

From Restriction to Intuition: Evaluating Intuitive Eating in a Sample of the General Population

 , , and
, , and
Abstract
:1. Introduction
- To make comparisons between ‘dieters’ and ‘non-dieters’ for the above-mentioned clinical variables that may be related to dieting—BMI, eating psychopathology, self-efficacy, and quality of life.
- Investigate possible correlations between IE and the same clinical variables in the two groups (‘dieters’ and ‘non-dieters’).
- Examine whether IE, BMI, eating psychopathology, self-efficacy, and quality of life can predict engagement in weight-loss dietary approaches.
2. Materials and Methods
2.1. Measures
- -
- Dieting history:
- -
- Intuitive Eating Scale-2 (IES-2):
- -
- Eating Disorder Examination Questionnaire (EDE-Q):
- -
- General Self-Efficacy Scale (GSE):
- -
- 12-Item Short-Form Health Survey (SF-12):
2.2. Statistical Analysis
3. Results
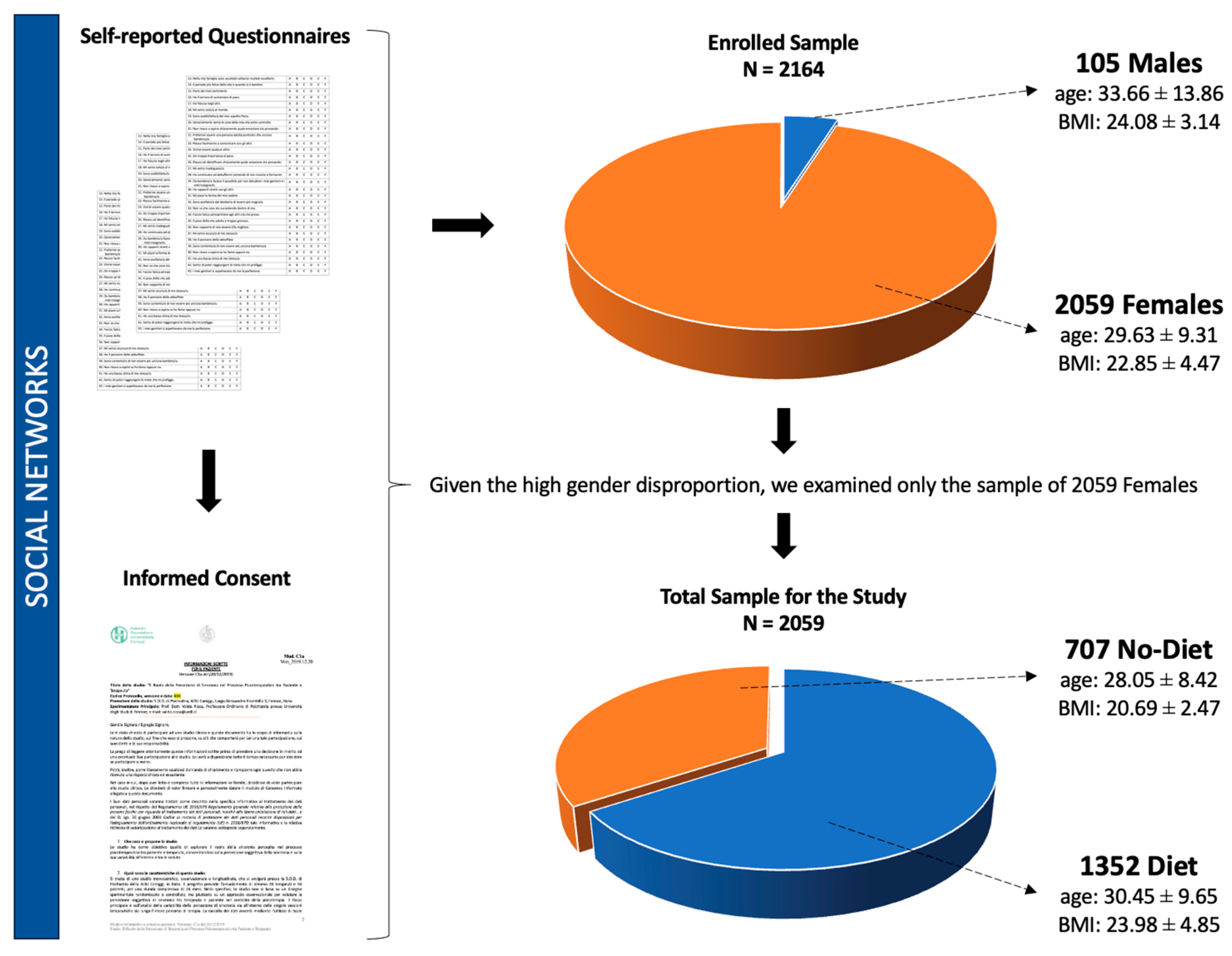
3.1. Descriptive Analysis of the Total Sample
3.2. Comparisons between “Diet” and “No Diet” Groups
3.3. Correlation Analyses within “Diet” and “No Diet” Groups
3.4. Logistic Regression Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, G.T. The controversy over dieting. In Eating Disorders and Obesity: A Comprehensive Handbook, 2nd ed.; Fairburn, C.G., Brownell, K.D., Eds.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Wadden, T.A.; Foster, G.D.; Sarwer, D.B.; Anderson, D.A.; Gladis, M.; Sanderson, R.S.; Letchak, R.; I Berkowitz, R.; Phelan, S. Dieting and the development of eating disorders in obese women: Results of a randomized controlled trial. Am. J. Clin. Nutr. 2004, 80, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Avenell, A.; Bolland, M.; Hudson, J.; Stewart, F.; Robertson, C.; Sharma, P.; Fraser, C.; MacLennan, G. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: Systematic review and meta-analysis. BMJ 2017, 359, j4849. [Google Scholar] [CrossRef] [PubMed]
- Stewart, T.M.; Martin, C.K.; Williamson, D.A. The Complicated Relationship between Dieting, Dietary Restraint, Caloric Restriction, and Eating Disorders: Is a Shift in Public Health Messaging Warranted? Int. J. Environ. Res. Public Health 2022, 19, 491. [Google Scholar] [CrossRef]
- Stice, E.; Presnell, K. Dieting and the eating disorders. In The Oxford Handbook of Eating Disorders; Agras, W.S., Ed.; Oxford University Press: Oxford, UK, 2010; pp. 148–179. [Google Scholar]
- Mann, T.; Tomiyama, A.J.; Westling, E.; Lew, A.M.; Samuels, B.; Chatman, J. Medicare’s search for effective obesity treatments: Diets are not the answer. Am. Psychol. 2007, 62, 220–233. [Google Scholar] [CrossRef]
- Bacon, L.; Aphramor, L. Weight science: Evaluating the evidence for a paradigm shift. Nutr. J. 2011, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and unhealthy weight control behaviors during adolescence: Associations with 10-year changes in body mass index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, K.; Anderson, D. Dietary restraint and weight loss as risk factors for eating pathology. Eat. Behav. 2016, 23, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.R.; Witt, A.A.; Grossman, S.L. Dieting in bulimia nervosa is associated with increased food restriction and psychopathology but decreased binge eating. Eat. Behav. 2013, 14, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Burton, E.; Lowe, M.; Butryn, M.; McDermott, B. Relation of dieting to eating pathology. In Eating Disorders in Children and Adolescents; Jaffa, T., Ed.; Cambridge University Press: Cambridge, UK, 2006; pp. 45–56. [Google Scholar]
- Fontaine, K.R.; Cheskin, L.J. Self-efficacy, attendance, and weight loss in obesity treatment. Addict. Behav. 1997, 22, 567–570. [Google Scholar] [CrossRef]
- Jeffery, R.W.; Bjornson-Benson, W.M.; Rosenthal, B.S.; Lindquist, R.A.; Kurth, C.L.; Johnson, S.L. Correlates of weight loss and its maintenance over two years of follow-up among middle-aged men. Prev. Med. 1984, 13, 155–168. [Google Scholar] [CrossRef]
- Linde, J.A.; Jeffery, R.W.; Levy, R.L.; Sherwood, N.E.; Utter, J.; Pronk, N.P.; Boyle, R.G. Binge eating disorder, weight control self-efficacy, and depression in overweight men and women. Int. J. Obes. 2004, 28, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.D.; Dutton, G.R.; Brantley, P.J. Self-efficacy as a predictor of weight change in African-American women. Obes. Res. 2004, 12, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Going, S.B.; Houtkooper, L.B.; Cussler, E.C.; Martin, C.J.; Metcalfe, L.L.; Finkenthal, N.R.; Blew, R.M.; Sardinha, L.B.; Lohman, T.G. Weight loss readiness in middle-aged women: Psychosocial predictors of success for behavioral weight reduction. J. Behav. Med. 2002, 25, 499–523. [Google Scholar] [CrossRef]
- Wamsteker, E.W.; Geenen, R.; Iestra, J.; Larsen, J.K.; Zelissen, P.M.; van Staveren, W.A. Obesity-related beliefs predict weight loss after an 8-week low-calorie diet. J. Am. Diet. Assoc. 2005, 105, 441–444. [Google Scholar] [CrossRef]
- Nezami, B.T.; Lang, W.; Jakicic, J.M.; Davis, K.K.; Polzien, K.; Rickman, A.D.; Hatley, K.E.; Tate, D.F. The Effect of Self-Efficacy on Behavior and Weight in a Behavioral Weight-Loss Intervention. Health Psychol. 2016, 35, 714. [Google Scholar] [CrossRef] [PubMed]
- Tribole, E.; Resch, E. Intuitive Eating: A Revolutionary Program That Works; Saint Martin’s Paperbacks: New York, NY, USA, 1995. [Google Scholar]
- Tribole, E.; Resch, E. Intuitive Eating: A Revolutionary Program That Works, 3rd ed.; Saint Martin’s Paperbacks: New York, NY, USA, 2012. [Google Scholar]
- Tylka, T.L. Development and psychometric evaluation of a measure of intuitive eating. J. Couns. Psychol. 2006, 53, 226–240. [Google Scholar] [CrossRef]
- Tylka, T.L.; Kroon Van Diest, A.M. The Intuitive Eating Scale-2: Item refinement and psychometric evaluation with college women and men. J. Couns. Psychol. 2013, 60, 137–153. [Google Scholar] [CrossRef]
- Smith, T.S.; Hawks, S.R. Intuitive Eating, Diet Composition, and The Meaning of Food in Healthy Weight Promotion. Am. J. Health Educ. 2006, 37, 130–136. [Google Scholar] [CrossRef]
- Bruce, L.J.; Ricciardelli, L.A. A systematic review of the psychosocial correlates of intuitive eating among adult women. Appetite 2016, 96, 454–472. [Google Scholar] [CrossRef]
- Hazzard, V.M.; Telke, S.E.; Simone, M.; Anderson, L.M.; Larson, N.I.; Neumark-Sztainer, D. Intuitive eating longitudinally predicts better psychological health and lower use of disordered eating behaviors: Findings from EAT 2010–2018. Eat. Weight Disord. 2021, 26, 287–294. [Google Scholar] [CrossRef]
- Van Dyke, N.; Drinkwater, E.J. Relationships between intuitive eating and health indicators: Literature review. Public Health Nutr. 2014, 17, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J. Positive body image, intuitive eating, and self-compassion protect against the onset of the core symptoms of eating disorders: A prospective study. Int. J. Eat. Disord. 2021, 54, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Christoph, M.; Järvelä-Reijonen, E.; Hooper, L.; Larson, N.; Mason, S.M.; Neumark-Sztainer, D. Longitudinal associations between intuitive eating and weight-related behaviors in a population-based sample of young adults. Appetite 2021, 160, 105093. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.T.; Magnuson, A.B. A review of interventions that promote eating by internal cues. J. Acad. Nutr. Diet. 2014, 114, 734–760. [Google Scholar] [CrossRef] [PubMed]
- Swami, V.; Maïano, C.; Todd, J.; Ghisi, M.; Cardi, V.; Bottesi, G.; Cerea, S. Dimensionality and psychometric properties of an Italian translation of the Intuitive Eating Scale-2 (IES-2): An assessment using a bifactor exploratory structural equation modelling framework. Appetite 2021, 166, 105588. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; Milanese, C.; Sartirana, M.; El Ghoch, M.; Sartori, F.; Geccherle, E.; Coppini, A.; Franchini, C.; Grave, R.D. The Eating Disorder Examination Questionnaire: Reliability and validity of the Italian version. Eat. Weight. Disord. 2017, 22, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Sibilia, L.; Schwarzer, R.; Jerusalem, M. Italian Adaptation of the General Self-Efficacy Scale. Resource Document. Ralf Schwarzer Web Site. 1995. Available online: http://userpage.fu-berlin.de/~health/italian.htm (accessed on 25 January 2012).
- Kodraliu, G.; Mosconi, P.; Groth, N.; Carmosino, G.; Perilli, A.; Gianicolo, E.A.; Rossi, C.; Apolone, G. Subjective health status assessment: Evaluation of the Italian version of the SF-12 Health Survey. Results from the MiOS Project. J. Epidemiol. Biostat. 2001, 6, 305–316. [Google Scholar] [CrossRef] [PubMed]
- JASP, Version 0.18.3. Computer software. JASP Team: Mound, TX, USA, 2024.
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Field, A.E.; Aneja, P.; Austin, S.B.; Shrier, L.A.; de Moor, C.; Gordon-Larsen, P. Race and gender differences in the association of dieting and gains in BMI among young adults. Obesity 2007, 15, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Sares-Jäske, L.; Knekt, P.; Männistö, S.; Lindfors, O.; Heliövaara, M. Self-report dieting and long-term changes in body mass index and waist circumference. Obes. Sci. Pract. 2019, 5, 291–303. [Google Scholar] [CrossRef]
- Timmerman, G.M.; Gregg, E.K. Dieting, perceived deprivation, and preoccupation with food. West. J. Nurs. Res. 2003, 25, 405–418. [Google Scholar] [CrossRef]
- Carson, T.L.; Hidalgo, B.; Ard, J.D.; Affuso, O. Dietary interventions and quality of life: A systematic review of the literature. J. Nutr. Educ. Behav. 2014, 46, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraça, E.V.; Marques, M.M.; Rutter, H.; Oppert, J.M.; De Bourdeaudhuij, I.; Lakerveld, J.; Brug, J. Successful behavior change in obesity interventions in adults: A systematic review of self-regulation mediators. BMC Med. 2015, 13, 84. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J.; Tylka, T.L.; Fuller-Tyszkiewicz, M. Intuitive eating and its psychological correlates: A meta-analysis. Int. J. Eat. Disord. 2021, 54, 1073–1098. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Blechert, J.; Hautzinger, M.; Matthias, E.; Herbert, C. Intuitive eating is associated with interoceptive sensitivity. Effects on body mass index. Appetite 2013, 70, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Kurz, A.L.; Albrecht, J.; Schreder, T.; Kleemann, A.M.; Schöpf, V.; Kopietz, R.; Wiesmann, M.; Schandry, R. Reduced perception of bodily signals in anorexia nervosa. Eat. Behav. 2008, 9, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Herbert, B.M.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Tsakiris, M. Atypical self-focus effect on interoceptive accuracy in anorexia nervosa. Front. Hum. Neurosci. 2016, 10, 484. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Pollatos, O. Attenuated interoceptive sensitivity in overweight and obese individuals. Eat. Behav. 2014, 15, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Herbert, B.M.; Pollatos, O. The relevance of interoception for eating behavior and eating disorders. In The Interoceptive Mind: From Homeostasis to Awareness; Tsakiris, M., De Preester, H., Eds.; Oxford University Press: Oxford, UK, 2019; pp. 165–186. [Google Scholar]
- Hensley-Hackett, K.; Bosker, J.; Keefe, A.; Reidlinger, D.; Warner, M.; D’arcy, A.; Utter, J. Intuitive Eating Intervention and Diet Quality in Adults: A Systematic Literature Review. J. Nutr. Educ. Behav. 2022, 54, 1099–1115. [Google Scholar] [CrossRef] [PubMed]
- Warren, J.M.; Smith, N.; Ashwell, M. A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviors: Effectiveness and associated potential mechanisms. Nutr. Res. Rev. 2017, 30, 272–283. [Google Scholar] [CrossRef]
- Stice, E.; Shaw, H.E. Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. J. Psychosom. Res. 2002, 53, 985–993. [Google Scholar] [CrossRef]
- Stice, E. Risk and maintenance factors for eating pathology: A meta-analytic review. Psychol. Bull. 2002, 128, 825–848. [Google Scholar] [CrossRef] [PubMed]
- Sutin, A.R.; Terracciano, A. Body weight misperception in adolescence and incident obesity in young adulthood. Psychol. Sci. 2015, 26, 507–511. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No Diet (n = 707) | Diet (n = 1352) | t | Cohen’s d | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Age (years) | 28.05 | 8.42 | 30.45 | 9.65 | −5.60 ** | −0.26 |
| BMI (kg/m2) | 20.69 | 2.47 | 23.98 | 4.85 | −16.89 ** | −0.79 |
| IES-2 | 3.69 | 0.61 | 3.21 | 0.67 | 15.79 ** | 0.73 |
| EDE-Q | 0.85 | 0.89 | 1.81 | 1.20 | −18.61 ** | −0.86 |
| SF-12 | 33.93 | 5.79 | 32.49 | 6.13 | 5.14 ** | 0.24 |
| GSE | 2.98 | 0.49 | 2.93 | 0.51 | 2.00 * | 0.10 |
| Diet | |||||
| 1 | 2 | 3 | 4 | 5 | |
| 1. IES-2 | - | ||||
| 2. BMI (kg/m2) | −0.27 ** | - | |||
| 3. EDE-Q | −0.65 ** | 0.23 ** | - | ||
| 4. SF-12 | 0.42 ** | −0.18 ** | −0.52 ** | - | |
| 5. GSE | 0.33 ** | −0.02 | −0.30 ** | 0.46 ** | - |
| No Diet | |||||
| 1 | 2 | 3 | 4 | 5 | |
| 1. IES-2 | - | ||||
| 2. BMI (kg/m2) | −0.26 ** | - | |||
| 3. EDE-Q | −0.19 ** | 0.27 * | - | ||
| 4. SF-12 | 0.15 | −0.10 | −0.51 ** | - | |
| 5. GSE | 0.08 | −0.03 | −0.24 | 0.47 ** | - |
| Predictor | B | SE | OR | Z | Wald | p |
|---|---|---|---|---|---|---|
| Intercept | −6.49 | 0.74 | 0.01 | −8.71 | 75.94 | <0.001 |
| IES-2 | −0.25 | 0.11 | 0.78 | −2.29 | 5.24 | 0.022 |
| EDE-Q | 0.80 | 0.08 | 2.22 | 10.10 | 102.06 | <0.001 |
| BMI (kg/m2) | 0.23 | 0.02 | 1.26 | 10.79 | 116.50 | <0.001 |
| SF-12 | 0.04 | 0.01 | 1.04 | 3.10 | 9.64 | 0.002 |
| Age | 0.02 | 0.01 | 1.02 | 2.34 | 5.47 | 0.019 |
| GSE | 0.09 | 0.12 | 1.10 | 0.75 | 0.57 | 0.450 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucherini Angeletti, L.; Spinelli, M.C.; Cassioli, E.; Rossi, E.; Castellini, G.; Brogioni, G.; Ricca, V.; Rotella, F. From Restriction to Intuition: Evaluating Intuitive Eating in a Sample of the General Population. Nutrients 2024, 16, 1240. https://doi.org/10.3390/nu16081240
Lucherini Angeletti L, Spinelli MC, Cassioli E, Rossi E, Castellini G, Brogioni G, Ricca V, Rotella F. From Restriction to Intuition: Evaluating Intuitive Eating in a Sample of the General Population. Nutrients. 2024; 16(8):1240. https://doi.org/10.3390/nu16081240
Chicago/Turabian StyleLucherini Angeletti, Lorenzo, Maria Chiara Spinelli, Emanuele Cassioli, Eleonora Rossi, Giovanni Castellini, Giulietta Brogioni, Valdo Ricca, and Francesco Rotella. 2024. "From Restriction to Intuition: Evaluating Intuitive Eating in a Sample of the General Population" Nutrients 16, no. 8: 1240. https://doi.org/10.3390/nu16081240