Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65°North)


Abstract
:1. Introduction
2. Methods
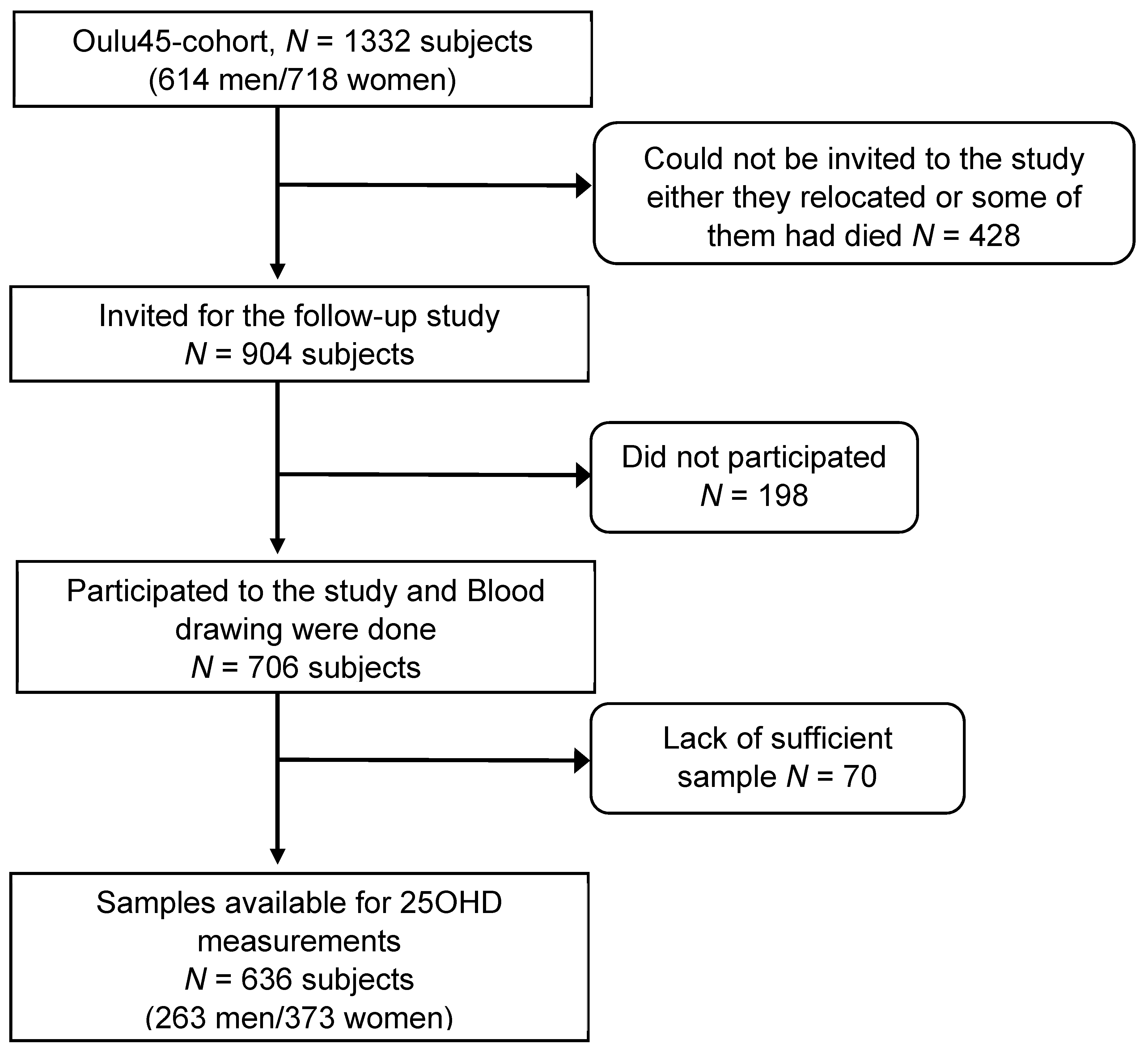
2.1. Study Population
2.2. Study Protocol
2.3. 25OHD Measurements
2.4. Definitions of MetS and Vitamin D Status
2.5. Statistics
3. Results
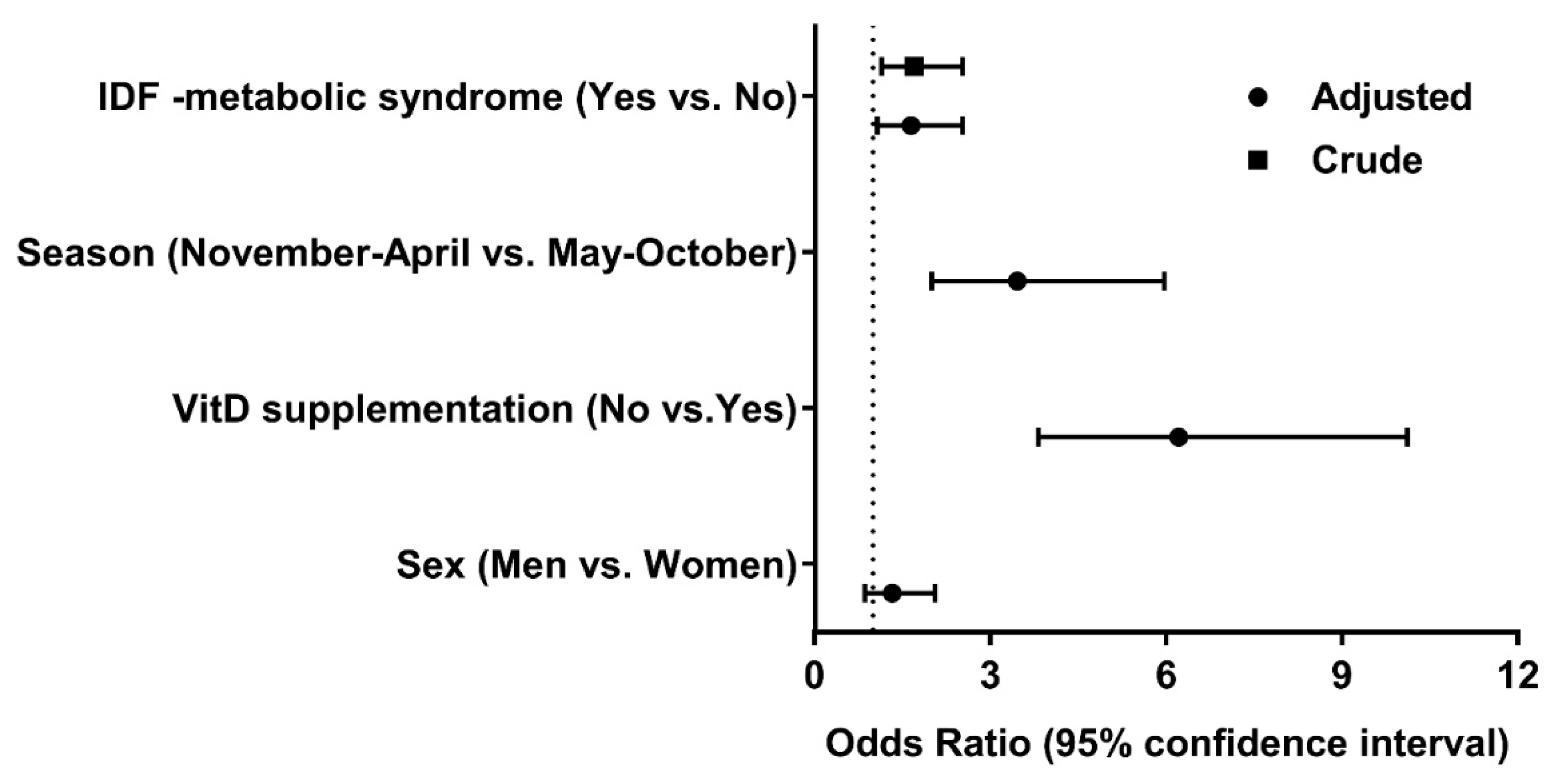
Vitamin D Levels and the components of MetS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mutt, S.J.; Hypponen, E.; Saarnio, J.; Jarvelin, M.R.; Herzig, K.H. Vitamin D and adipose tissue-more than storage. Front. Physiol. 2014, 5, 228. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Huotari, A.; Herzig, K.H. Vitamin D and living in northern latitudes--an endemic risk area for vitamin D deficiency. Int. J. Circumpolar Health 2008, 67, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Hassi, J.; Sikkila, K.; Ruokonen, A.; Leppaluoto, J. The pituitary-thyroid axis in healthy men living under subarctic climatological conditions. J. Endocrinol. 2001, 169, 195–203. [Google Scholar] [CrossRef] [Green Version]
- MacLaughlin, J.; Holick, M.F. Aging decreases the capacity of human skin to produce vitamin D3. J. Clin. Investig. 1985, 76, 1536–1538. [Google Scholar] [CrossRef] [PubMed]
- Hurskainen, A.; Virtanen, J.K.; Tuomainen, T.; Nurmi, T.; Voutilainen, S. Association of serum 25-hydroxyvitamin D with type 2 diabetes and markers of insulin resistance in a general older population in Finland. Diabetes. Metab. Res. 2012, 28, 418–423. [Google Scholar] [CrossRef]
- Jablonski, K.L.; Chonchol, M.; Pierce, G.L.; Walker, A.E.; Seals, D.R. 25-Hydroxyvitamin D deficiency is associated with inflammation-linked vascular endothelial dysfunction in middle-aged and older adults. Hypertension 2011, 57, 63–69. [Google Scholar] [CrossRef]
- Cheng, S.; Massaro, J.M.; Fox, C.S.; Larson, M.G.; Keyes, M.J.; McCabe, E.L.; Robins, S.J.; O’Donnell, C.J.; Hoffmann, U.; Jacques, P.F.; et al. Adiposity, cardiometabolic risk, and vitamin D status: The Framingham Heart Study. Diabetes 2010, 59, 242–248. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, P.; Wang, F.; Yang, J.; Liu, Z.; Qin, H. Association between vitamin D and risk of colorectal cancer: A systematic review of prospective studies. J. Clin. Oncol. 2011, 29, 3775–3782. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Michos, E.D.; Post, W.; Astor, B. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch. Intern. Med. 2008, 168, 1629–1637. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. IDF Epidemiology Task Force Consensus Group The metabolic syndrome--a new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Scuteri, A.; Najjar, S.S.; Morrell, C.H.; Lakatta, E.G. Cardiovascular Health Study The metabolic syndrome in older individuals: Prevalence and prediction of cardiovascular events: The Cardiovascular Health Study. Diabetes Care 2005, 28, 882–887. [Google Scholar] [CrossRef]
- Despres, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Mutt, S.J.; Karhu, T.; Lehtonen, S.; Lehenkari, P.; Carlberg, C.; Saarnio, J.; Sebert, S.; Hypponen, E.; Jarvelin, M.R.; Herzig, K.H. Inhibition of cytokine secretion from adipocytes by 1,25-dihydroxyvitamin D(3) via the NF-kappaB pathway. FASEB J. 2012, 26, 4400–4407. [Google Scholar] [CrossRef]
- Pham, T.M.; Ekwaru, J.P.; Setayeshgar, S.; Veugelers, P.J. The Effect of Changing Serum 25-Hydroxyvitamin D Concentrations on Metabolic Syndrome: A Longitudinal Analysis of Participants of a Preventive Health Program. Nutrients 2015, 7, 7271–7284. [Google Scholar] [CrossRef] [Green Version]
- Vitezova, A.; Zillikens, M.C.; van Herpt, T.T.; Sijbrands, E.J.; Hofman, A.; Uitterlinden, A.G.; Franco, O.H.; Kiefte-de Jong, J.C. Vitamin D status and metabolic syndrome in the elderly: The Rotterdam Study. Eur. J. Endocrinol. 2015, 172, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Bea, J.W.; Jurutka, P.W.; Hibler, E.A.; Lance, P.; Martinez, M.E.; Roe, D.J.; Sardo Molmenti, C.L.; Thompson, P.A.; Jacobs, E.T. Concentrations of the vitamin D metabolite 1,25(OH)2D and odds of metabolic syndrome and its components. Metabolism 2015, 64, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Yu, Z.; Pan, A.; Hu, F.B.; Franco, O.H.; Li, H.; Li, X.; Yang, X.; Chen, Y.; Lin, X. Plasma 25-hydroxyvitamin D concentration and metabolic syndrome among middle-aged and elderly Chinese individuals. Diabetes Care 2009, 32, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; Eguchi, M.; Kurotani, K.; Kochi, T.; Kashino, I.; Ito, R.; Kuwahara, K.; Tsuruoka, H.; Kabe, I.; Mizoue, T. Serum 25-hydroxyvitamin D and metabolic syndrome in a Japanese working population: The Furukawa Nutrition and Health Study. Nutrition 2017, 36, 26–32. [Google Scholar] [CrossRef]
- Reis, J.P.; von Mühlen, D.; Kritz-Silverstein, D.; Wingard, D.L.; Barrett-Connor, E. Vitamin D, parathyroid hormone levels, and the prevalence of metabolic syndrome in community-dwelling older adults. Diabetes Care 2007, 30, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Bonakdaran, S.; Fakhraee, F.; Karimian, M.S.; Mirhafez, S.R.; Rokni, H.; Mohebati, M.; Mazidi, M.; Mousavi, M.; Ferns, G.A.; Ghayour-Mobarhan, M. Association between serum 25-hydroxyvitamin D concentrations and prevalence of metabolic syndrome. Adv. Med. Sci. 2016, 61, 219–223. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J. Vitamin D: An overview of vitamin D status and intake in E urope. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Lehtonen-Veromaa, M.; Möttönen, T.; Leino, A.; Heinonen, O.J.; Rautava, E.; Viikari, J. Prospective study on food fortification with vitamin D among adolescent females in Finland: Minor effects. Br. J. Nutr. 2008, 100, 418–423. [Google Scholar] [CrossRef]
- Männistö, S.; Ovaskainen, M.; Valsta, L. The national Findiet 2002 study. Publ. Natl. Public Health Inst. B 2003, 3, 2003. [Google Scholar]
- Helldán, A.; Raulio, S.; Kosola, M.; Tapanainen, H.; Ovaskainen, M.; Virtanen, S. Finravinto 2012-tutkimus: The National FINDIET 2012 Survey; Raportti: 16/2013; National Institute for Health and Welfare: Helsinki, Finland, 2013. [Google Scholar]
- Lamberg-Allardt, C.; Viljakainen, H. A Working Group Follow-up Study on the Vitamin D Status in the Finnish Population 2002 and 2004; Reports of the Ministry of Social Affairs and Health; Ministry of Social Affairs and Health: Helsinki, Finland, 2006. [Google Scholar]
- Metsämarttila, E.; Rodilla, E.; Jokelainen, J.; Herrala, S.; Leppäluoto, J.; Keinänen-Kiukaanniemi, S.; Herzig, K. Effect of physical activity on pulse wave velocity in elderly subjects with normal glucose, prediabetes or Type 2 Diabetes. Sci. Rep. 2018, 8, 8045. [Google Scholar] [CrossRef] [PubMed]
- Stenbäck, V.; Mutt, S.J.; Leppäluoto, J.; Gagnon, D.D.; Mäkelä, K.A.; Jokelainen, J.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. Association of physical activity with telomere length among elderly adults—The Oulu cohort 1945. Front. Physiol. 2019, 10, 444. [Google Scholar] [CrossRef]
- Ala-Kokko, T.I.; Mutt, S.J.; Nisula, S.; Koskenkari, J.; Liisanantti, J.; Ohtonen, P.; Poukkanen, M.; Laurila, J.J.; Pettila, V.; Herzig, K.H.; FINNAKI Study Group. Vitamin D deficiency at admission is not associated with 90-day mortality in patients with severe sepsis or septic shock: Observational FINNAKI cohort study. Ann. Med. 2016, 48, 67–75. [Google Scholar] [CrossRef]
- Vayrynen, J.P.; Mutt, S.J.; Herzig, K.H.; Vayrynen, S.A.; Kantola, T.; Karhu, T.; Karttunen, T.J.; Klintrup, K.; Makela, J.; Makinen, M.J.; et al. Decreased preoperative serum 25-Hydroxyvitamin D levels in colorectal cancer are associated with systemic inflammation and serrated morphology. Sci. Rep. 2016, 6, 36519. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Boonen, S.; Brandi, M.; Bruyère, O.; Cooper, C.; Kanis, J.A.; Kaufman, J.; Ringe, J.; Weryha, G.; Reginster, J. Vitamin D supplementation in elderly or postmenopausal women: A 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Curr. Med. Res. Opin. 2013, 29, 305–313. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hiraki, L.T.; Cooper, J.D.; Dastani, Z.; Li, R.; Houston, D.K.; et al. Causal relationship between obesity and vitamin D status: Bi-directional Mendelian randomization analysis of multiple cohorts. PLoS Med. 2013, 10, e1001383. [Google Scholar] [CrossRef]
- Kelloniemi, H.; Ek, E.; Laitinen, J. Optimism, dietary habits, body mass index and smoking among young Finnish adults. Appetite 2005, 45, 169–176. [Google Scholar] [CrossRef]
- Uusitupa, M.; Hermansen, K.; Savolainen, M.; Schwab, U.; Kolehmainen, M.; Brader, L.; Mortensen, L.; Cloetens, L.; Johansson-Persson, A.; Önning, G. Effects of an isocaloric healthy N ordic diet on insulin sensitivity, lipid profile and inflammation markers in metabolic syndrome–a randomized study (SYSDIET). J. Intern. Med. 2013, 274, 52–66. [Google Scholar] [CrossRef]
- Brader, L.; Rejnmark, L.; Carlberg, C.; Schwab, U.; Kolehmainen, M.; Rosqvist, F.; Cloetens, L.; Landin-Olsson, M.; Gunnarsdottir, I.; Poutanen, K.S. Effects of a healthy Nordic diet on plasma 25-hydroxyvitamin D concentration in subjects with metabolic syndrome: A randomized, placebo-controlled trial (SYSDIET). Eur. J. Nutr. 2014, 53, 1123–1134. [Google Scholar] [CrossRef]
- Rock, C.L.; Emond, J.A.; Flatt, S.W.; Heath, D.D.; Karanja, N.; Pakiz, B.; Sherwood, N.E.; Thomson, C.A. Weight loss is associated with increased serum 25-hydroxyvitamin D in overweight or obese women. Obesity 2012, 20, 2296–2301. [Google Scholar] [CrossRef]
- Saukkonen, T.; Mutt, S.J.; Jokelainen, J.; Saukkonen, A.; Raza, G.S.; Karhu, T.; Härkönen, P.; Eckel, J.; Herzig, K.; Rajala, U.; et al. Adipokines and inflammatory markers in elderly subjects with high risk of type 2 diabetes and cardiovascular disease. Sci. Rep. 2018, 8, 12816. [Google Scholar] [CrossRef]
- Ju, S.Y.; Jeong, H.S.; Kim, D.H. Blood vitamin D status and metabolic syndrome in the general adult population: A dose-response meta-analysis. J. Clin. Endocrinol. Metab. 2014, 99, 1053–1063. [Google Scholar] [CrossRef]
- Itkonen, S.T.; Skaffari, E.; Saaristo, P.; Saarnio, E.M.; Erkkola, M.; Jakobsen, J.; Cashman, K.D.; Lamberg-Allardt, C. Effects of vitamin D2-fortified bread v. supplementation with vitamin D2 or D3 on serum 25-hydroxyvitamin D metabolites: An 8-week randomised-controlled trial in young adult Finnish women. Br. J. Nutr. 2016, 115, 1232–1239. [Google Scholar] [CrossRef]
- Cashman, K.D.; Seamans, K.M.; Lucey, A.J.; Stocklin, E.; Weber, P.; Kiely, M.; Hill, T.R. Relative effectiveness of oral 25-hydroxyvitamin D3 and vitamin D3 in raising wintertime serum 25-hydroxyvitamin D in older adults. Am. J. Clin. Nutr. 2012, 95, 1350–1356. [Google Scholar] [CrossRef] [Green Version]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hypponen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Deficiency (<50 nmol/L) | Insufficiency (50–75 nmol/L) | Sufficiency (≥75 nmol/L) | p Value | |
|---|---|---|---|---|---|
| Number of subjects | 636 | 139 (21.9) | 366 (57.5) | 131 (20.6) | |
| Age (years) | 69.0 ± 0.5 | 68.9 ± 0.5 | 69.0 ± 0.5 | 69.0 ± 0.5 | 0.241 |
| Gender | 0.030 | ||||
| Men | 263 (41.2) | 63 (24.0) | 159 (60.5) | 41 (15.6) | |
| Women | 373 (58.8) | 76 (20.4) | 207 (55.5) | 90 (24.1) | |
| Physical activity | <0.001 | ||||
| Sedentary | 55 (9.2) | 23 (41.8) | 29 (52.7) | 3 (5.5) | |
| Moderate | 345 (58.0) | 79 (22.9) | 195 (56.5) | 71 (20.6) | |
| Vigorous | 195 (32.8) | 32 (16.4) | 115 (59.0) | 48 (24.6) | |
| Season of blood sampling | <0.001 | ||||
| May-October | 170 (29.5) | 20 (11.8) | 110 (64.7) | 40 (23.5) | |
| November-April | 406 (70.5) | 113 (27.8) | 223 (54.9) | 70 (17.2) | |
| Vitamin D supplements | <0.001 | ||||
| No | 328 (51.6) | 111 (33.8) | 177 (54.0) | 40 (12.2) | |
| Yes | 308 (48.4) | 28 (9.1) | 189 (61.4) | 91 (29.5) | |
| Smoking | 0.090 | ||||
| Current | 76 (12.2) | 25 (32.9) | 40 (52.6) | 11 (14.5) | |
| Former | 219 (35.3) | 45 (20.5) | 120 (54.8) | 54 (24.7) | |
| Never | 326 (52.5) | 69 (21.2) | 192 (58.9) | 65 (19.9) | |
| Alcohol | 1.7 ± 3.6 | 2.5 ± 4.7 | 1.5 ± 3.3 | 1.6 ± 2.7 | 0.336 |
| Total | Deficiency (<50 nmol/L) | Insufficiency (50–75 nmol/L) | Sufficiency (≥75 nmol/L) | p Value | p * Value | p ** Value | |
|---|---|---|---|---|---|---|---|
| 25OHD levels (nmol/L) | 62.9 ± 18.5 | 41.5 ± 7.1 | 61.7 ± 6.8 | 89.1 ± 17.3 | <0.001 | ||
| BMI | 27.6 ± 4.8 | 28.6 ± 4.8 | 27.7 ± 4.7 | 26.4 ± 4.7 | <0.001 | 0.132 | |
| Waist circumference (cm) | 93.8 ± 13.7 | 96.7 ± 14.0 | 94.0 ± 13.0 | 90.3 ± 14.3 | <0.001 | 0.286 | 0.847 |
| Lean body mass (kg) | 47.0 ± 9.6 | 47.6 ± 9.7 | 47.4 ± 9.7 | 45.2 ± 9.0 | 0.143 | 0.516 | 0.817 |
| Fat mass (kg) | 26.1 ± 10.1 | 28.0 ± 10.5 | 26.0 ± 10.4 | 24.7 ± 8.7 | 0.083 | 0.488 | 0.369 |
| Fasting glucose (mmol/L) | 5.7 ± 1.0 | 5.8 ± 0.8 | 5.8 ± 1.2 | 5.6 ± 0.7 | 0.010 | 0.502 | 0.903 |
| Fasting insulin (mmol/L) | 15.4 ± 17.3 | 17.4 ± 18.5 | 15.7 ± 18.8 | 12.6 ± 9.4 | <0.001 | 0.225 | 0.737 |
| Total cholesterol (mmol/L) | 5.3 ± 1.2 | 5.6 ± 1.3 | 5.2 ± 1.2 | 5.2 ± 1.3 | 0.024 | 0.004 | 0.001 |
| HDL cholesterol (mmol/L) | 1.7 ± 0.5 | 1.6 ± 0.5 | 1.6 ± 0.5 | 1.7 ± 0.5 | 0.084 | 0.761 | 0.369 |
| LDL cholesterol (mmol/L) | 3.4 ± 1.1 | 3.6 ± 1.2 | 3.3 ± 1.0 | 3.2 ± 1.1 | 0.052 | 0.036 | 0.021 |
| Triglycerides (mmol/L) | 1.3 ± 0.7 | 1.5 ± 1.2 | 1.2 ± 0.5 | 1.0 ± 0.4 | <0.001 | <0.001 | 0.001 |
| DP (mmHg) | 85.5 ± 9.6 | 87.0 ± 8.7 | 85.2 ± 9.9 | 84.8 ± 9.6 | 0.057 | 0.182 | 0.332 |
| SP (mmHg) | 144.1 ± 17.4 | 144.6 ± 17.2 | 144.3 ± 16.7 | 143.2 ± 19.4 | 0.600 | 0.242 | 0.272 |
| HOMA_B | 109.4 ± 41.9 | 115.0 ± 43.6 | 108.7 ± 41.1 | 105.3 ± 41.9 | 0.058 | 0.301 | 0.545 |
| HOMA_S | 71.7 ± 39.8 | 64.0 ± 36.1 | 70.9 ± 39.5 | 81.8 ± 42.7 | <0.001 | 0.243 | 0.610 |
| HOMA_IR | 1.9 ± 1.3 | 2.1 ± 1.5 | 1.9 ± 1.3 | 1.7 ± 1.2 | <0.001 | 0.106 | 0.342 |
| Components | Total Cases | 25OHD Level | p Value | Vitamin D Supplementation | p Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Deficiency (<50 nmol/L) | Insufficiency (50–75 nmol/L) | Sufficiency (≥75 nmol/L) | No | Yes | |||||||||
| Number | Percentage | Number | Percentage | Number | Percentage | Number | Percentage | Number | Percentage | ||||
| Metabolic syndrome (IDF) | |||||||||||||
| No | 313 | 54 | 17.3 | 187 | 59.7 | 72 | 23.0 | 0.016 | 141 | 45.1 | 172 | 54.9 | <0.001 |
| Yes | 319 | 84 | 26.3 | 176 | 55.2 | 59 | 18.5 | 183 | 57.4 | 136 | 42.6 | ||
| Waist circumference (cm) | |||||||||||||
| Men < 94 & Women < 80 | 175 | 20 | 11.4 | 109 | 62.3 | 46 | 26.3 | <0.001 | 83 | 47.4 | 92 | 52.6 | 0.043 |
| Men ≥ 94 & Women ≥ 80 | 457 | 118 | 25.8 | 254 | 55.6 | 85 | 18.6 | 241 | 52.7 | 216 | 47.3 | ||
| Triglyceride (mg/dL) | |||||||||||||
| <150 | 374 | 80 | 21.4 | 222 | 59.4 | 72 | 19.2 | 0.491 | 183 | 48.9 | 191 | 51.1 | 0.074 |
| ≥150 | 259 | 58 | 22.4 | 144 | 55.6 | 57 | 22.0 | 144 | 55.6 | 115 | 44.4 | ||
| HDL cholesterol (mg/dL) | |||||||||||||
| Men ≥ 40 & women ≥ 50 | 394 | 85 | 21.6 | 232 | 58.9 | 77 | 19.5 | 0.732 | 193 | 49.0 | 201 | 51.0 | 0.034 |
| Men < 40 & women<50 | 239 | 53 | 22.2 | 134 | 56.1 | 53 | 21.7 | 134 | 56.1 | 105 | 43.9 | ||
| Blood pressure (mmHg) | |||||||||||||
| No (<130/85) | 106 | 19 | 17.9 | 58 | 54.8 | 29 | 27.3 | 0.192 | 43 | 40.6 | 63 | 59.4 | 0.006 |
| Yes (≥130/85) | 527 | 120 | 22.8 | 305 | 57.9 | 102 | 19.3 | 282 | 53.5 | 245 | 46.5 | ||
| Fasting glucose (mg/dL) | |||||||||||||
| <100 | 296 | 59 | 19.9 | 164 | 55.4 | 73 | 24.7 | 0.058 | 128 | 43.2 | 168 | 56.8 | <0.001 |
| ≥100 | 337 | 80 | 23.7 | 199 | 59.1 | 58 | 17.2 | 197 | 58.5 | 140 | 41.5 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mutt, S.J.; Jokelainen, J.; Sebert, S.; Auvinen, J.; Järvelin, M.-R.; Keinänen-Kiukaanniemi, S.; Herzig, K.-H. Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65°North). Nutrients 2019, 11, 1229. https://doi.org/10.3390/nu11061229
Mutt SJ, Jokelainen J, Sebert S, Auvinen J, Järvelin M-R, Keinänen-Kiukaanniemi S, Herzig K-H. Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65°North). Nutrients. 2019; 11(6):1229. https://doi.org/10.3390/nu11061229
Chicago/Turabian StyleMutt, Shivaprakash Jagalur, Jari Jokelainen, Sylvain Sebert, Juha Auvinen, Marjo-Riitta Järvelin, Sirkka Keinänen-Kiukaanniemi, and Karl-Heinz Herzig. 2019. "Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65°North)" Nutrients 11, no. 6: 1229. https://doi.org/10.3390/nu11061229