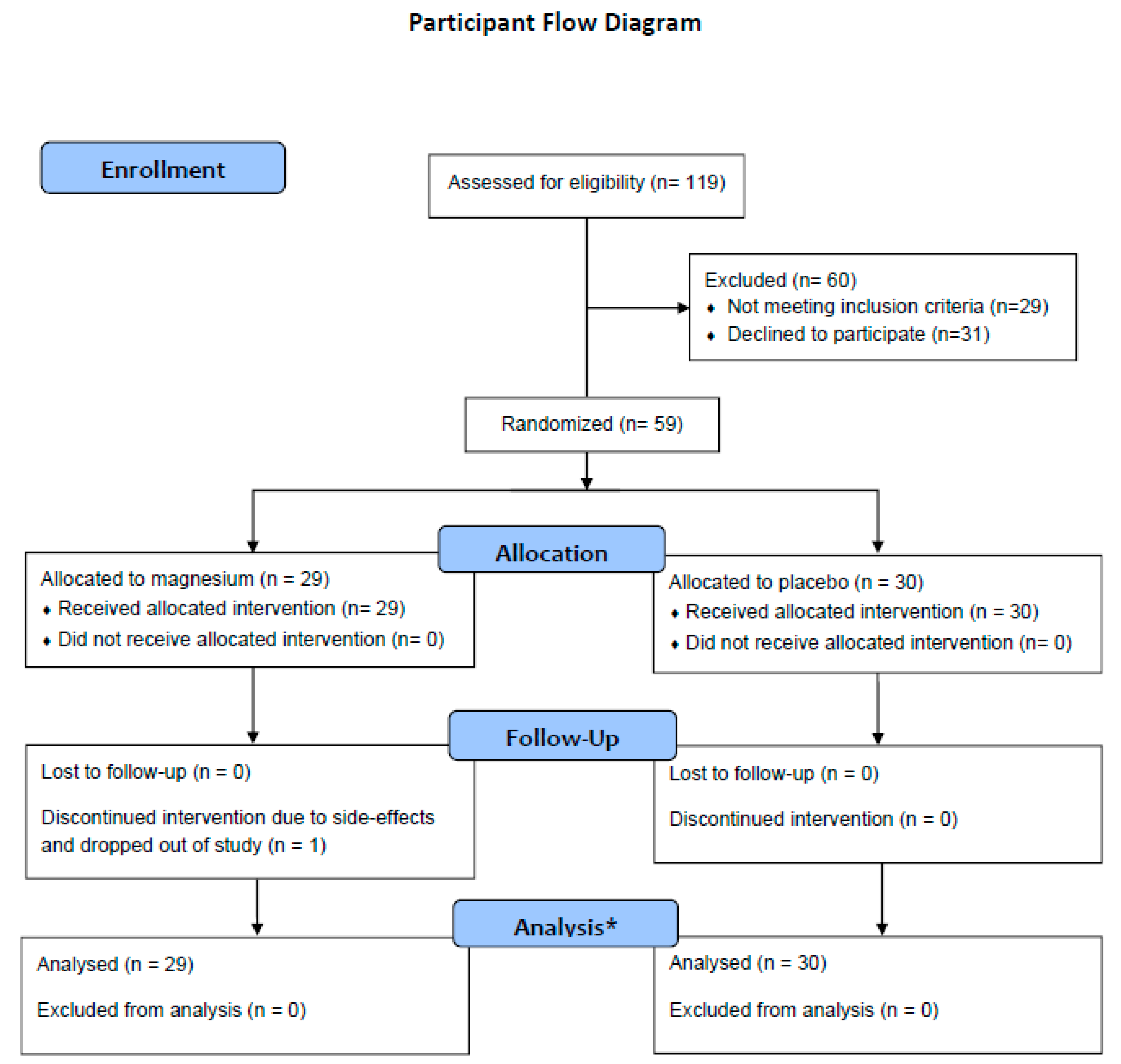
3.1. Study Participants
3.2. Follow-Up
3.3. Adherence and Magnesium Concentrations
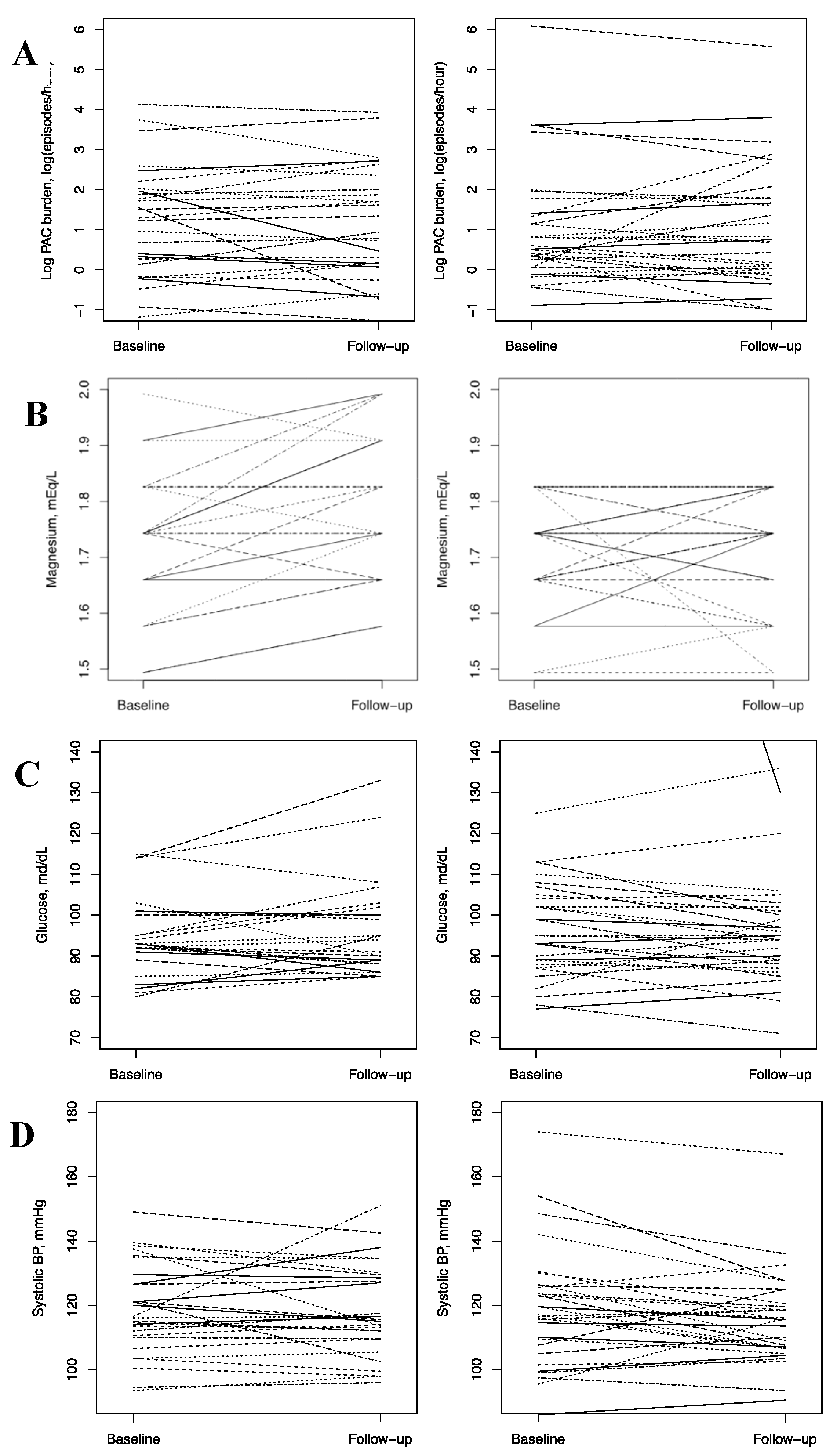
3.4. Effect of Magnesium Supplementation on Trial Outcomes
3.5. Safety and Tolerability of the Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.C.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults. National implications for rhythm management and stroke prevention: The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Miyasaka, Y.; Barnes, M.E.; Gersh, B.J.; Cha, S.S.; Bailey, K.R.; Abhayaratna, W.P.; Seward, J.B.; Tsang, T.S.M. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006, 114, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; de Ferranti, S.D.; et al. Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation 2018. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 2014, 130, e199–e267. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Chen, P.-S.; Bild, D.E.; Mascette, A.M.; Albert, C.M.; Alonso, A.; Calkins, H.; Connolly, S.J.; Curtis, A.B.; Darbar, D.; et al. Prevention of atrial fibrillation: Report from an NHLBI workshop. Circulation 2009, 119, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Van Wagoner, D.R.; Piccini, J.P.; Albert, C.M.; Anderson, M.E.; Benjamin, E.J.; Brundel, B.; Califf, R.M.; Calkins, H.; Chen, P.-S.; Chiamvimonvat, N.; et al. Progress toward the prevention and treatment of atrial fibrillation: A summary of the Heart Rhythm Society Research Forum on the Treatment and Prevention of Atrial Fibrillation, Washington, DC, December 9–10, 2013. Heart Rhythm 2015, 12, e5–e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arsenault, K.A.; Yusuf, A.M.; Crystal, E.; Healey, J.S.; Morillo, C.A.; Nair, G.M.; Whitlock, R.P. Interventions for preventing post-operative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Syst. Rev. 2013, 1, CD003611. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.M.; Lubitz, S.A.; Sullivan, L.M.; Sun, J.X.; Levy, D.; Vasan, R.S.; Magnani, J.W.; Ellinor, P.T.; Benjamin, E.J.; Wang, T.J. Low serum magnesium and the development of atrial fibrillation in the community: The Framingham Heart Study. Circulation 2013, 127, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Misialek, J.R.; Lopez, F.L.; Lutsey, P.L.; Huxley, R.R.; Peacock, J.M.; Chen, L.Y.; Soliman, E.Z.; Agarwal, S.K.; Alonso, A. Serum and dietary magnesium and incidence of atrial fibrillation in whites and in African Americans—Atherosclerosis Risk in Communities (ARIC) Study. Circ. J. 2013, 77, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Markovits, N.; Kurnik, D.; Halkin, H.; Margalit, R.; Bialik, M.; Lomnicky, Y.; Loebstein, R. Database evaluation of the association between serum magnesium levels and the risk of atrial fibrillation in the community. Int. J. Cardiol. 2016, 205, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H.; Milne, D.B.; Klevay, L.M.; Gallagher, S.; Johnson, L. Dietary magnesium deficiency induces heart rhythm changes, impairs glucose tolerance, and decreases serum cholesterol in post menopausal women. J. Am. Coll. Nutr. 2007, 26, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, G.M.; Byrd-Bredbenner, C.; Moe, G.; Berning, J.R.; Kelley, D.S. Wardlaw’s Perspectives in Nutrition, 10th ed.; McGraw-Hill Education: New York, NY, USA, 2016. [Google Scholar]
- Worwag, M.; Classen, H.G.; Schumacher, E. Prevalence of magnesium and zinc deficiencies in nursing home residents in Germany. Magn. Res. 1999, 12, 181–189. [Google Scholar]
- Dietary Guidelines for Americans 2015–2020. Available online: https://health.gov/dietaryguidelines/2015/resources/2015-2020_Dietary_Guidelines.pdf (accessed on 2 October 2017).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; Marcus, G.M. Atrial Ectopy as a Predictor of Incident Atrial Fibrillation A Cohort Study. Ann. Intern. Med. 2013, 159, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Chong, B.H.; Pong, V.; Lam, K.F.; Liu, S.; Zuo, M.L.; Lau, Y.F.; Lau, C.P.; Tse, H.F.; Siu, C.W. Frequent premature atrial complexes predict new occurrence of atrial fibrillation and adverse cardiovascular events. Europace 2012, 14, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Conen, D.; Adam, M.; Roche, F.; Barthelemy, J.C.; Felber Dietrich, D.; Imboden, M.; Kunzli, N.; von Eckardstein, A.; Regenass, S.; Hornemann, T.; et al. Premature atrial contractions in the general population: Frequency and risk factors. Circulation 2012, 126, 2302–2308. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Hoang, D.D.; Zimetbaum, P.; Miller, J.D.; Froelicher, V.F.; Kumar, U.N.; Xu, X.; Yang, F.; Heidenreich, P.A. Diagnostic utility of a novel leadless arrhythmia monitoring device. Am. J. Cardiol. 2013, 112, 520–524. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Byrd-Bredbenner, C.; Moe, G.; Beshgetoor, D.; Berning, J. Wardlaw’s Perspectives in Nutrition, 9th ed.; McGraw-Hill: New York, NY, USA, 2013; 259p. [Google Scholar]
- Christiansen, E.H.; Frost, L.; Andreasen, F.; Mortensen, P.; Thomsen, P.E.; Pedersen, A.K. Dose-related cardiac electrophysiological effects of intravenous magnesium. A double-blind placebo-controlled dose-response study in patients with paroxysmal supraventricular tachycardia. Europace 2000, 2, 320–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, H.S.; Thomsen, P.E. The electrophysiological effects of intravenous magnesium on human sinus node, atrioventricular node, atrium, and ventricle. Clin. Cardiol. 1989, 12, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulick, D.L.; Hong, R.; Ryzen, E.; Rude, R.K.; Rubin, J.N.; Elkayam, U.; Rahimtoola, S.H.; Bhandari, A.K. Electrophysiologic effects of intravenous magnesium in patients with normal conduction systems and no clinical evidence of significant cardiac disease. Am. Heart J. 1988, 115, 367–373. [Google Scholar] [CrossRef]
- Zehender, M.; Meinertz, T.; Faber, T.; Caspary, A.; Jeron, A.; Bremm, K.; Just, H. Antiarrhythmic Effects of Increasing the Daily Intake of Magnesium and Potassium in Patients With Frequent Ventricular Arrhythmias fn1fn1This study was supported by Trommsdorff GmbH and Company, Alsdorf, Germany and Hexal AG, Holzkirchen, Germany. J. Am. Coll. Cardiol. 1997, 29, 1028–1034. [Google Scholar] [CrossRef]
- Huxley, R.R.; Filion, K.B.; Konety, S.; Alonso, A. Meta-analysis of cohort and case-control studies of type 2 diabetes mellitus and risk of atrial fibrillation. Am. J. Cardiol. 2011, 108, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Roetker, N.S.; Chen, L.Y.; Heckbert, S.R.; Nazarian, S.; Soliman, E.Z.; Bluemke, D.A.; Lima, J.A.; Alonso, A. Relation of systolic, diastolic, and pulse pressure and aortic distensibility with atrial fibrillation (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2014, 114, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Jee, S.H.; Miller, E.R., 3rd; Guallar, E.; Singh, V.K.; Appel, L.J.; Klag, M.J. The effect of magnesium supplementation on blood pressure: A meta-analysis of randomized clinical trials. Am. J. Hypertens. 2002, 15, 691–696. [Google Scholar] [CrossRef]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, Y.; Del Gobbo, L.C.; Rosanoff, A.; Wang, J.; Zhang, W.; Song, Y. Effects of Magnesium Supplementation on Blood Pressure: A Meta-Analysis of Randomized Double-Blind Placebo-Controlled Trials. Hypertension 2016, 68, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; He, K.; Levitan, E.B.; Manson, J.E.; Liu, S. Effects of oral magnesium supplementation on glycaemic control in type 2 diabetes: A meta-analysis of randomized double-blind controlled trials. Diabet. Med. 2006, 23, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Del Gobbo, L.C.; Hruby, A.; Rosanoff, A.; He, K.; Dai, Q.; Costello, R.B.; Zhang, W.; Song, Y. The circulating concentration and 24-h urine excretion of magnesium dose- and time-dependently respond to oral magnesium supplementation in a meta-analysis of randomized controlled trials. J. Nutr. 2016, 146, 595–602. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | Magnesium (400 mg Daily) | Placebo | p-Value | |
|---|---|---|---|---|
| N | 59 | 29 | 30 | |
| Demographics | ||||
| Age, years | 61.5 ± 5.2 | 61.3 ± 5.3 | 61.6 ± 5.2 | 0.814 |
| Age category | 0.761 | |||
| ≥65 years | 14 (23.7) | 6 (20.7) | 8 (26.7) | |
| <65 years | 45 (76.3) | 23 (79.3) | 22 (73.3) | |
| Sex | 0.039 | |||
| Female | 43 (72.9) | 25 (86.2) | 18 (60.0) | |
| Male | 16 (27.1) | 4 (13.8) | 12 (40) | |
| Race | 0.612 | |||
| White | 56 (94.9) | 27 (93.1) | 29 (96.7) | |
| Nonwhite | 3 (5.1) | 2 (6.9) | 1 (3.3) | |
| Educational attainment | 0.279 | |||
| High school graduate or GED | 1 (1.7) | 0 (0) | 1 (3.3) | |
| Some college | 10 (16.9) | 6 (20.7) | 4 (13.3) | |
| College graduate | 26 (44.1) | 10 (34.5) | 16 (53.3) | |
| Graduate school or professional school | 22 (37.3) | 13 (44.8) | 9 (30) | |
| Physiologic characteristics | ||||
| Height, cm | 167.9 (9.2) | 167.1 (8.1) | 168.7 (10.3) | 0.491 |
| Weight, kg | 79.2 (18.2) | 78.0 (18.0) | 80.5 (18.7) | 0.603 |
| BMI, kg/m2 | 27.9 ± 4.6 | 27.7 ± 4.9 | 28.0 ± 4.5 | 0.804 |
| Serum magnesium, mEq/L | 1.72 ± 0.11 | 1.74 ± 0.12 | 1.71 ± 0.10 | 0.308 |
| Systolic blood pressure, mmHg | 119 ± 16 | 119 ± 14 | 119 ± 18 | 0.933 |
| Diastolic blood pressure, mmHg | 71 ± 9 | 72 ± 9 | 71 ± 10 | 0.627 |
| Antihypertensive medication | 14 (24) | 9 (31) | 5 (17) | 0.233 |
| Serum glucose, mg/dL | 98.9 ± 29.9 | 94.2 ± 10.6 | 103.2 ± 40.2 | 0.242 |
| Sensitivity analysis ** | 95.2 ± 11.1 | 94.2 ± 10.6 | 96.2 ± 11.6 | 0.494 |
| Glucose lowering medication | 2 (3.4) | 0 (0) | 2 (6.7) | 0.492 |
| PAC burden, episodes/h | 14.5 ± 58 | 8.5 ± 14 | 20.2 ± 80 | 0.437 |
| Median (25th, 75th percentiles) | 2.28 (1.22, 6.86) | 3.64 (1.31, 7.57) | 1.75 (1.12, 4.01) | |
| Log PAC burden, log(episodes/h) | 1.15 ± 1.42 | 1.26 ± 1.35 | 1.04 ± 1.49 | 0.566 |
| Median (25th, 75th percentiles) | 0.82 (0.20, 1.92) | 1.29 (0.27, 2.02) | 0.55 (0.11, 1.39) |
| Compliance | % Reporting Missing Pills | Reason for Missing Pills, N | |||||
| Forgot | Too Busy | Makes Me Sick | Other | ||||
| Ever reported * | |||||||
| Magnesium | 60% | 7 | 0 | 5 | 2 | ||
| Placebo | 52% | 11 | 2 | 0 | 3 | ||
| % Reporting Missing Pills in: | Reason for Missing Pills, N | ||||||
| Reported at Specific Follow-Up Visits ** | Last 3 Days | Last 1 Week | Last 2 Weeks | ||||
| Intervention Day 21 | |||||||
| Magnesium | 8% | 12% | 20% | 2 | 0 | 2 | 1 |
| Placebo | 0% | 7% | 24% | 7 | 1 | 0 | 0 |
| Intervention Day 42 | |||||||
| Magnesium | 22% | 33% | 39% | 5 | 0 | 5 | 1 |
| Placebo | 15% | 22% | 31% | 6 | 2 | 0 | 2 |
| Intervention Day 80 | |||||||
| Magnesium | 14% | 27% | 40% | 5 | 0 | 1 | 0 |
| Placebo | 12% | 23% | 28% | 6 | 1 | 0 | 1 |
| Magnesium (400 mg Daily) Mean (SD) | Placebo Mean (SD) | Intervention Effect Coefficient * (95% CI) | p-Value | |
|---|---|---|---|---|
| Primary outcome (episodes/h) | ||||
| Log PAC burden | 0.94 (0.69, 1.3) ** | 0.73 | ||
| Baseline | 1.26 (1.4) | 1.04 (1.49) | ||
| Follow-up † | 1.16 (1.41) | 1.09 (1.53) | ||
| Change | −0.06 (0.68) | 0.05 (0.75) | ||
| PAC burden | 0.44 (−2.58, 3.46) | |||
| Baseline | 8.5 ± 14 | 20.2 ± 80 | ||
| Follow-up † | 8.1 ± 12 | 14.6 ± 48 | ||
| Change | −0.6 ± 7 | −5.6 ± 33 | ||
| Secondary outcomes | ||||
| Serum magnesium, mEq/L | 0.07 (0.03, 0.12) | 0.002 | ||
| Baseline | 1.74 (0.12) | 1.71 (0.1) | ||
| Follow-up ‡ | 1.8 (0.13) | 1.71 (0.11) | ||
| Change | 0.07 (0.09) | 0 (0.1) | ||
| Serum glucose, mg/dL | ||||
| Baseline | 94.2 (10.6) | 103.2 (40.2) | 2.4 (−3.0, 7.7) | 0.39 |
| Follow-up ‡ | 96.3 (12.2) | 96.2 (13.7) | ||
| Change | 1.8 (7.5) | −7.1 (32.8) | ||
| Serum glucose ¥, mg/dL | ||||
| Baseline | 94.2 (10.6) | 96.2 (11.6) | 2.8 (−0.9, 6.4) | 0.14 |
| Follow-up ‡ | 96.3 (12.2) | 95 (12.4) | ||
| Change | 1.75 (7.5) | −1.21 (6.7) | ||
| Systolic blood pressure, mmHg | 2.9 (−1.8, 7.2) | 0.18 | ||
| Baseline | 119 (14) | 119 (18) | ||
| Follow-up ‡ | 118 (14) | 115 (14) | ||
| Change | −1 (10) | −4 (10) | ||
| Diastolic blood pressure, mmHg | −0.5 (−3.5, 2.5) | 0.74 | ||
| Baseline | 71.8 (8. 7) | 70.6 (10.3) | ||
| Follow-up ‡ | 71.0 (8.8) | 70.8 (8.7) | ||
| Change | −0.5 (7.1) | 0.2 (6.1) | ||
| Primary Outcome | Baseline Serum Magnesium Concentration | p-Interaction | |||
|---|---|---|---|---|---|
| <Median | ≥Median | ||||
| Intervention Effect Coefficient * (95% CI) | p-Value | Intervention Effect Coefficient * (95% CI) | p-Value | ||
| Log PAC burden | 0.89 (0.51, 1.54) ** | 0.67 | 0.91 (0.61, 1.35) ** | 0.64 | 0.88 |
| Serum magnesium, mEq/L | 0.05 (0, 0.10) | 0.04 | 0.12 (0.04,0.20) | 0.004 | 0.24 |
| Serum glucose, magnesium/dL | −4.7 (−13.3, 4.0) | 0.29 | 6.0 (2.0, 10.0) | 0.03 | 0.06 |
| Serum glucose, magnesium/dL ¥ | −3.2 (−9.0, 2.6) | 0.28 | 6.0 (2.0, 10.0) | 0.03 | 0.01 |
| Systolic blood pressure, mmHg | 4.8 (1.0, 8.5) | 0.01 | 3.8 (−2.5, 10.2) | 0.24 | 0.96 |
| Diastolic blood pressure, mmHg | 5.5 (0.6, 10.4) | 0.03 | 2.4 (−5.6, 0.8) | 0.14 | 0.009 |
| Intervention Day # | Intervention | Comment |
|---|---|---|
| Day #21 | Magnesium | Less solid stools |
| Magnesium | Initially, I took the pill before bed with calcium and fish oil and a blood pressure med. It did not really make me sick, but I felt some bloating and cramping. I switched to taking it in the am, and that works better. That was the reason for missing. | |
| Magnesium | Diarrhea | |
| Magnesium | My stools have changed in consistency and color. | |
| Magnesium | I have had some diarrhea but that could be due to my innards. They have been unpredictable since my abdominal/colorectal surgeries. | |
| Magnesium | After 4 pills, I quit taking them due to intestinal issues. I was in the bathroom the third and fourth day and very crampy all day. I emailed and was told I could quit taking them. | |
| Magnesium | The first two days, I experienced brief bouts of diarrhea about 90 min after taking the pills. No problems since. | |
| Magnesium | Some diarrhea and gas | |
| Placebo | Sudden onset of nausea lasting about 30 s about an hour after taking the pill. | |
| Placebo | Increase in diarrhea but could be from the increase in nuts in my diet. | |
| Day #42 | Magnesium | Slightly often stools |
| Magnesium | Diarrhea | |
| Magnesium | Slight nausea, slight pain in stomach, increased flatulence | |
| Magnesium | Upset Stomach | |
| Magnesium | The initial 4 pills made me sick. Also, I am currently stressed as my (spouse) is scheduled for (major) surgery next week. | |
| Magnesium | A little diarrhea an hour or so after taking the pill, but this only happened on the first two days. | |
| Magnesium | Had gastrointestional issues when taking the pill. | |
| Magnesium | Loose stools, some diarrhea, and cramps after taking pill in the morning. | |
| Placebo | Diarrhea, but could be due to increased nut intake, | |
| Day #80 | Magnesium | Some difficulty with digestion |
| Magnesium | My fingernails have gotten must stronger, and my bowels were loose and somewhat sluggish. | |
| Magnesium | I have been a lot ‘looser’ since taking the pills. | |
| Magnesium | Upset stomach | |
| Magnesium | Small bouts of diarrhea the first two days of taking the pills; nothing since. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lutsey, P.L.; Chen, L.Y.; Eaton, A.; Jaeb, M.; Rudser, K.D.; Neaton, J.D.; Alonso, A. A Pilot Randomized Trial of Oral Magnesium Supplementation on Supraventricular Arrhythmias. Nutrients 2018, 10, 884. https://doi.org/10.3390/nu10070884
Lutsey PL, Chen LY, Eaton A, Jaeb M, Rudser KD, Neaton JD, Alonso A. A Pilot Randomized Trial of Oral Magnesium Supplementation on Supraventricular Arrhythmias. Nutrients. 2018; 10(7):884. https://doi.org/10.3390/nu10070884
Chicago/Turabian StyleLutsey, Pamela L., Lin Y. Chen, Anne Eaton, Melanie Jaeb, Kyle D. Rudser, James D. Neaton, and Alvaro Alonso. 2018. "A Pilot Randomized Trial of Oral Magnesium Supplementation on Supraventricular Arrhythmias" Nutrients 10, no. 7: 884. https://doi.org/10.3390/nu10070884