
Galectins-1, -3 and -9 Are Present in Breast Milk and Have a Role in Early Life Development

 ,
,  , , ,
, , ,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort and Study Subjects
2.2. Maternal Plasma and Arterial Umbilical Cord Sampling
2.3. Breast Milk Samples
2.4. Determination of Gal Concentrations
2.5. Data Processing and Statistical Analysis
3. Results
3.1. Galectins in Plasma from Mother–Infant Pairs
3.1.1. Clinical Characteristics
3.1.2. Galectins Concentration in MP and UCP
3.1.3. Association of Maternal and Infant Factors with Galectins Concentrations
3.2. Galectins Presence in Breast Milk
3.2.1. Clinical Characteristics
3.2.2. Galectin Levels in Transitional Milk at Day 7 and 15
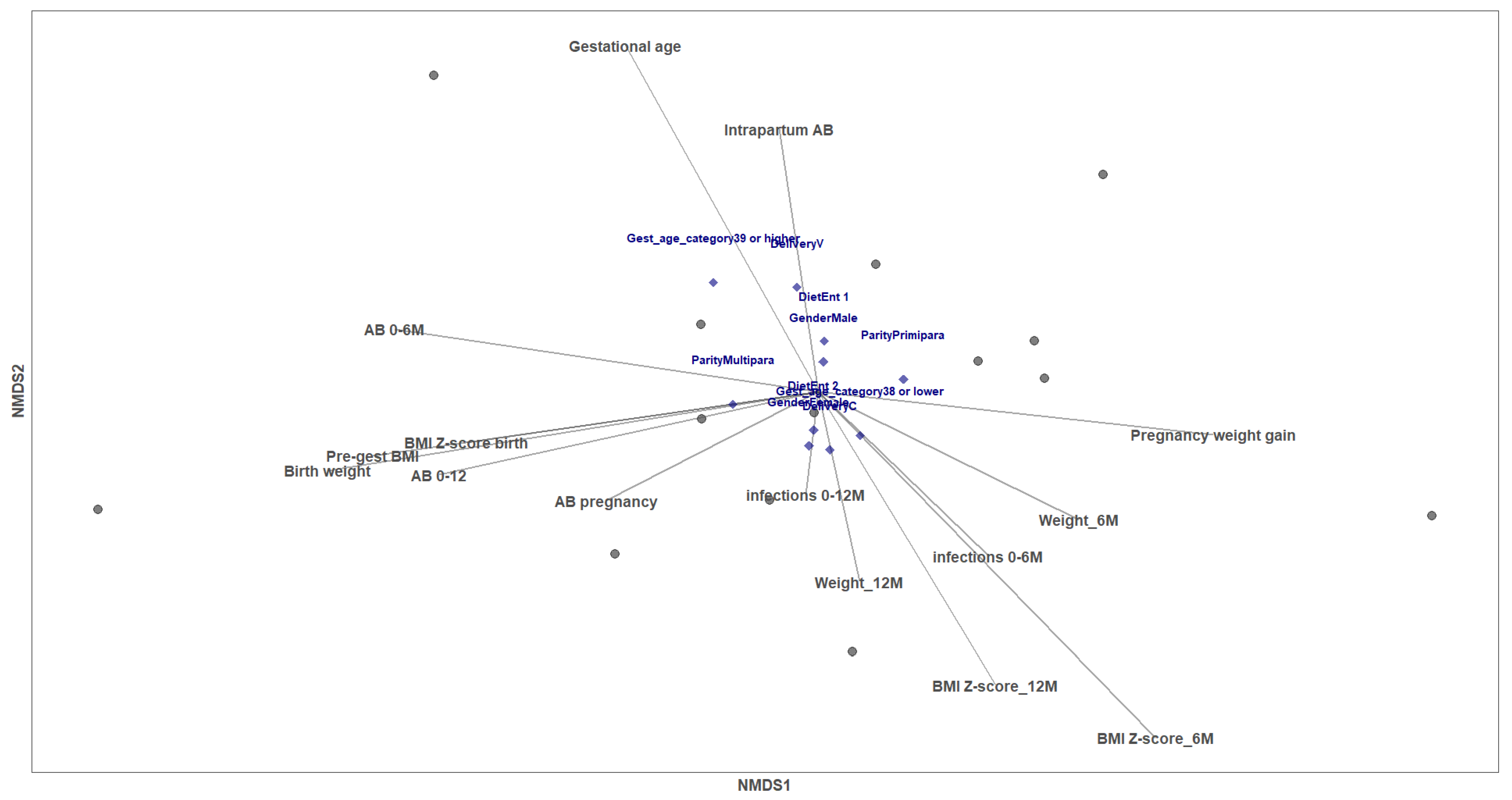
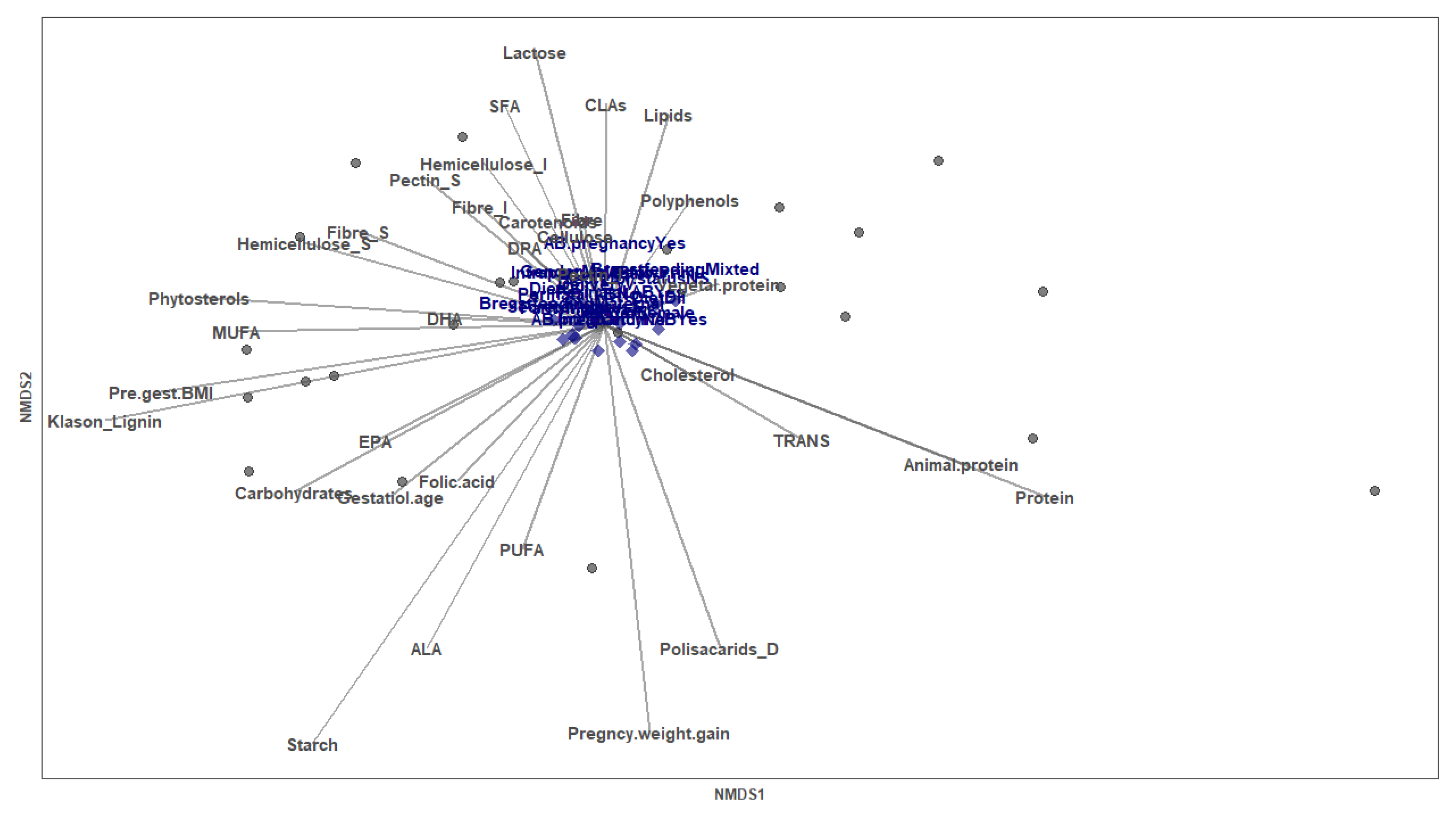
3.2.3. Perinatal Factors Shaping Galectin Levels in Breastmilk
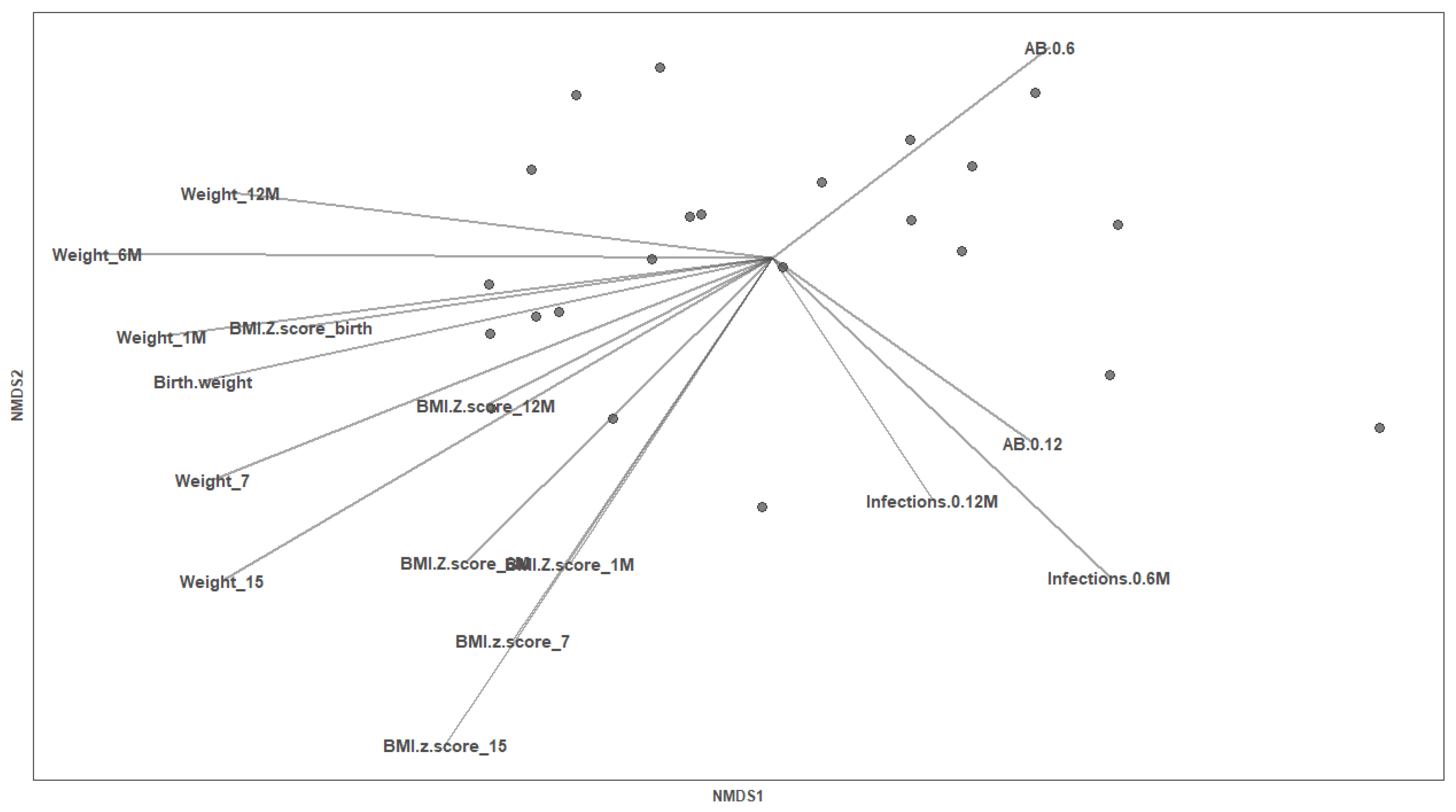
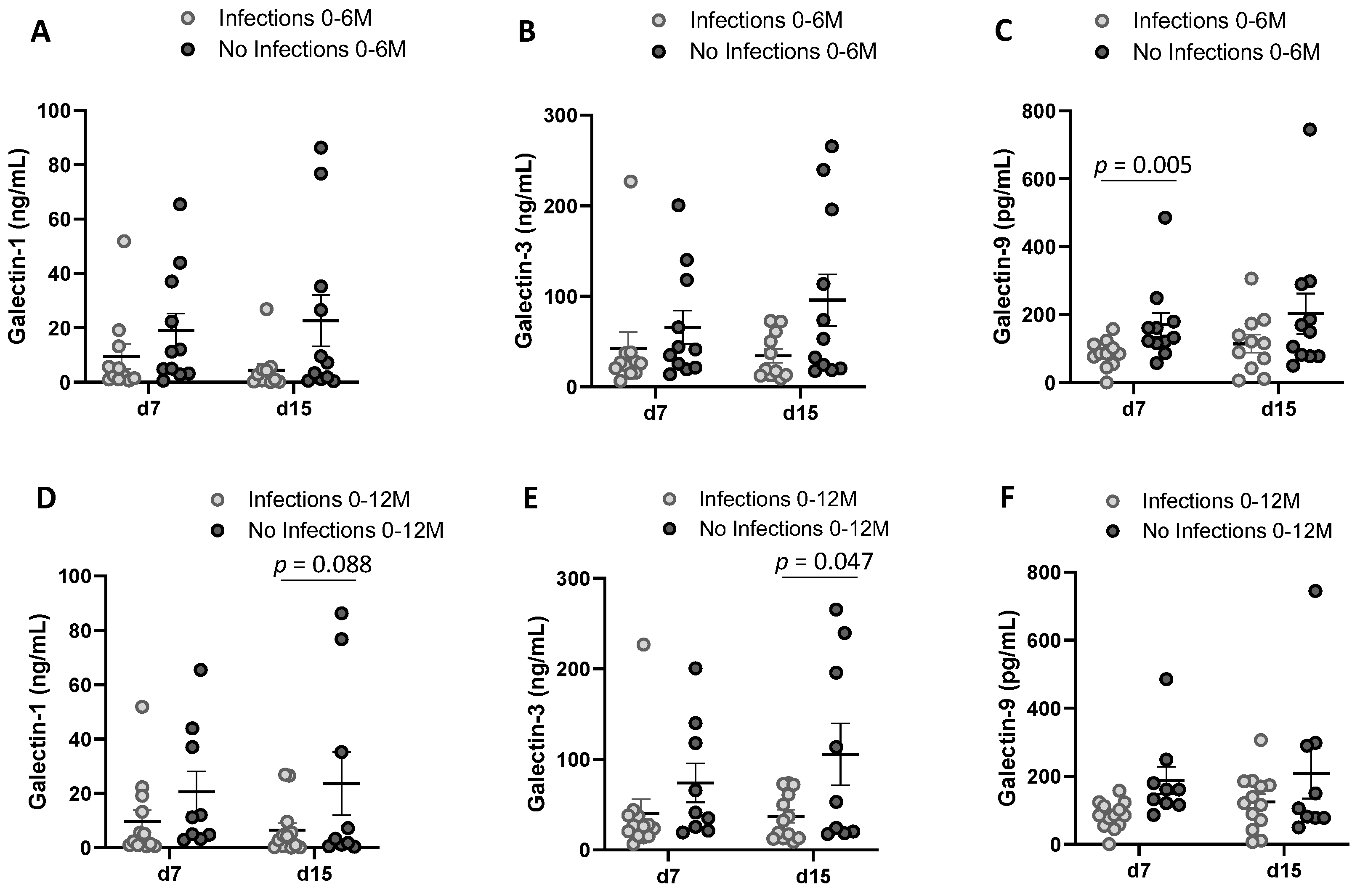
3.2.4. Infant Factors Associated with Breast Milk Galectin Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leffler, H.; Carlsson, S.; Hedlund, M.; Qian, Y.; Poirier, F. Introduction to Galectins. Glycoconj. J. 2002, 19, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.-W.; Beom Hong, S.; Hoe Kim, J.; do Kwon, H.; Kyu Song, H. Structural Basis for Recognition of Autophagic Receptor NDP52 by the Sugar Receptor Galectin-8. Nat. Commun. 2013, 4, 1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiemann, S.; Baum, L.G. Galectins and Immune Responses—Just How Do They Do Those Things They Do? Annu. Rev. Immunol. 2016, 34, 243–264. [Google Scholar] [CrossRef]
- Yang, R.-Y.; Hill, P.N.; Hsu, D.K.; Liu, F.-T. Role of the Carboxyl-Terminal Lectin Domain in Self-Association of Galectin-3. Biochemistry 1998, 37, 4086–4092. [Google Scholar] [CrossRef] [PubMed]
- Lepur, A.; Salomonsson, E.; Nilsson, U.J.; Leffler, H. Ligand Induced Galectin-3 Protein Self-Association. J. Biol. Chem. 2012, 287, 21751–21756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, C.F.; Miceli, M.C.; Baum, L.G. Clusters, Bundles, Arrays and Lattices: Novel Mechanisms for Lectin–Saccharide-Mediated Cellular Interactions. Curr. Opin. Struct. Biol. 2002, 12, 616–623. [Google Scholar] [CrossRef]
- Johannes, L.; Jacob, R.; Leffler, H. Galectins at a Glance. J. Cell Sci. 2018, 131, jcs208884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, K.; Freitag, N.; Barrientos, G.; Hartel, C.; Blois, S.M. Galectin-Levels Are Elevated in Infants Born Preterm Due to Amniotic Infection and Rapidly Decline in the Neonatal Period. Front. Immunol. 2021, 11, 3846. [Google Scholar] [CrossRef]
- El-Azzamy, H.; Balogh, A.; Romero, R.; Xu, Y.; LaJeunesse, C.; Plazyo, O.; Xu, Z.; Price, T.G.; Dong, Z.; Tarca, A.L. Characteristic Changes in Decidual Gene Expression Signature in Spontaneous Term Parturition. J. Pathol. Transl. Med. 2017, 51, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blois, S.M.; Ilarregui, J.M.; Tometten, M.; Garcia, M.; Orsal, A.S.; Cordo-Russo, R.; Toscano, M.A.; Bianco, G.A.; Kobelt, P.; Handjiski, B. A Pivotal Role for Galectin-1 in Fetomaternal Tolerance. Nat. Med. 2007, 13, 1450–1457. [Google Scholar] [CrossRef]
- Kopcow, H.D.; Rosetti, F.; Leung, Y.; Allan, D.S.J.; Kutok, J.L.; Strominger, J.L. T Cell Apoptosis at the Maternal–Fetal Interface in Early Human Pregnancy, Involvement of Galectin-1. Proc. Natl. Acad. Sci. USA 2008, 105, 18472–18477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirado-Gonzalez, I.; Freitag, N.; Barrientos, G.; Shaikly, V.; Nagaeva, O.; Strand, M.; Kjellberg, L.; Klapp, B.F.; Mincheva-Nilsson, L.; Cohen, M. Galectin-1 Influences Trophoblast Immune Evasion and Emerges as a Predictive Factor for the Outcome of Pregnancy. Mol. Hum. Reprod. 2012, 19, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitag, N.; Tirado-González, I.; Barrientos, G.; Herse, F.; Thijssen, V.L.J.L.; Weedon-Fekjær, S.M.; Schulz, H.; Wallukat, G.; Klapp, B.F.; Nevers, T. Interfering with Gal-1–Mediated Angiogenesis Contributes to the Pathogenesis of Preeclampsia. Proc. Natl. Acad. Sci. USA 2013, 110, 11451–11456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrientos, G.; Freitag, N.; Tirado-Gonzalez, I.; Unverdorben, L.; Jeschke, U.; Thijssen, V.L.J.L.; Blois, S.M. Involvement of Galectin-1 in Reproduction: Past, Present and Future. Hum. Reprod. Update 2014, 20, 175–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitag, N.; Tirado-Gonzalez, I.; Barrientos, G.; Powell, K.L.; Boehm-Sturm, P.; Koch, S.P.; Hecher, K.; Staff, A.C.; Arck, P.C.; Diemert, A. Galectin-3 Deficiency in Pregnancy Increases the Risk of Fetal Growth Restriction (FGR) via Placental Insufficiency. Cell Death Dis. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Lei, C.; Zhang, W. Expression of Galectin-3 in Mouse Endometrium and Its Effect during Embryo Implantation. Reprod. Biomed. Online 2012, 24, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Heusler, I.; Biron-Shental, T.; Farladansky-Gershnabel, S.; Pasternak, Y.; Kidron, D.; Vulih-Shuitsman, I.; Einbinder, Y.; Cohen-Hagai, K.; Benchetrit, S.; Zitman-Gal, T. Enhanced Expression of Galectin-3 in Gestational Diabetes. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Enninga, E.A.L.; Harrington, S.M.; Creedon, D.J.; Ruano, R.; Markovic, S.N.; Dong, H.; Dronca, R.S. Immune Checkpoint Molecules Soluble Program Death Ligand 1 and Galectin-9 Are Increased in Pregnancy. Am. J. Reprod. Immunol. 2018, 79, e12795. [Google Scholar] [CrossRef] [Green Version]
- Bode, L. Human Milk Oligosaccharides: Every Baby Needs a Sugar Mama. Glycobiology 2012, 22, 1147–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noll, A.J.; Gourdine, J.-P.; Yu, Y.; Lasanajak, Y.; Smith, D.F.; Cummings, R.D. Galectins Are Human Milk Glycan Receptors. Glycobiology 2016, 26, 655–669. [Google Scholar] [CrossRef]
- Coscia, A.; Orrù, S.; di Nicola, P.; Giuliani, F.; Varalda, A.; Peila, C.; Fabris, C.; Conti, A.; Bertino, E. Detection of Cow’s Milk Proteins and Minor Components in Human Milk Using Proteomics Techniques. J. Matern.-Fetal Neonatal Med. 2012, 25, 49–51. [Google Scholar] [CrossRef] [PubMed]
- García-Mantrana, I.; Alcántara, C.; Selma-Royo, M.; Boix-Amorós, A.; Dzidic, M.; Gimeno-Alcañiz, J.; Úbeda-Sansano, I.; Sorribes-Monrabal, I.; Escuriet, R.; Gil-Raga, F.; et al. MAMI: A Birth Cohort Focused on Maternal-Infant Microbiota during Early Life. BMC Pediatr. 2019, 19, 140. [Google Scholar] [CrossRef] [Green Version]
- García-Mantrana, I.; Selma-Royo, M.; González, S.; Parra-Llorca, A.; Martínez-Costa, C.; Collado, M.C. Distinct Maternal Microbiota Clusters Are Associated with Diet during Pregnancy: Impact on Neonatal Microbiota and Infant Growth during the First 18 Months of Life. Gut Microbes 2020, 11, 962–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rio-Aige, K.; Azagra-Boronat, I.; Massot-Cladera, M.; Selma-Royo, M.; Parra-Llorca, A.; González, S.; García-Mantrana, I.; Castell, M.; Rodríguez-Lagunas, M.J.; Collado, M.C.; et al. Association of Maternal Microbiota and Diet in Cord Blood Cytokine and Immunoglobulin Profiles. Int. J. Mol. Sci. 2021, 22, 1778. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Macías, E.; Selma-Royo, M.; García-Mantrana, I.; Calatayud, M.; González, S.; Martínez-Costa, C.; Collado, M.C. Maternal Diet Shapes the Breast Milk Microbiota Composition and Diversity: Impact of Mode of Delivery and Antibiotic Exposure. J. Nutr. 2020, 151, 330–340. [Google Scholar] [CrossRef]
- Azagra-Boronat, I.; Massot-Cladera, M.; Mayneris-Perxachs, J.; Knipping, K.; Van’t Land, B.; Tims, S.; Stahl, B.; Garssen, J.; Franch, A.; Castell, M.; et al. Immunomodulatory and Prebiotic Effects of 2′-Fucosyllactose in Suckling Rats. Front. Immunol. 2019, 10, 1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oksanen, J.; Simpson, G.; Blanchet, F.; Klindt, R.; Legendre, P.; Minchin, P.; O’Hara, R.; Solymos, P.; Stevens, M.; Szoecs, E.; et al. Vegan: Community Ecology Package. R Package Version 2.6–2. 2022. Available online: https://cran.r-project.org/web/packages/vegan/index.html (accessed on 20 April 2022).
- Kalagiri, R.R.; Carder, T.; Choudhury, S.; Vora, N.; Ballard, A.R.; Govande, V.; Drever, N.; Beeram, M.R.; Uddin, M.N. Inflammation in Complicated Pregnancy and Its Outcome. Am. J. Perinatol. 2016, 33, 1337–1356. [Google Scholar] [CrossRef] [PubMed]
- Yockey, L.J.; Iwasaki, A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity 2018, 49, 397–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brubel, R.; Bokor, A.; Pohl, A.; Schilli, G.K.; Szereday, L.; Bacher-Szamuel, R.; Rigo, J., Jr.; Polgar, B. Serum Galectin-9 as a Noninvasive Biomarker for the Detection of Endometriosis and Pelvic Pain or Infertility-Related Gynecologic Disorders. Fertil. Steril. 2017, 108, 1016–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farladansky-Gershnabel, S.; Heusler, I.; Biron-Shental, T.; Shechter-Maor, G.; Amiel, A.; Kidron, D.; Weisz, A.; Einbinder, Y.; Cohen-Hagai, K.; Benchetrit, S.; et al. Elevated Expression of Galectin-3, Thioredoxin and Thioredoxin Interacting Protein in Preeclampsia. Pregnancy Hypertens. 2021, 26, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Jennewein, M.F.; Goldfarb, I.; Dolatshahi, S.; Cosgrove, C.; Noelette, F.J.; Krykbaeva, M.; Das, J.; Sarkar, A.; Gorman, M.J.; Fischinger, S.; et al. Fc Glycan-Mediated Regulation of Placental Antibody Transfer. Cell 2019, 178, 202–215.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purizaca-benites, M. La Placenta y La Barrera Placentaria. Revista Peruana de Ginecología y Obstetricia 2008, 54, 270–278. [Google Scholar] [CrossRef]
- Miyauchi, M.; Ao, M.; Furusho, H.; Chea, C.; Nagasaki, A.; Sakamoto, S.; Ando, T.; Inubushi, T.; Kozai, K.; Takata, T. Galectin-3 Plays an Important Role in Preterm Birth Caused by Dental Infection of Porphyromonas Gingivalis. Sci. Rep. 2018, 8, 2867. [Google Scholar] [CrossRef] [Green Version]
- He, X.W.; Li, W.L.; Li, C.; Liu, P.; Shen, Y.G.; Zhu, M.; Jin, X.P. Serum Levels of Galectin-1, Galectin-3, and Galectin-9 Are Associated with Large Artery Atherosclerotic Stroke. Sci. Rep. 2017, 7, 40994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linden, J.R.; de Paepe, M.E.; Laforce-Nesbitt, S.S.; Bliss, J.M. Galectin-3 Plays an Important Role in Protection against Disseminated Candidiasis. Med. Mycol. 2013, 51, 641–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.-H.; Zhou, W.-H.; Tao, Y.; Wang, S.-C.; Jiang, Y.-L.; Zhang, D.; Piao, H.-L.; Fu, Q.; Li, D.-J.; Du, M.-R. The Galectin-9/Tim-3 Pathway Is Involved in the Regulation of NK Cell Function at the Maternal–Fetal Interface in Early Pregnancy. Cell. Mol. Immunol. 2016, 13, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Meggyes, M.; Miko, E.; Polgar, B.; Bogar, B.; Farkas, B.; Illes, Z.; Szereday, L. Peripheral Blood TIM-3 Positive NK and CD8+ T Cells throughout Pregnancy: TIM-3/Galectin-9 Interaction and Its Possible Role during Pregnancy. PLoS ONE 2014, 9, e92371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molinari, C.E.; Casadio, Y.S.; Hartmann, B.T.; Livk, A.; Bringans, S.; Arthur, P.G.; Hartmann, P.E. Proteome Mapping of Human Skim Milk Proteins in Term and Preterm Milk. J. Proteome Res. 2012, 11, 1696–1714. [Google Scholar] [CrossRef]
- Trégoat, V.; Montagne, P.; Béné, M.C.; Faure, G. Increases of Iga Milk Concentrations Correlate with IgA2 Increment. J. Clin. Lab. Anal. 2001, 15, 55–58. [Google Scholar] [CrossRef]
- Castellote, C.; Casillas, R.; Ramírez-Santana, C.; Pérez-Cano, F.J.; Castell, M.; Moretones, M.G.; López-Sabater, M.C.; Franch, À. Premature Delivery Influences the Immunological Composition of Colostrum and Transitional and Mature Human Milk. J. Nutr. 2011, 141, 1181–1187. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Karmaus, W.; Davis, S.; Gangur, V. Immune Markers in Breast Milk and Fetal and Maternal Body Fluids: A Systematic Review of Perinatal Concentrations. J. Hum. Lact. 2011, 27, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Rio-aige, K.; Azagra-boronat, I.; Castell, M.; Selma-royo, M.; Rodr, J.; Francisco, J.P. The Breast Milk Immunoglobulinome. Nutrients 2021, 13, 1810. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, Z.; Ming, D.; Huang, C.; Xu, S.; Li, Z.; Wang, Z.; Liu, H.; Zeng, X.; Wang, F. Effect of Maternal Dietary Starch-to-Fat Ratio and Daily Energy Intake during Late Pregnancy on the Performance and Lipid Metabolism of Primiparous Sows and Newborn Piglets. J. Anim. Sci. 2022, 100, skac033. [Google Scholar] [CrossRef] [PubMed]
- Haisan, J.; Inabu, Y.; Shi, W.; Oba, M. Effects of Pre- and Postpartum Dietary Starch Content on Productivity, Plasma Energy Metabolites, and Serum Inflammation Indicators of Dairy Cows. J. Dairy Sci. 2021, 104, 4362–4374. [Google Scholar] [CrossRef]
- Kaur, G.; Guo, X.F.; Sinclair, A.J. Short Update on Docosapentaenoic Acid: A Bioactive Long-Chain n-3 Fatty Acid. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 88–91. [Google Scholar] [CrossRef]
- Bernardi, J.R.; Escobar, R.D.S.; Ferreira, C.F.; Silveira, P.P. Fetal and Neonatal Levels of Omega-3: Effects on Neurodevelopment, Nutrition, and Growth. Sci. World J. 2012, 2012, 202473. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; Demmelmair, H.; Grote, V.; Totzauer, M. Optimized Protein Intakes in Term Infants Support Physiological Growth and Promote Long-Term Health. Semin. Perinatol. 2019, 43, 151153. [Google Scholar] [CrossRef]
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; van Tol, E.A.F.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast Milk Nutrient Content and Infancy Growth. Acta Paediatr. Int. J. Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.L.; Yang, F.; Xiong, F. Association of Leptin, Adiponectin, and Ghrelin in Breast Milk with the Growth of Infants with Exclusive Breastfeeding. Chin. J. Contemp. Pediatrics 2018, 20, 91–96. [Google Scholar] [CrossRef]
- Prentice, P.M.; Schoemaker, M.H.; Vervoort, J.; Hettinga, K.; Lambers, T.T.; van Tol, E.A.F.; Acerini, C.L.; Olga, L.; Petry, C.J.; Hughes, I.A.; et al. Human Milk Short-Chain Fatty Acid Composition Is Associated with Adiposity Outcomes in Infants. J. Nutr. 2019, 149, 716–722. [Google Scholar] [CrossRef]
- Dzidic, M.; Boix-Amorós, A.; Selma-Royo, M.; Mira, A.; Collado, M. Gut Microbiota and Mucosal Immunity in the Neonate. Med. Sci. 2018, 6, 56. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics | n = 15 |
|---|---|
| Pre-gestational BMI (kg/m2), mean ± SEM | 24.36 ± 1.21 |
| Pregnancy weight gain (kg), mean ± SEM | 11.29 ± 1.09 |
| Antibiotic during pregnancy, yes (%) | 4 (26.67) |
| Intrapartum antibiotic, yes (%) | 10 (66.67) |
| Gestational age (weeks), mean ± SEM | 38.2 ± 0.30 |
| Mode of delivery: vaginal birth, yes (%) | 5 (33.33) |
| First time mothers, yes (%) | 8 (53.3) |
| Gestational diabetes mellitus (GDM), yes (%) | 2 (13.33) |
| Infant Characteristics | n = 15 |
| Gender: Female, yes (%) | 5 (33.33) |
| Body weight gain from birth to the 1st month (mg/day) | 32.11 ± 2.57 |
| Birth WFL z score, mean ± SEM | −0.29 ± 0.28 |
| Weight (kg), mean ± SEM | |
| Birth | 3.06 ± 0.11 |
| 1st month | 4.03 ± 0.15 |
| 6th month | 7.68 ± 0.15 |
| 12th month | 9.56 ± 0.23 |
| BMI z score, mean ± SEM | |
| Birth | −0.5 ± 0.27 |
| 1st month | −0.70 ± 0.34 |
| 6th month | −0.35 ± 0.19 |
| 12th month | 0.13 ± 0.23 |
| Female | Male | p | |
|---|---|---|---|
| MP | n = 5 | n = 10 | |
| Gal-1 (ng/mL) | 16.10 ± 5.28 | 29.53 ± 7.32 | 0.327 |
| Gal-3 (ng/mL) | 11.47 ± 3.43 | 18.22 ± 3.95 | 0.426 |
| Gal-9 (pg/mL) | 350 ± 26 | 475 ± 32 | 0.020 * |
| UCP | n = 5 | n = 9 | |
| Gal-1 (ng/mL) | 20.69 ± 4.16 | 24.32 ± 3.41 | 0.317 |
| Gal-3 (ng/mL) | 16.94 ± 7.75 | 17.51 ± 7.03 | 0.789 |
| Gal-9 (pg/mL) | 263 ± 89 | 296 ± 20 | 0.205 |
| Maternal Characteristics | n = 23 |
|---|---|
| Pre-gestational BMI (Kg/m2), mean ± SEM | 22.72 ± 0.92 |
| Pregnancy weight gain (Kg), mean ± SEM | 11.94 ± 1.13 |
| Antibiotic during pregnancy, yes (%) | 8 (34.78) |
| Intrapartum antibiotic, yes (%) | 10 (43.48) |
| Perinatal antibiotic, yes (%) | 14 (60.87) |
| Gestational age (weeks), mean ± SEM | 39.29 ± 0.27 |
| Mode of delivery: vaginal birth, yes (%) | 15 (65.22) |
| First time mothers, yes (%) | 10 (43.48) |
| Gestational diabetes mellitus (GDM), yes (%) | 2 (8.69) |
| Infant Characteristics | n = 23 |
| Gender: Female, yes (%) | 12 (52.17) |
| Body weight gain from birth to the 1st month (mg/day) | 25.33 ± 1.97 |
| Birth WFL z score, mean ± SEM | −0.20 ± 0.19 |
| Weight (kg), mean ± SEM | |
| Birth | 3.18 ± 0.11 |
| 7th day | 3.17 ± 0.09 |
| 15th day | 3.40 ± 0.08 |
| 1st month | 3.98 ± 0.11 |
| 6th month | 7.41 ± 0.19 |
| 12th month | 9.47 ± 0.25 |
| BMI z score at birth, mean ± SEM | |
| Birth | −0.29 ± 0.20 |
| 7th day | −0.55 ± 0.22 |
| 15th day | −0.55 ± 0.19 |
| 1st month | −0.71 ± 0.21 |
| 6th month | −0.08 ± 0.16 |
| 12th month | 0.39 ± 0.20 |
| d7, n = 23 | d15, n = 23 | p | |
|---|---|---|---|
| Gal-1 (ng/mL) | 14.88 ± 3.86 | 14.22 ± 4.98 | 0.253 |
| Gal-3 (ng/mL) | 54.25 ± 12.43 | 66.05 ± 15.19 | 0.869 |
| Gal-9 (pg/mL) | 149.41 ± 29.61 | 182.73 ± 39.89 | 0.645 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rio-Aige, K.; Girbal, M.; Selma-Royo, M.; Parra-Llorca, A.; González, S.; Martínez-Costa, C.; Castell, M.; Collado, M.C.; Pérez-Cano, F.J.; Rodríguez-Lagunas, M.J. Galectins-1, -3 and -9 Are Present in Breast Milk and Have a Role in Early Life Development. Nutrients 2022, 14, 4338. https://doi.org/10.3390/nu14204338
Rio-Aige K, Girbal M, Selma-Royo M, Parra-Llorca A, González S, Martínez-Costa C, Castell M, Collado MC, Pérez-Cano FJ, Rodríguez-Lagunas MJ. Galectins-1, -3 and -9 Are Present in Breast Milk and Have a Role in Early Life Development. Nutrients. 2022; 14(20):4338. https://doi.org/10.3390/nu14204338
Chicago/Turabian StyleRio-Aige, Karla, Marina Girbal, Marta Selma-Royo, Anna Parra-Llorca, Sonia González, Cecilia Martínez-Costa, Margarida Castell, María Carmen Collado, Francisco J. Pérez-Cano, and María J. Rodríguez-Lagunas. 2022. "Galectins-1, -3 and -9 Are Present in Breast Milk and Have a Role in Early Life Development" Nutrients 14, no. 20: 4338. https://doi.org/10.3390/nu14204338
APA StyleRio-Aige, K., Girbal, M., Selma-Royo, M., Parra-Llorca, A., González, S., Martínez-Costa, C., Castell, M., Collado, M. C., Pérez-Cano, F. J., & Rodríguez-Lagunas, M. J. (2022). Galectins-1, -3 and -9 Are Present in Breast Milk and Have a Role in Early Life Development. Nutrients, 14(20), 4338. https://doi.org/10.3390/nu14204338