SunGold Kiwifruit Supplementation of Individuals with Prediabetes Alters Gut Microbiota and Improves Vitamin C Status, Anthropometric and Clinical Markers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Study Design
2.3. Anthropometric Measures
2.3.1. Weight (kg)
2.3.2. Height (m)
2.3.3. BMI (kg/m2)
2.3.4. Waist Circumference (cm)
2.3.5. Hip Circumference (cm)
2.3.6. Waist-To-Hip Ratio
2.3.7. Fat Mass (%)
2.3.8. Blood Pressure (mmHg)
2.4. Blood Parameters
2.4.1. Glucose
2.4.2. Vitamin C
2.4.3. HbA1c
2.4.4. Lipid Parameters
2.4.5. hs-CRP
2.4.6. Hormones
2.5. Faecal Microbiota Analysis
2.5.1. DNA Extraction and Sequence Analysis
2.5.2. Faecal Water Content
2.6. Questionnaires
2.6.1. Demographic Information
2.6.2. Medication and Supplement Use
2.6.3. Dietary Intake
- percent energy from fat = (fat (g/day) × 37.7 kJ/g)/energy (kJ/day)
- percent energy from carbohydrate = (carbohydrate (g/day) × 16.7 kJ/g)/energy (kJ/day)
- percent energy from protein = (protein (g/day) × 16.7 kJ/g)/energy (kJ/day)
2.6.4. Physical Activity
2.7. Statistical Analysis
3. Results
3.1. Dietary Intakes: Macronutrients, Micronutrients, Fruit Intake
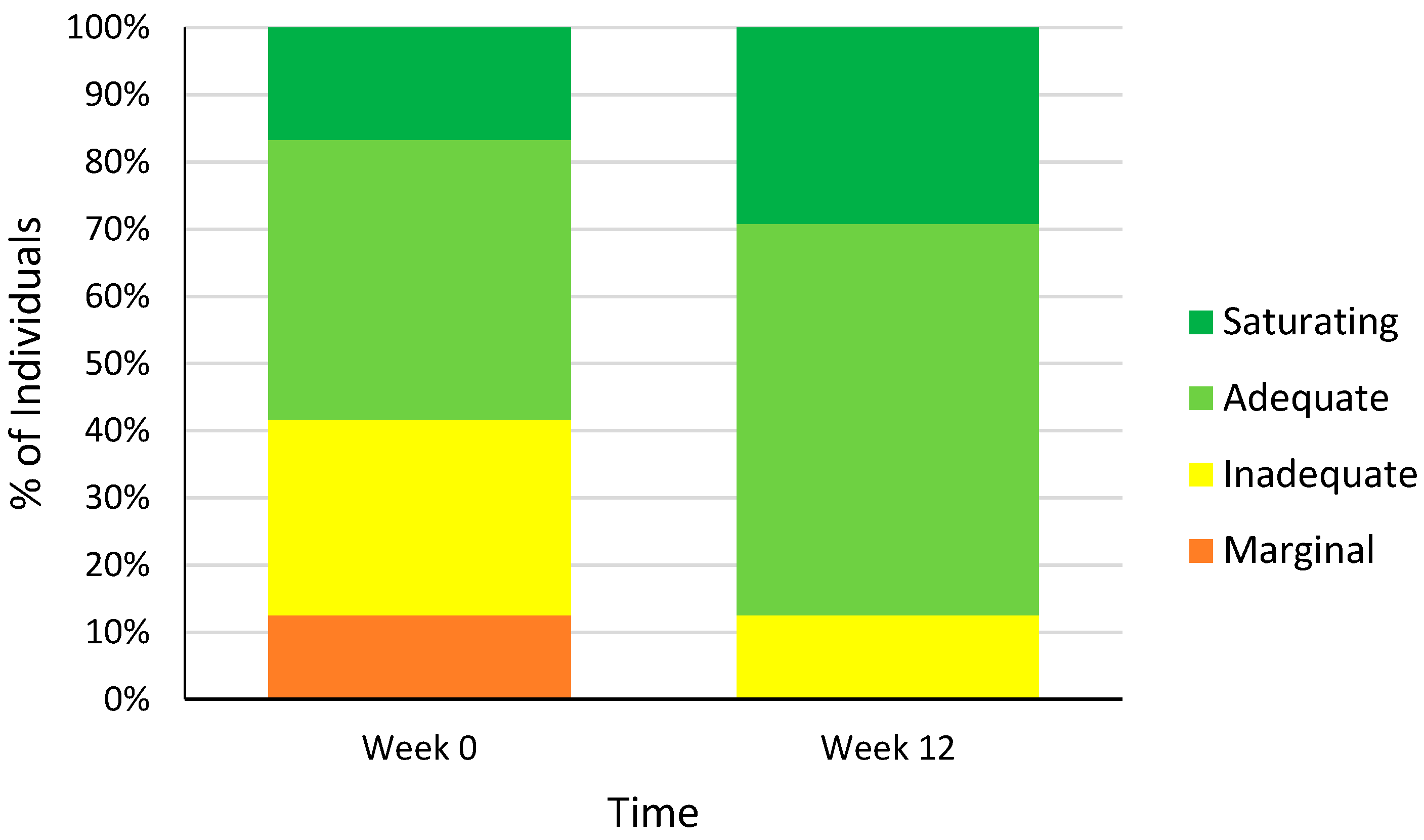
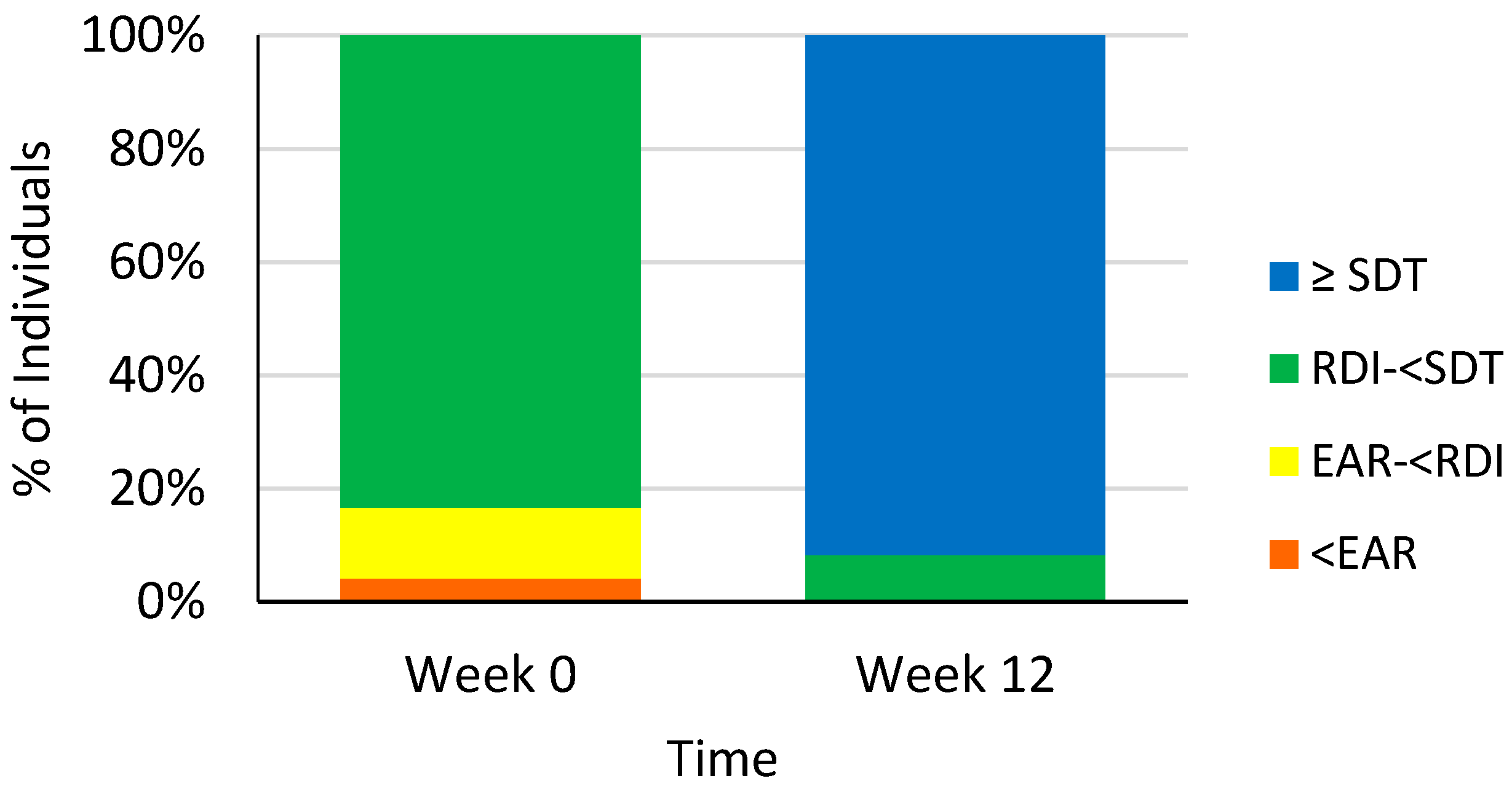
3.2. Dietary Vitamin C Intakes
3.3. Anthropometry and Blood Pressure
3.4. Biochemical Indices
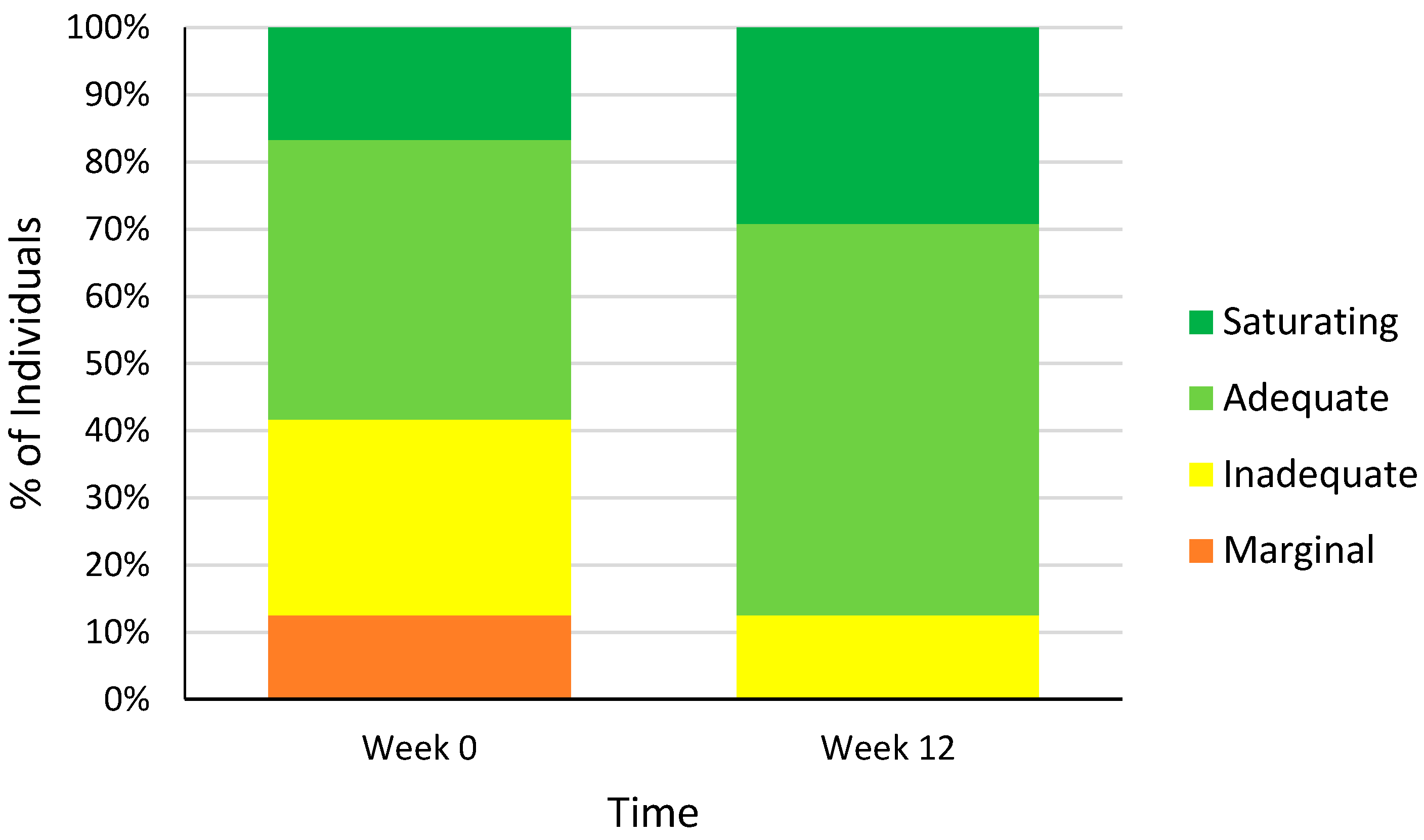
3.5. Plasma Vitamin C Levels
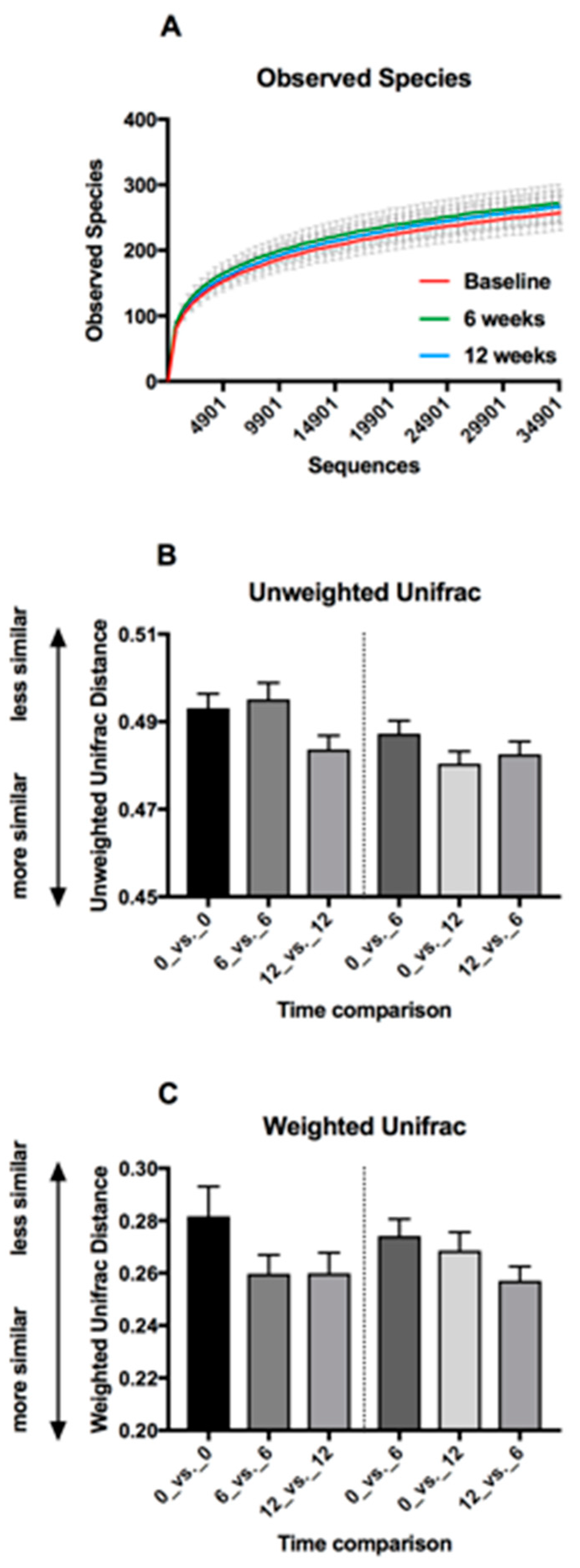
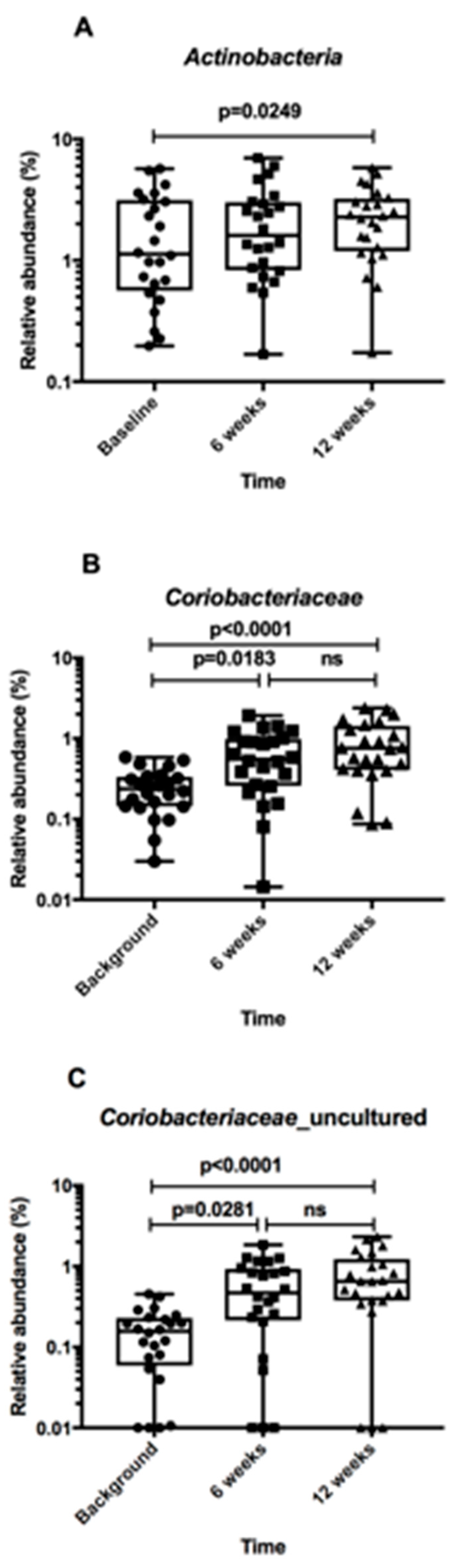
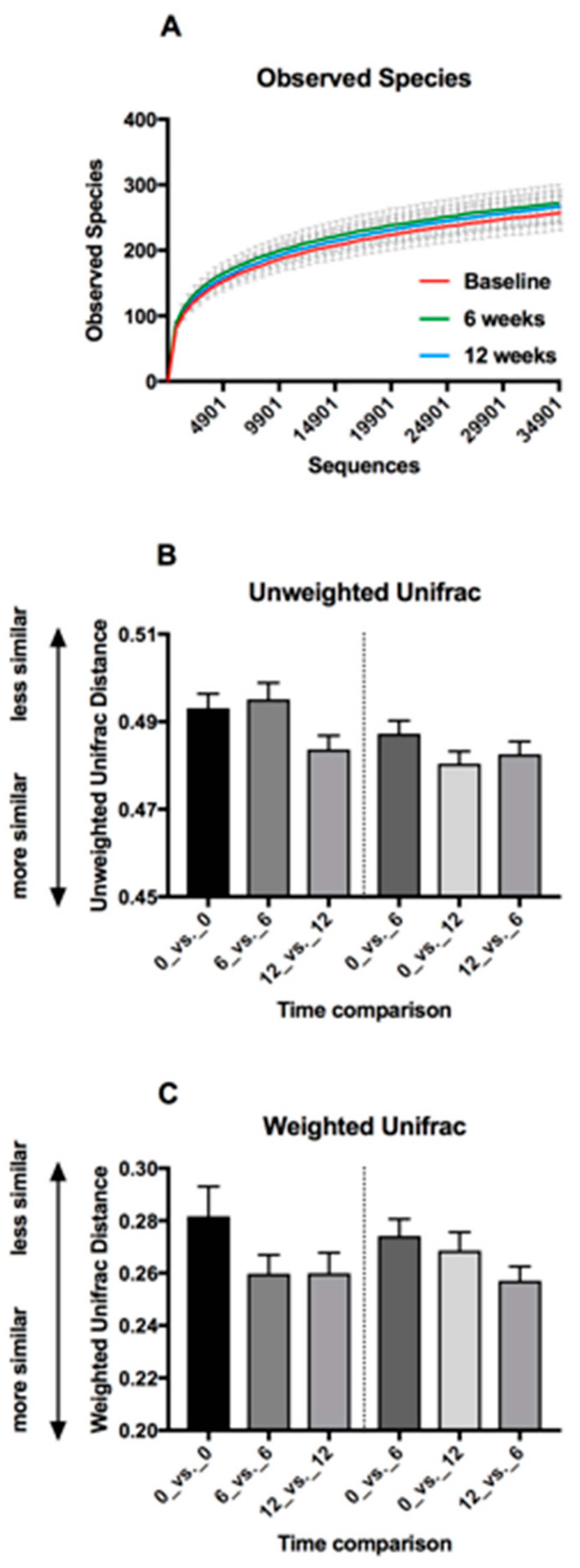
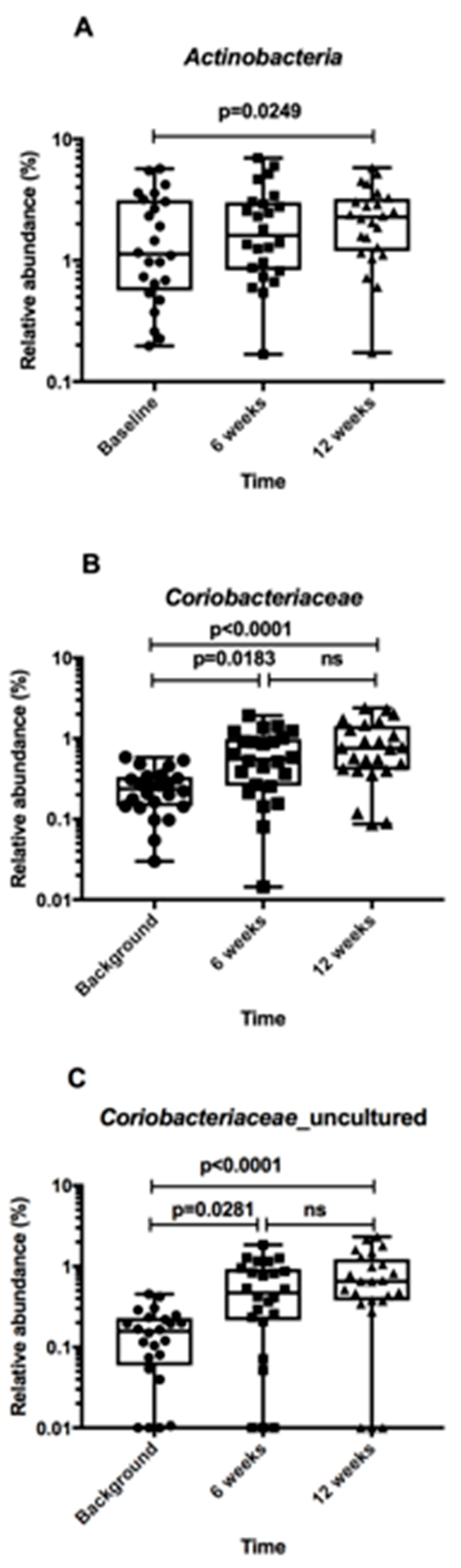
3.6. Faecal Microbiota
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas 2015. Available online: www.diabetesatlas.org (accessed on 12 June 2017).
- World Health Organization, Diabetes Fact Sheet N°312 [Internet], World Health Organization Media Centre. Available online: http://www.who.int/mediacentre/factsheets/fs312/en/index.html (accessed on 12 June 2017).
- Coppell, K.J.; Mann, J.I.; Williams, S.M.; Jo, E.; Drury, P.L.; Miller, J.C.; Parnell, W.R. Prevalence of diagnosed and undiagnosed diabetes and prediabetes in New Zealand: Findings from the 2008/09 Adult Nutrition Survey. N. Z. Med. J. 2013, 126, 23–42. [Google Scholar] [PubMed]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2014, 37, S120–S143. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, L.; Wareham, N.; Bingham, S.; Day, N. Vitamin C and hyperglycemia in the European prospective investigation into cancer-Norfolk (EPIC-Norfolk) study: A population-based study. Diabetes Care 2000, 23, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Feskens, E.J.M.; Virtanen, S.M.; Räsänen, L.; Tuomilehto, J.; Stengård, J.; Pekkanen, J.; Nissinen, A.; Kromhout, D. Dietary factors determining diabetes and impaired glucose tolerance: A 20-year follow-up of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetes Care 1995, 18, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Will, J.; Ford, E.; Bowman, B. Serum vitamin C concentrations and diabetes: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Clin. Nutr. 1999, 70, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Harding, A.-H.; Wareham, N.J.; Bingham, S.A.; Khaw, K.; Luben, R.; Welch, A.; Forouhiet, N.G. Plasma vitamin C level, fruit and vegetable consumption and the risk of new-onset type 2 diabetes mellitus: The European prospective investigation of cancer-Norfolk prospective study. Arch. Intern. Med. 2008, 168, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Na, L.; Shan, R.; Cheng, Y.; Li, Y.; Wu, X.; Sun, C. Dietary Vitamin C Intake Reduces the Risk of Type 2 Diabetes in Chinese Adults: HOMA-IR and T-AOC as Potential Mediators. PLoS ONE 2016, 11, e0163571. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5042374/ (accessed on 12 June 2017). [CrossRef] [PubMed]
- Ellulu, M.S.; Rahmat, A.; Patimah, I.; Khaza’ai, H.; Abed, Y. Effect of vitamin C on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: A randomized controlled trial. Drug Des. Dev. Ther. 2015, 9, 3405–3412. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, A.; Duran-Valdez, E.; Robinson, I.; De Serna, D.; Schade, D. Does Short-term Vitamin C Reduce Cardiovascular Risk in Type 2 Diabetes? Endocr. Pract. 2013, 19, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Dakhale, G.N.; Chaudhari, H.V.; Shrivastava, M. Supplementation of vitamin C reduces blood glucose and improves glycosylated hemoglobin in type 2 diabetes mellitus: A randomized, double-blind study. Adv. Pharmacol. Sci. 2011, 2011, 195271. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Werner, A.D.; Lara, J.; Willis, N.D.; Mathers, J.C.; Siervo, M. Effects of vitamin C supplementation on glycaemic control: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2017, 71, 1371–1380. [Google Scholar] [CrossRef] [PubMed]
- Gillani, S.W.; Sulaiman, S.A.S.; Abdul, M.I.M.; Baig, M.R. Combined effect of metformin with ascorbic acid versus acetyl salicylic acid on diabetes-related cardiovascular complication: A 12-month single blind multicenter randomized control trial. Cardiovasc. Diabetol. 2017, 16, 103. [Google Scholar] [CrossRef] [PubMed]
- Sivakumaran, S.; Huffman, L.; Sivakumaran, S.; Drummond, L. The nutritional composition of Zespri SunGold Kiwifruit and Zespri Sweet Green Kiwifruit. Food Chem. 2018, 238, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Pullar, J.M.; Moran, S.; Vissers, M.C. Bioavailability of vitamin C from kiwifruit in non-smoking males: Determination of ‘healthy’ and ‘optimal’ intakes. J. Nutr. Sci. 2012, 1, e14. [Google Scholar] [CrossRef] [PubMed]
- Monro, J.A. Kiwifruit, Carbohydrate Availability and the Glycemic Response. Adv. Food Nutr. Res. 2013, 68, 257–271. [Google Scholar] [PubMed]
- Sims, I.M.; Monro, J.A. Fiber: Composition, structures and functional properties. Adv. Food Nutr. Res. 2013, 68, 81–99. [Google Scholar] [PubMed]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D.; et al. A Metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; Vogensen, F.K.; Van den Berg, F.W.J.; Nielsen, D.S.; Andreasen, A.S.; Pedersen, B.K.; Al-Soud, W.A.; Sørensen, S.J.; Hansen, L.H.; Jakobsenet, M. Gut Microbiota in Human Adults with Type 2 Diabetes Differs from Non-Diabetic Adults. PLoS ONE 2010, 5, e9085. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.H.; Tremaroli, V.; Nookaew, I.; Bergström, G.; Behre, C.J.; Fagerberg, B.; Nielsen, J.; Bäckhed, F. Gut metagenome in European women with normal, impaired and diabetic glucose control. Nature 2013, 498, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Shen, D.; Fang, Z.; Jie, Z.; Qiu, X.; Zhang, C.; Chen, Y.; Ji, L. Human gut microbiota changes reveal the progression of glucose intolerance. PLoS ONE 2013, 8, e71108. [Google Scholar] [CrossRef] [PubMed]
- Cani, P.D. The gut microbiota manages host metabolism. Nat. Rev. Endocrinol. 2014, 10, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Blatchford, P.; Bentley-Hewitt, K.L.; Stoklosinski, H.; McGhie, T.; Gearry, R.; Gibson, G.; Ansell, J. In vitro characterisation of the fermentation profile and prebiotic capacity of gold-fleshed kiwifruit. Benef. Microbes 2015, 6, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Braatvedt, G.D.; Cundy, T.; Crooke, M.; Florkowski, C.; Mann, J.I.; Lunt, H.; Rodney, J.; Orr-Walker, B.; Timothy, K.; Drury, P.L. Understanding the new HbA1c units for the diagnosis of Type 2 diabetes. N. Z. Med. J. 2012, 125, 70. [Google Scholar] [PubMed]
- World Health Organization. Section 5: Collecting Step 2 Data: Physical Measurements. Available online: http://www.who.int/chp/steps/Part3_Section5.pdf?ua=1 (accessed on 19 June 2017).
- Ricós, C.; Alvarez, V.; Cava, F.; García-Lario, J.V.; Hernández, A.; Jiménez, C.V.; Minchinela, J.; Perich, C.; Simón, M. Current databases on biological variation: Pros, cons and progress. Scand. J. Clin. Lab. Investig. 1999, 59, 491–500. [Google Scholar]
- PullaR, J.M.; Bozonet, S.M.; Carr, A.C. Appropriate Handling, Processing and Analysis of Blood Samples Is Essential to Avoid Oxidation of Vitamin C to Dehydroascorbic Acid. Antioxid 2018, 7, 29. [Google Scholar] [CrossRef] [PubMed]
- Bozkaya, G.; Uzuncan, N.; Bilgili, S.; Demirezen, O. Evaluation of analytical performance of Variant II turbo HbA1c analyzer according to sigma metrics. J. Med. Biochem. 2018, 37, 1–13. [Google Scholar] [CrossRef]
- Bang, A.S.; Soule, S.G.; Yandle, T.G.; Richards, A.M.; Pemberton, C.J. Characterisation of proghrelin peptides in mammalian tissue and plasma. J. Endocrinol. 2007, 192, 313–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Peña, A.G.; Goodrich, J.K.; Gordonet, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335. [Google Scholar] [CrossRef] [PubMed]
- Rognes, T.; Flouri, T.; Nichols, B.; Quince, C.; Mahé, F. VSEARCH: A versatile open source tool for metagenomics. PeerJ 2016, 4, e2584. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate Vitamin C status in prediabetes and type 2 diabetes mellitus: Associations with glycaemic control, obesity, and smoking. Nutrients 2017, 9, 997. [Google Scholar] [CrossRef] [PubMed]
- NHMRC. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes Canberra: ACT: National Health and Medical Research Council. 2006. Available online: https://www.nhmrc.gov.au/_files_nhmrc/file/publications/17122_nhmrc_nrv_update–dietary_intakes–web.pdf (accessed on 12 June 2017).
- IPAQ. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ): Short and Long Forms. 2005. Available online: https://sites.google.com/site/theipaq/ (accessed on 12 June 2017).
- Will, J.C.; Byers, T. Does diabetes mellitus increase the requirement for vitamin C? Nutr. Rev. 1996, 54, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Kositsawat, J.; Freeman, V.L. Vitamin C and A1c relationship in the National Health and Nutrition Examination Survey (NHANES) 2003–2006. J. Am. Coll. Nutr. 2011, 30, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Sinha, M.K.; Garg, H.; Khanna, R.; Khanna, H.D. Oxidative stress in patients with essential hypertension. Natl. Med. J. India 2005, 18, 297–299. [Google Scholar] [PubMed]
- Boland, M. Advances in Food and Nutrition Research. In Nutritional Benefits of Kiwifruit; Moughan, P.J., Ed.; Elsevier Science: Burlington, MA, USA, 2013. [Google Scholar]
- Karlsen, A.; Svendsen, M.; Seljeflot, I.; Laake, P.; Duttaroy, A.K.; Drevon, C.A.; Arnesen, H.; Tonstad, S.; Blomhoffet, R. Kiwifruit decreases blood pressure and whole-blood platelet aggregation in male smokers. J. Hum. Hypertens. 2012, 27, 126. [Google Scholar] [CrossRef] [PubMed]
- Clavel, T.; Lepage, P.; Charrier, C. The family coriobacteriaceae. In The Prokaryotes, 4th ed.; Rosenberg, E., DeLong, E.F., Lory, S., Stackebrandt, E., Thompson, F., Eds.; Springer International Publishing: Berlin, Germany, 2014; pp. 201–238. [Google Scholar]
- Del Rio, D.; Costa, L.G.; Lean, M.E.J.; Crozier, A. Polyphenols and health: What compounds are involved? Nutr. Metab. Cardiovasc. Dis. 2010, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Power, M.E.; Tilman, D.; Estes, J.A.; Menge, B.A.; Bond, W.J.; Mills, L.S.; Daily, G.; Castilla, G.C.; Lubchenco, J.; Paine, R.T. Challenges in the Quest for Keystones. BioScience 1996, 46, 609–620. [Google Scholar] [CrossRef] [Green Version]
- Tigchelaar, E.F.; Bonder, M.J.; Jankipersadsing, S.A.; Fu, J.; Wijmenga, C.; Zhernakova, A. Gut microbiota composition associated with stool consistency. Gut 2015, 65, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.C.; Patel, M.; Plank, L.D.; Ferguson, L.R. Kiwifruit promotes laxation in the elderly. Asia Pac. J. Clin. Nutr. 2002, 11, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.; Leung, G.; Tong, T.; Wong, N.Y. Increasing dietary fiber intake in terms of kiwifruit improves constipation in Chinese patients—Increasing dietary fiber intake in terms of kiwifruit improves constipation in Chinese patients. World J. Gastroenterol. 2007, 13, 4771–4775. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Lin, Y.-T.; Lu, Y.-T.; Liu, Y.-S.; Liu, J.-F. Kiwifruit improves bowel function in patients with irritable bowel syndrome with constipation. Asia Pac. J. Clin. Nutr. 2010, 19, 451–457. [Google Scholar] [PubMed]
- Cunillera, O.; Almeda, J.; Mascort, J.J.; Basora, J.; Marzo-Castillejo, M. Improvement of functional constipation with kiwifruit intake in a Mediterranean patient population: An open, non-randomized pilot study. Revista Española de Nutrición Humana y Dietética 2015, 19, 58–67. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lead-In Phase | Week 0 (Baseline) | Week 6 (Study Mid-Point) | Week 12 (Study Completion) | |
|---|---|---|---|---|
| Questionnaires | Food diary | Demography Medical history Medications Supplements Anthropometry Physical activity | Changes to medications and supplements Anthropometry | Changes to medications and supplements Anthropometry Physical activity Food diary |
| Blood Tests | Fasting glucose vitamin C HbA1c Lipids Hormones hs-CRP | Fasting glucose | Fasting glucose vitamin C HbA1c Lipids Hormones hs-CRP |
| Characteristics | n = 26 |
|---|---|
| Age (years) (mean ± SD) | 66 ± 9 |
| Gender | |
| Female % (n) | 50 (13) |
| Male % (n) | 50 (13) |
| Ethnicity | |
| European % (n) | 81 (21) |
| Māori % (n) | 8 (2) |
| Samoan % (n) | 4 (1) |
| Asian/Chinese % (n) | 4 (1) |
| Other % (n) | 4 (1) |
| Qualification | |
| No qualification % (n) | 27 (7) |
| Secondary school % (n) | 19 (5) |
| Post-secondary certificate, diploma or trade diploma % (n) | 42 (11) |
| University % (n) | 12 (3) |
| Smoking Status | |
| Current smoker % (n) | 15 (4) |
| Ex-smoker % (n) | 39 (10) |
| Non-smoker % (n) | 46 (12) |
| Alcohol Status | |
| Current drinker % (n) | 73 (19) |
| Ex-drinker % (n) | 12 (3) |
| Non-drinker % (n) | 15 (4) |
| Daily Dietary Intake | Week 0 (n = 26) | Week 12 (n = 24) |
|---|---|---|
| Macronutrients | ||
| Energy (KJ) | 7407 ± 2759 | 7176 ± 1683 |
| Fibre (g) | 23 ± 8 | 23 ± 8 |
| Protein (g) | 81 ± 24 | 80 ± 22 |
| Protein (% of energy) | 19 ± 4 | 19 ± 4 |
| Total fat (g) | 72 ± 35 | 68 ± 18 |
| Total fat (% of energy) | 35 ± 6 | 36 ± 6 |
| Total carbohydrate (g) | 190 ± 71 | 184 ± 49 |
| Total carbohydrate (% of energy) | 43 ± 5 | 43 ± 6 |
| Total available sugars (g) | 82 ± 33 | 86 ± 23 |
| Fructose (g) | 16 ± 8 | 22 ± 6 *** |
| Glucose (g) | 14 ± 6 | 20 ± 5 *** |
| Sucrose (g) | 35 ± 25 | 29 ± 16 * |
| Lactose (g) | 14 ± 8 | 20 ± 5 |
| Maltose (g) | 3.0 ± 1.8 | 2.8 ± 1.5 |
| Total starch (g) | 108 ± 43 | 97 ± 34 |
| Micronutrients † | ||
| vitamin C (mg) | 79 ± 35 | 347 ± 70 *** |
| vitamin E (mg) | 8.5 ± 3.9 | 10.3 ± 3.3 * |
| Total folate (µg) | 271 ± 126 | 337 ± 119 * |
| Folate (naturally occurring) (µg) | 236 ± 105 | 291 ± 98 ** |
| Food Groups | ||
| Fresh fruit including kiwifruit (g) | 131 ± 91 | 237 ± 68 *** |
| Fresh fruit excluding kiwifruit (g) | 131 ± 91 | 72 ± 55 *** |
| Total fruit including kiwifruit (g) | 184 ± 101 | 274 ± 104 ** |
| Total fruit excluding kiwifruit (g) | 184 ± 101 | 108 ± 94 ** |
| Characteristics | Week 0 (n = 26) | Week 6 (n = 26) | Week 12 (n = 24) |
|---|---|---|---|
| Anthropometry | |||
| Weight (kg) | 80.2 ± 19.8 | 80.1 ± 20.0 | 77.9 ± 18.6 |
| BMI (kg/m2) | 29.4 ± 7.3 | 29.4 ± 7.4 | 28.6 ± 7.0 |
| Fat mass (%) | 34.3 ± 6.6 | 34.4 ± 6.6 | 34.0 ± 6.9 |
| Waist circumference (cm) | 98.6 ± 15.3 | 97.7 ± 15.2 * | 95.5 ± 14.6 *** |
| Waist-to-hip ratio | 0.90 ± 0.09 | 0.90 ± 0.09 | 0.89 ± 0.09 * |
| Blood Pressure | |||
| Diastolic (mmHg) | 76 ± 8 | 73 ± 9 * | 72 ± 10 * |
| Systolic (mmHg) | 129 ± 14 | 124 ± 17 * | 123 ± 18 ** |
| Physical Activity | |||
| (met-minutes/week) | 3598 ± 5273 |
| Biochemical Indices | Week 0 (n = 26) | Week 12 (n = 24) |
|---|---|---|
| HbA1c (mmol/mol) | 43 ± 2 | 42 ± 2 ** |
| Fasting Glucose (mmol/L) | 5.4 ± 0.7 | 5.5 ± 0.8 * |
| Plasma vitamin C (µmol/L) | 50 ± 19 | 64 ± 13 *** |
| Total cholesterol (mmol/L) | 5.2 ± 1.3 | 5.1 ± 1.3 |
| HDL cholesterol (mmol/L) | 1.35 ± 0.23 | 1.35 ± 0.23 |
| LDL cholesterol (mmol/L) | 3.3 ± 1.0 | 3.3 ± 1.1 |
| Triglycerides (mmol/L) | 1.1 ± 0.5 | 1.1 ± 0.4 |
| Cholesterol (total/HDL) ratio | 3.9 ± 0.9 | 3.8 ± 0.9 |
| hs-CRP (mg/L) | 1.8 (0.6–3.2) | 0.9 (0.5–2.2) |
| Insulin (pmol/L) | 51 (31–73) | 42 (31–67) |
| Ghrelin (pmol/L) | 162 (110–204) | 154 (119–206) |
| Leptin (ng/mL) | 38 (27–71) | 35 (25–75) |
| Adiponectin (µg/mL) | 9 (6–11) | 10 (7–12) |
| Diversity Measure | Week 0 (n = 22) | Week 6 (n = 22) | Week 12 (n = 21) |
|---|---|---|---|
| Observed species | 250 (213–316) | 279 (232–306) | 241 (217–283) |
| Whole tree (PD) | 19 (17–23) | 21 (18–22) | 20 (17–22) |
| Shannon index | 5.1 (4.6–5.4) | 5.4 (4.7–5.8) | 5.0 (4.9–5.3) |
| Simpson’s diversity | 0.95 (0.91–0.96) | 0.96 (0.93–0.97) | 0.94 (0.93–0.95) |
| Chao index | 318 (257–377) | 367 (288–396) | 338 (307–389) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, R.; Willis, J.; Gearry, R.B.; Hughes, A.; Lawley, B.; Skidmore, P.; Frampton, C.; Fleming, E.; Anderson, A.; Jones, L.; et al. SunGold Kiwifruit Supplementation of Individuals with Prediabetes Alters Gut Microbiota and Improves Vitamin C Status, Anthropometric and Clinical Markers. Nutrients 2018, 10, 895. https://doi.org/10.3390/nu10070895
Wilson R, Willis J, Gearry RB, Hughes A, Lawley B, Skidmore P, Frampton C, Fleming E, Anderson A, Jones L, et al. SunGold Kiwifruit Supplementation of Individuals with Prediabetes Alters Gut Microbiota and Improves Vitamin C Status, Anthropometric and Clinical Markers. Nutrients. 2018; 10(7):895. https://doi.org/10.3390/nu10070895
Chicago/Turabian StyleWilson, Renée, Jinny Willis, Richard B. Gearry, Alan Hughes, Blair Lawley, Paula Skidmore, Chris Frampton, Elizabeth Fleming, Angie Anderson, Lizzie Jones, and et al. 2018. "SunGold Kiwifruit Supplementation of Individuals with Prediabetes Alters Gut Microbiota and Improves Vitamin C Status, Anthropometric and Clinical Markers" Nutrients 10, no. 7: 895. https://doi.org/10.3390/nu10070895