The Mediterranean Diet and Nutritional Adequacy: A Review


Abstract
:1. Introduction
2. Methods
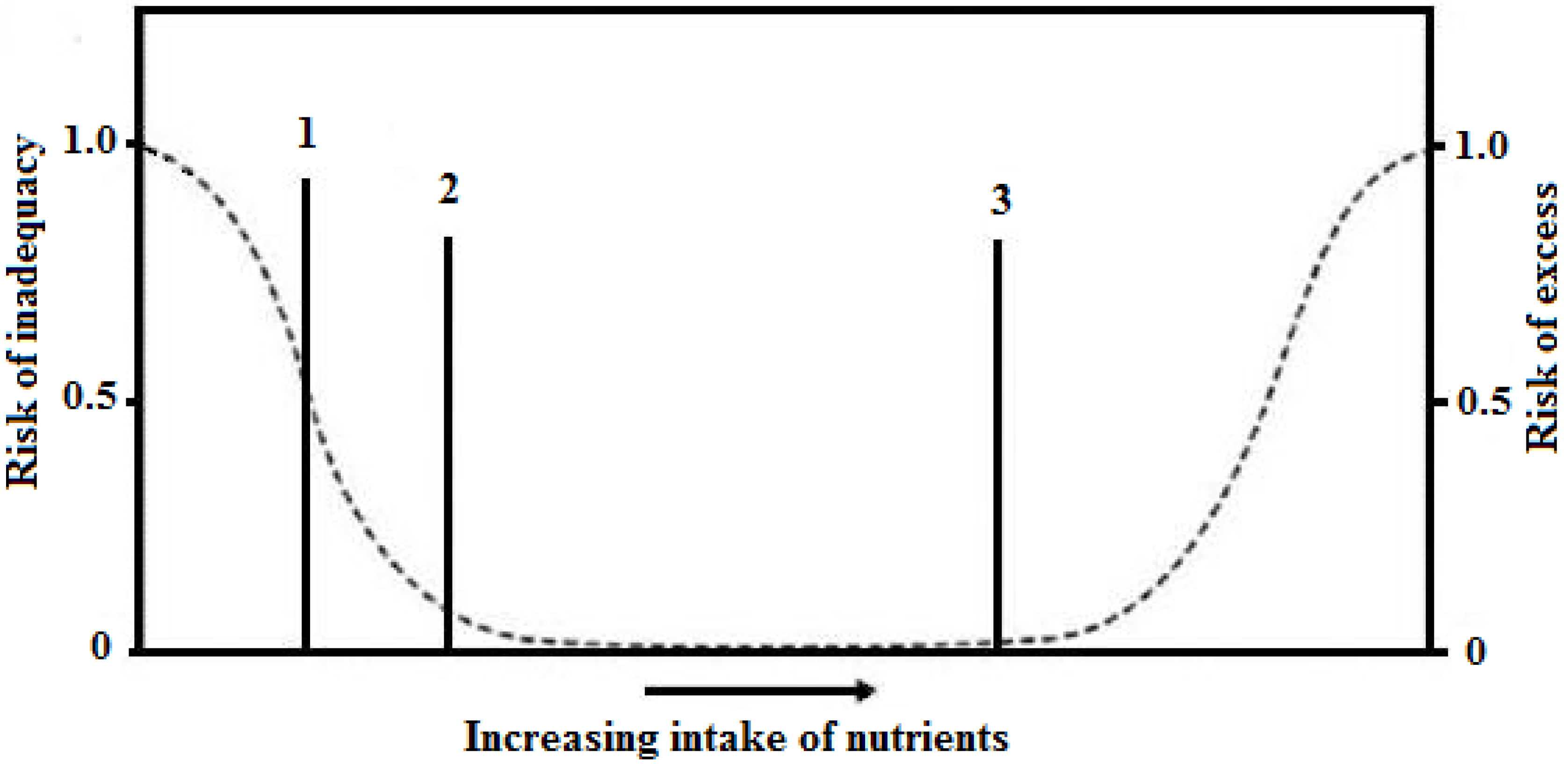
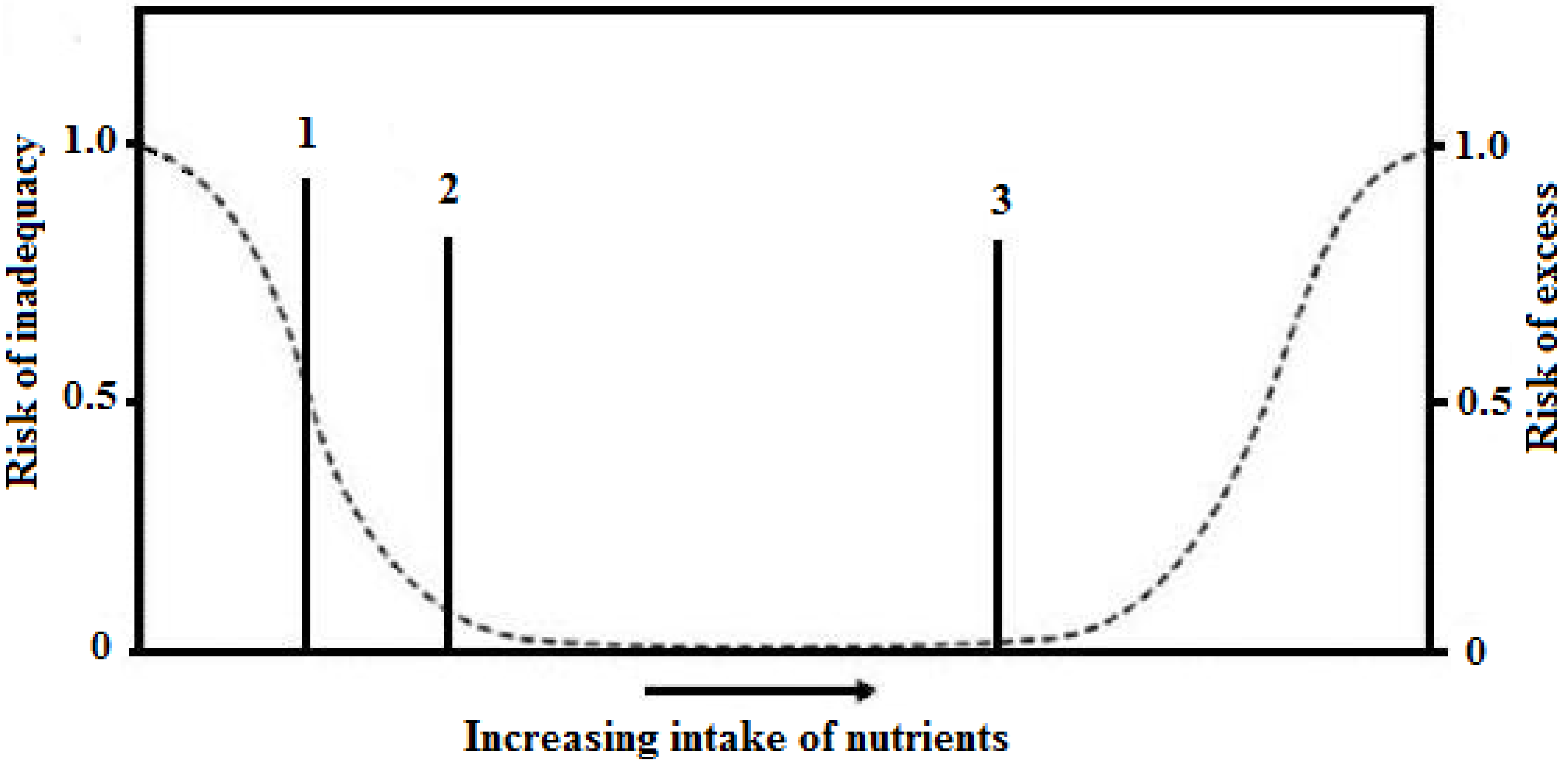
Nutritional Adequacy Assessment
3. Results
3.1. Prevalence of Nutritional Adequacy in Europe and Some Mediterranean Countries
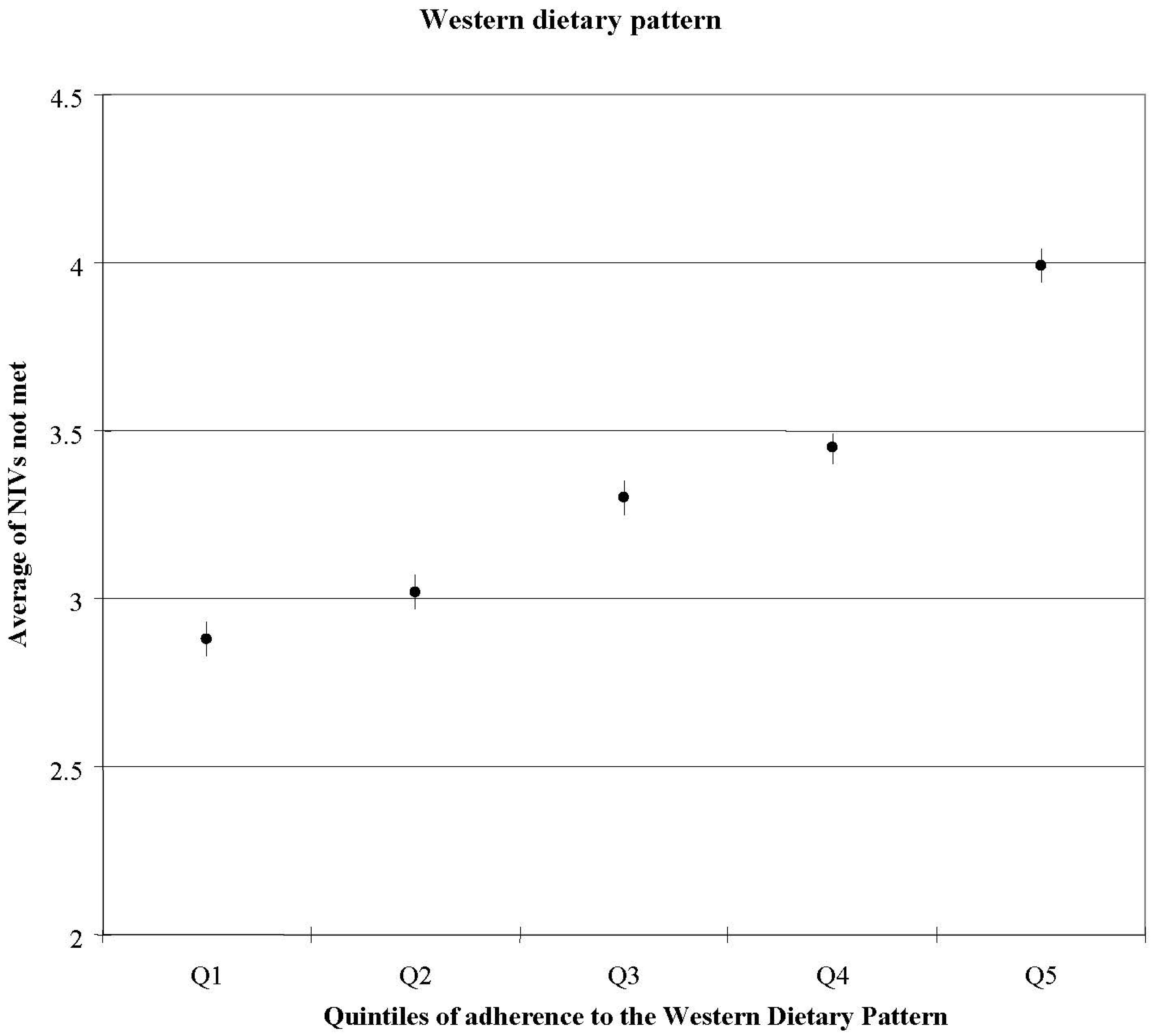
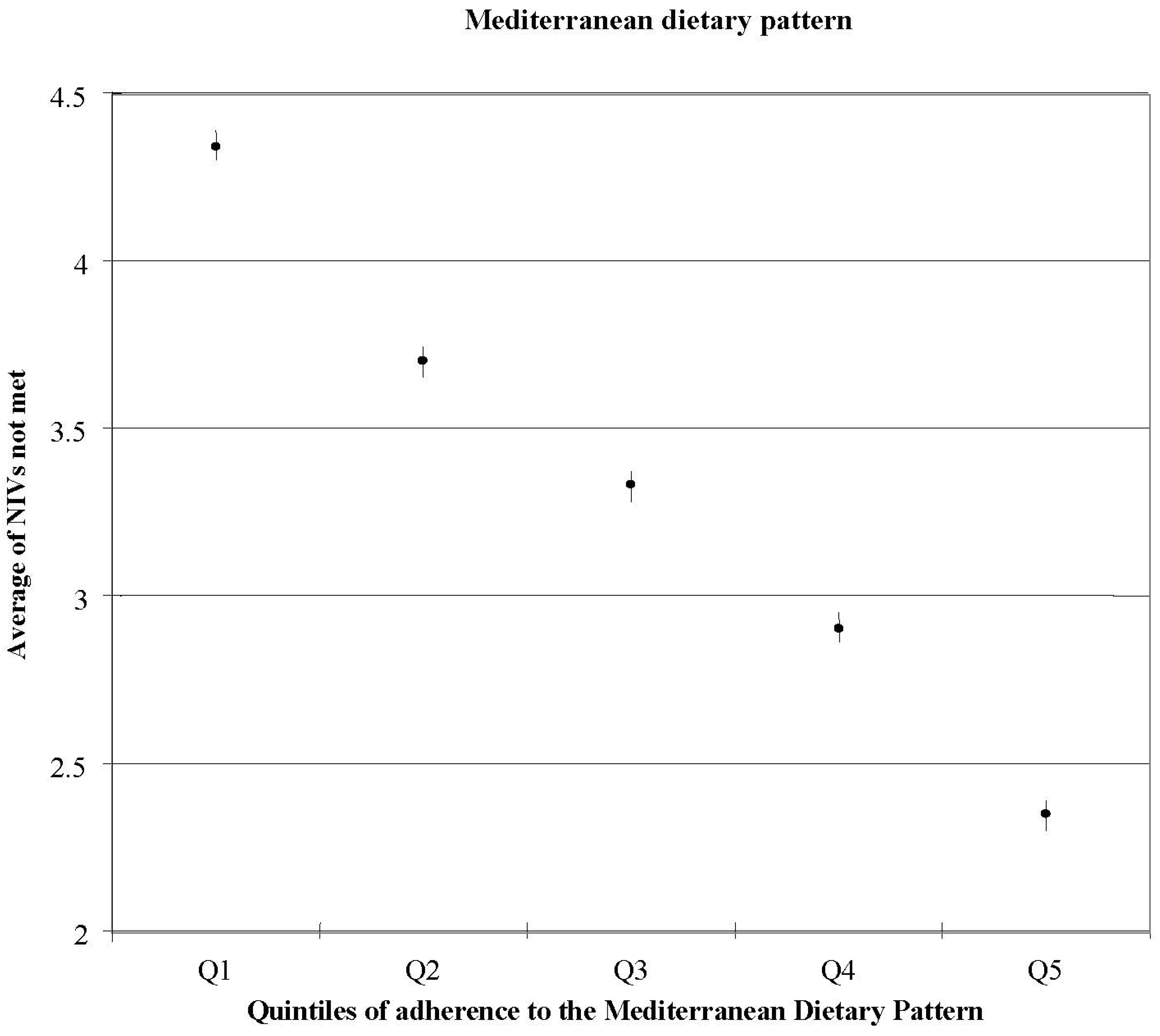
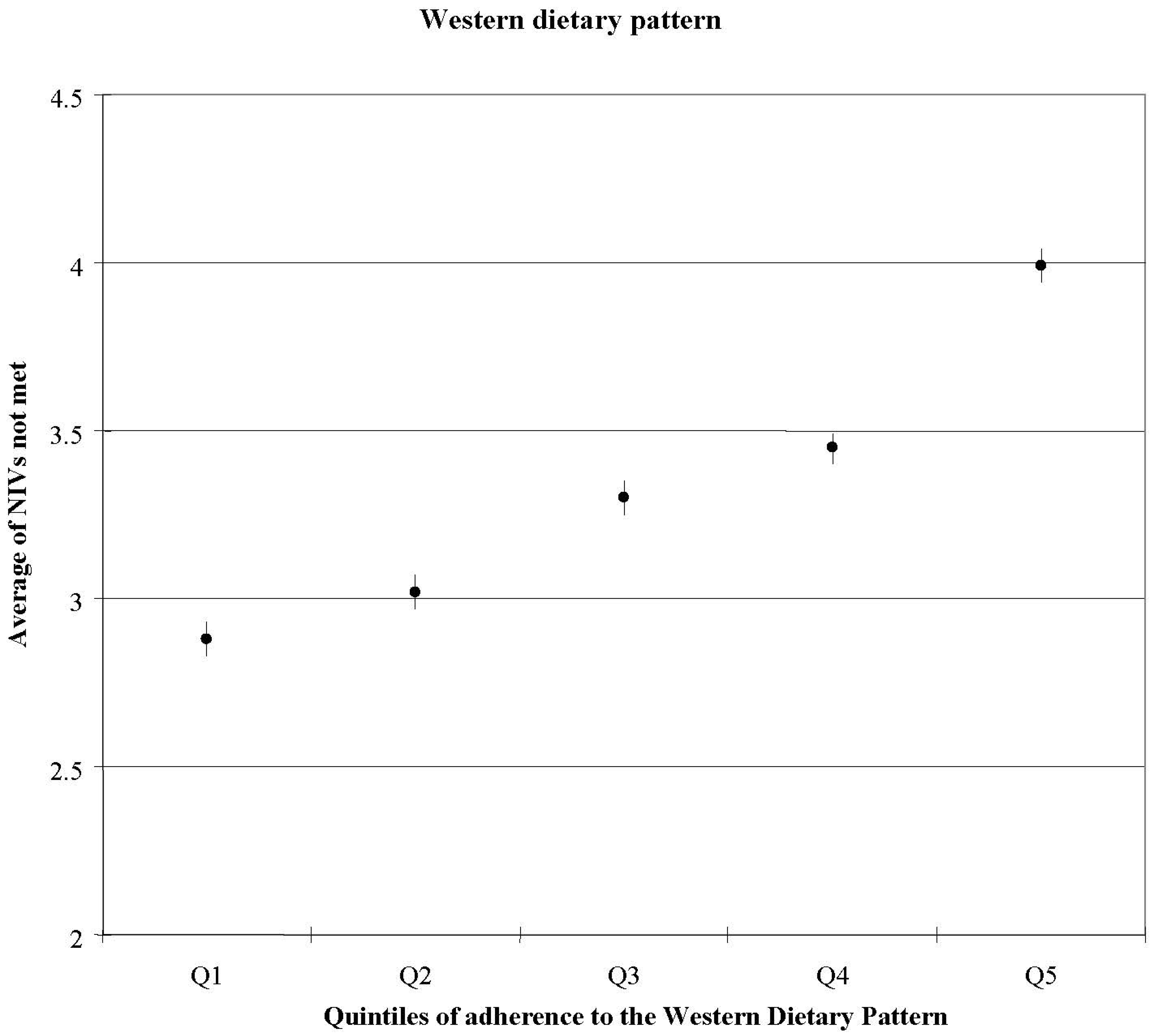
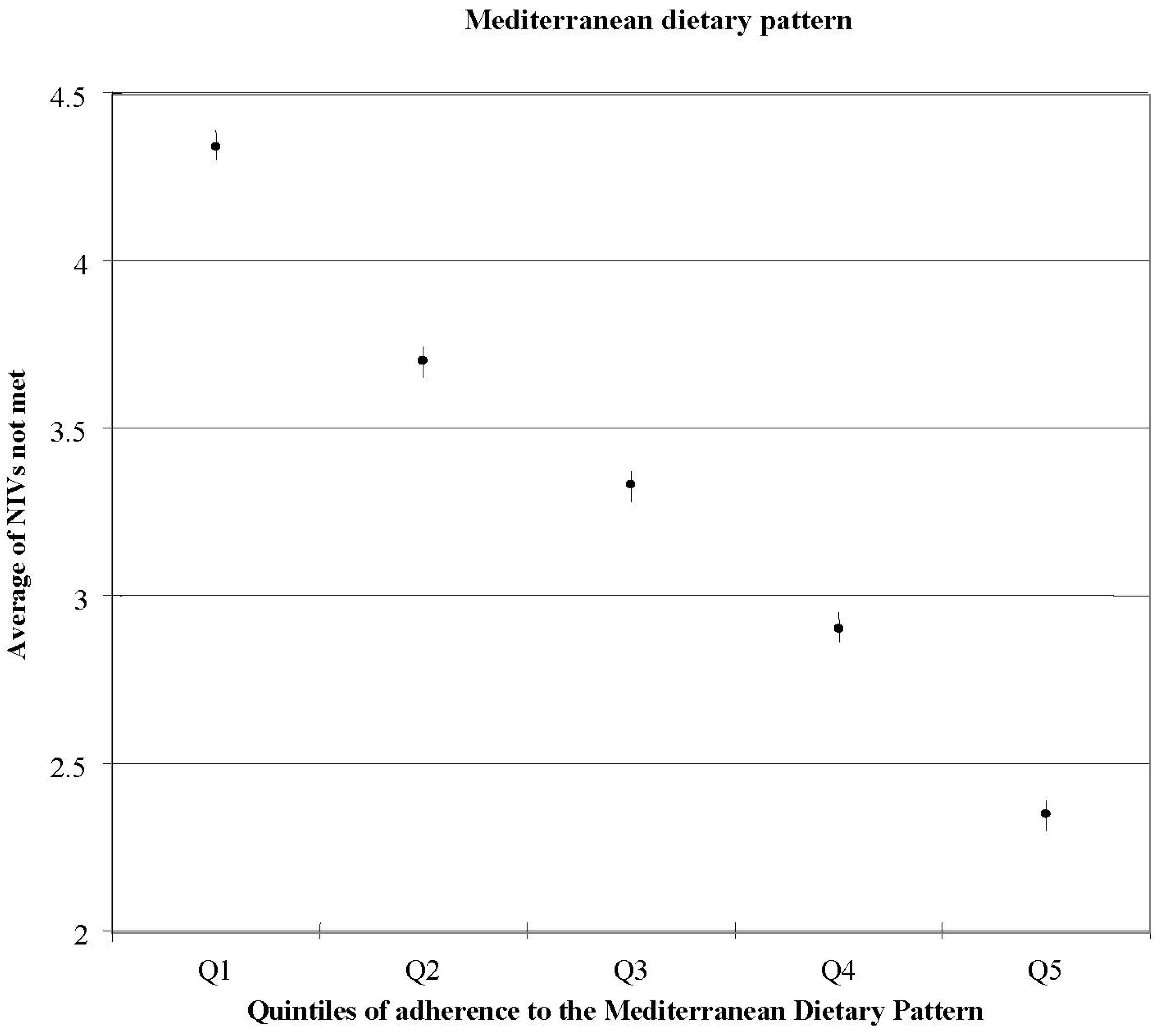
3.2. Nutritional Adequacy of the Mediterranean and Western Dietary Patterns

{kind=link}
{kind=link}
{kind=link}
| Food groups * | Dietary Patterns ** | |
|---|---|---|
| Factor 1 (Western) | Factor 2 (Mediterranean) | |
| Olive oil | - | 0.32 |
| Poultry | - | 0.38 |
| Red meat | 0.54 | - |
| Processed meat | 0.5 | - |
| Eggs | 0.37 | - |
| Fish | - | 0.59 |
| Sauces | 0.42 | - |
| Pre-cooked food | 0.41 | - |
| Fast food | 0.57 | - |
| Caloric soft drinks | 0.35 | - |
| Commercial sweets | 0.4 | - |
| Whole fat dairy | 0.43 | - |
| Low fat dairy | −0.31 | 0.37 |
| Legumes | - | 0.3 |
| Vegetables | - | 0.68 |
| Fruits | - | 0.54 |
| Potatoes | 0.45 | - |
3.3. Nutritional Adequacy in Children and the Mediterranean Diet
| KIDMED test | Scoring |
|---|---|
| Takes a fruit or fruit juice every day | +1 |
| Has a second fruit every day | +1 |
| Has fresh or cooked vegetables regularly once a day | +1 |
| Has fresh or cooked vegetables more than once a day | +1 |
| Consumes fish regularly (at least 2–3/week) | +1 |
| Goes >1/week to a fast food restaurant (hamburger) | −1 |
| Likes pulses and eats them >1/week | +1 |
| Consumes pasta or rice almost every day (5 or more per week) | +1 |
| Has cereals or grains (bread, etc.) for breakfast | +1 |
| Consumes nuts regularly (at least 2–3/week) | +1 |
| Uses olive oil at home | +1 |
| Skips breakfast | −1 |
| Has a dairy product for breakfast (yoghurt, milk, etc.) | +1 |
| Has commercially baked goods or pastries for breakfast | −1 |
| Takes two yoghurts and/or some cheese (40 g) daily | +1 |
| Takes sweets and candy several times every day | −1 |
| KIDMED Index | Adherence to the Mediterranean Diet |
| Score ≤ 3 points | Poor |
| Score 4–7 points | Medium |
| Score ≥ 8 points | High |
| KIDMED Index for 6–14 years | ||||
|---|---|---|---|---|
| Poor ≤ 3 (%) | Medium 4–7 (%) | High ≥ 8 (%) | p-trend | |
| Men/Women | ||||
| Energy | 4.8/13.3 | 1.9/6.9 | 1.3/6.3 | 0.303/0.467 |
| Protein | 0.0/0.0 | 0.0/0.0 | 0.0/0.0 | - |
| Calcium | 4.8/26.7 | 2.6/10.4 | 0.4/4.2 | 0.027/<0.000 |
| Iron | 0.0/33.3 | 0.8/23.8 | 0.0/15.4 | 0.300/0.008 |
| Magnesium | 19.0/0.0 | 9.8/4.2 | 4.6/2.9 | 0.004/0.707 |
| Thiamin | 0.0/0.0 | 0.4/0.4 | 0.0/0.4 | 0.464/0.871 |
| Riboflavin | 0.0/0.0 | 1.1/1.2 | 0.4/0.8 | 0.559/0.881 |
| Niacin | 0.0/0.0 | 0.4/0.4 | 0.0/0.4 | 0.464/0.871 |
| Vitamin B6 | 0.0/33.3 | 3.0/10.8 | 2.9/5.0 | 0.724/<0.000 |
| Folate | 14.3/46.7 | 9.8/32.3 | 5.0/23.8 | 0.021/0.010 |
| Vitamin B12 | 0.0/0.0 | 0.0/0.0 | 0.0/0.0 | - |
| Vitamin C | 47.6/13.3 | 18/15.4 | 5.4/4.6 | ˂0.000/˂0.000 |
| Vitamin A | 57.1/80.0 | 63.9/61.5 | 59.6/54.2 | 0.523/0.024 |
| Vitamin D | 100.0/100.0 | 95.9/99.6 | 95.8/97.1 | 0.618/0.024 |
| Vitamin E | 28.6/66.7 | 43.2/60.8 | 36.3/57.1 | 0.394/0.310 |
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402–1406. [Google Scholar]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet foundation expert group. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2784. [Google Scholar] [CrossRef]
- Bos, M.B.; de Vries, J.H.; Feskens, E.J.; van Dijk, S.J.; Hoelen, D.W.; Siebelink, E.; Heijligenberg, R.; de Groot, L.C. Effect of a high monounsaturated fatty acids diet and a Mediterranean diet on serum lipids and insulin sensitivity in adults with mild abdominal obesity. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 591–598. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Bes-Rastrollo, M.; Román-Viñas, B.; Pfrimer, K.; Sánchez-Villegas, A.; Martínez-González, M.A. Dietary patterns and nutritional adequacy in a Mediterranean country. Br. J. Nutr. 2009, 101, 21–28. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Basora-Gallisá, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Escoda, R.; et al. Effects of dietary fibre intake on risk factors for cardiovascular disease in subjects at high risk. J. Epidemiol. Community Health 2009, 63, 582–588. [Google Scholar] [CrossRef]
- Rodríguez-Rejón, A.I.; Castro-Quezada, I.; Ruano-Rodríguez, C.; Ruiz-López, M.D.; Sánchez-Villegas, A.; Toledo, E.; Artacho, R.; Estruch, R.; Salas-Salvadó, J.; Covas, M.I.; et al. Effect of a Mediterranean diet intervention on dietary glycemic index and dietary glycemic load: The PREDIMED study. J. Nutr. Educ. Behav. submitted for publication. 2013. [Google Scholar]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Visioli, F.; Galli, C. The role of antioxidants in the Mediterranean diet. Lipids 2001, 36, 49–52. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Tzima, N.; Chrysohoou, C.; Economou, M.; Zampelas, A.; Stefanadis, C. Adherence to the Mediterranean diet is associated with total antioxidant capacity in healthy adults: The ATTICA study. Am. J. Clin. Nutr. 2005, 82, 694–699. [Google Scholar]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health. Biofactors 2013, 39, 335–342. [Google Scholar] [CrossRef]
- Mitrou, P.N.; Kipnis, V.; Thiébaut, A.C.; Reedy, J.; Subar, A.F.; Wirfält, E.; Flood, A.; Mouw, T.; Hollenbeck, A.R.; Leitzmann, M.F.; et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population: Results from the NIH-AARP Diet and Health Study. Arch. Intern. Med. 2007, 167, 2461–2468. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gomez-Gracia, E.; Ruiz-Gutiérrez, V.; et al. Prevention of diabetes with Mediterranean diets a subgroup analysis of a randomized trial. Ann. Intern. Med. 2013, 160, 1–10. [Google Scholar]
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.C.; Tjønneland, A.; Olsen, A.; Clavel-Chapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef]
- Román-Viñas, B.; Serra-Majem, L.; Ribas-Barba, L.; Ngo, J.; García-Álvarez, A.; Wijnhoven, T.M.; Tabacchi, G.; Branca, F.; de Vries, J.; de Groot, L.C. Overview of methods used to evaluate the adequacy of nutrient intakes for individuals and populations. Br. J. Nutr. 2009, 101, 6–11. [Google Scholar] [CrossRef]
- Dhonukshe-Rutten, R.A.; Bouwman, J.; Brown, K.A.; Cavelaars, A.E.; Collings, R.; Grammatikaki, E.; de Groot, L.C.; Gurinovic, M.; Harvey, L.J.; Hermoso, M.; et al. EURRECA-Evidence-based methodology for deriving micronutrient recommendations. Crit. Rev. Food Sci. Nutr. 2013, 53, 999–1040. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Aranceta, J.; Garaulet, M.; Carazo, E.; Mataix, J.; Pérez-Rodrigo, C.; Quemada, M.; Tojo, R.; et al. Risk of inadequate intake of vitamins A, B1, B6, C, E, folate, iron and calcium in the Spanish population aged 4 to 18. Int. J. Vitam. Nutr. Res. 2001, 71, 325–331. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Pérez-Rodrigo, C.; García-Closas, R.; Peña-Quintana, L.; Aranceta, J. Factors associated to nutrient intake among children and adolescents: Results from the EnKid study. Ann. Nutr. Metab. 2002, 46, 31–38. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academy Press: Washington, DC, USA, 2006; pp. 5–68. [Google Scholar]
- Román-Viñas, B.; Ribas Barba, L.; Ngo, J.; Martínez-González, M.A.; Wijnhoven, T.M.; Serra-Majem, L. Validity of dietary patterns to assess nutrient intake adequacy. Br. J. Nutr. 2009, 101, 12–20. [Google Scholar] [CrossRef]
- Dubois, L.; Girard, M.; Bergeron, N. The choice of a diet quality indicator to evaluate the nutritional health of populations. Public Health Nutr. 2000, 3, 357–365. [Google Scholar]
- Tabacchi, G.; Wijnhoven, T.M.; Branca, F.; Román-Viñas, B.; Ribas-Barba, L.; Ngo, J.; García-Álvarez, A.; Serra-Majem, L. How is the adequacy of micronutrient intake assessed across Europe? A systematic literature review. Br. J. Nutr. 2009, 101, 29–36. [Google Scholar] [CrossRef]
- King, J.C.; Vorster, H.H.; Tome, D.G. Nutrient intake values (NIVs): A recommended terminology and framework for the derivation of values. Food Nutr. Bull. 2007, 28, 16–26. [Google Scholar]
- King, J.C.; Garza, C. Executive summary. Food Nutr. Bull. 2007, 28, 3–12. [Google Scholar]
- Vorster, H.H.; Murphy, S.P.; Allen, L.H.; King, J.C. Application of nutrient intake values (NIVs). Food Nutr. Bull. 2007, 28, 116–122. [Google Scholar]
- Murphy, S.P.; Vorster, H.H. Methods for using nutrient intake values (NIVs) to assess or plan nutrient intakes. Food Nutr. Bull. 2007, 28, 51–60. [Google Scholar]
- Serra-Majem, L.; Román-Viñas, B.; Ribas Barba, L.; Ngo, J. Vitamin Status in Europe and Spain. Methodology to Estimate Vitamin Intake Adequacy. In Hot Topics en Vitaminas y Salud; Alonso, E., Varela, G., Eds.; Fundación Tomás Pascual y Pilar Gómez-Cuétara, Universidad San Pablo CEU: Madrid, Spain, 2011; pp. 123–131. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes: Applications in Dietary Assessment; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- National Research Council. Recommended Dietary Allowances; National Research Council: Washington, DC, USA, 1941. [Google Scholar]
- Murphy, S.P.; Poos, M.I. Dietary reference intakes: Summary of applications in dietary assessment. Public Health Nutr. 2002, 5, 843–849. [Google Scholar] [CrossRef]
- Carriquiry, A.L. Assessing the prevalence of nutrient inadequacy. Public Health Nutr. 1999, 2, 23–33. [Google Scholar] [CrossRef]
- Gibson, R.S. Nutritional Assessment: A Laboratory Manual; Oxford University Press: New York, NY, USA, 1993. [Google Scholar]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Newby, P.K.; Hu, F.B.; Rimm, E.B.; Smith-Warner, S.A.; Feskanich, D.; Sampson, L.; Willett, W.C. Reproducibility and validity of the Diet Quality Index Revised as assessed by use of a food-frequency questionnaire. Am. J. Clin. Nutr. 2003, 78, 941–949. [Google Scholar]
- Weinstein, S.J.; Vogt, T.M.; Gerrior, S.A. Healthy Eating Index scores are associated with blood nutrient concentrations in the third National Health and Nutrition Examination Survey. J. Am. Diet. Assoc. 2004, 104, 576–584. [Google Scholar] [CrossRef]
- Mirmiran, P.; Azadbakht, L.; Azizi, F. Dietary diversity within food groups: An indicator of specific nutrient adequacy in Tehranian women. J. Am. Coll. Nutr. 2006, 25, 354–361. [Google Scholar] [CrossRef]
- Steyn, N.P.; Nel, J.H.; Nantel, G.; Kennedy, G.; Labadarios, D. Food variety and dietary diversity scores in children: Are they good indicators of dietary adequacy? Public Health Nutr. 2006, 9, 644–650. [Google Scholar]
- Bach, A.; Serra-Majem, L.; Carrasco, J.L.; Roman, B.; Ngo, J.; Bertomeu, I.; Obrador, B. The use of indexes evaluating the adherence to the Mediterranean diet in epidemiological studies: A review. Public Health Nutr. 2006, 9, 132–146. [Google Scholar]
- Alberti, A.; Fruttini, D.; Fidanza, F. The Mediterranean adequacy index: Further confirming results of validity. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 61–66. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur. J. Clin. Nutr. 2003, 57, 35–39. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean diet quality index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar]
- Newby, P.K.; Weismayer, C.; Akesson, A.; Tucker, K.L.; Wolk, A. Long-term stability of food patterns identified by use of factor analysis among Swedish women. J. Nutr. 2006, 136, 626–633. [Google Scholar]
- Roman-Viñas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Serra-Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef]
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European nutrition and health report 2009. Forum. Nutr. 2009, 62, 1–40. [Google Scholar] [CrossRef]
- Mensink, G.B.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef]
- Belgnaoui, S.; Belahsen, R. Nutrient intake and food consumption among pregnant women from an agricultural region of Morocco. Int. J. Food Sci. Nutr. 2006, 57, 19–27. [Google Scholar] [CrossRef]
- Méjean, C.; Traissac, P.; Eymard-Duvernay, S.; El Ati, J.; Delpeuch, F.; Maire, B. Diet quality of North African migrants in France partly explains their lower prevalence of diet-related chronic conditions relative to their native French peers. J. Nutr. 2007, 137, 2106–2113. [Google Scholar]
- Pekcan, G.; Karaagaoglu, N. State of nutrition in Turkey. Nutr. Health 2000, 14, 41–52. [Google Scholar] [CrossRef]
- Djazayery, A.; Pajooyan, J. Food consumption patterns and nutritional problems in the Islamic Republic of Iran. Nutr. Health 2000, 14, 53–61. [Google Scholar] [CrossRef]
- Atinmo, T.; Mirmiran, P.; Oyewole, O.E.; Belahsen, R.; Serra-Majem, L. Breaking the poverty/malnutrition cycle in Africa and the Middle East. Nutr. Rev. 2009, 67, S40–S46. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Geleva, D.; Carrasco, J.; Ribas-Barba, L.; Serra-Majem, L. Evaluating associations between Mediterranean diet adherence indexes and biomarkers of diet and disease. Public Health Nutr. 2006, 9, 1110–1117. [Google Scholar]
- Maillot, M.; Issa, C.; Vieux, F.; Lairon, D.; Darmon, N. The shortest way to reach nutritional goals is to adopt Mediterranean food choices: Evidence from computer-generated personalized diets. Am. J. Clin. Nutr. 2011, 94, 1127–1137. [Google Scholar] [CrossRef]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish school children and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar]
- Mesías, M.; Seiquer, I.; Navarro, M.P. Is the Mediterranean diet adequate to satisfy zinc requirements during adolescence? Public Health Nutr. 2012, 15, 1429–1436. [Google Scholar] [CrossRef]
- Mesías, M.; Seiquer, I.; Muñoz-Hoyos, A.; Galdó, G.; Navarro, M.P. The beneficial effect of Mediterranean dietary patterns on dietary iron utilization in male adolescents aged 11–14 years. Int. J. Food Sci. Nutr. 2009, 60, 355–368. [Google Scholar] [CrossRef]
- Seiquer, I.; Mesías, M.; Hoyos, A.M.; Galdó, G.; Navarro, M.P. A Mediterranean dietary style improves calcium utilization in healthy male adolescents. J. Am. Coll. Nutr. 2008, 27, 454–462. [Google Scholar] [CrossRef]
- Heidemann, C.; Schulze, M.B.; Franco, O.H.; van Dam, R.M.; Mantzoros, C.S.; Hu, F.B. Dietary patterns and risk of mortality from cardiovascular disease, cancer, and all causes in a prospective cohort of women. Circulation 2008, 118, 230–237. [Google Scholar] [CrossRef]
- Beaudry, M.; Galibois, I.; Chaumette, P. Dietary patterns of adults in Québec and their nutritional adequacy. Can. J. Public Health 1998, 89, 347–351. [Google Scholar]
- Costacou, T.; Bamia, C.; Ferrari, P.; Riboli, E.; Trichopoulos, D.; Trichopoulou, A. Tracing the Mediterranean diet through principal components and cluster analyses in the Greek population. Eur. J. Clin. Nutr. 2003, 57, 1378–1385. [Google Scholar] [CrossRef]
- Zhang, C.; Schulze, M.B.; Solomon, C.G.; Hu, F.B. A prospective study of dietary patterns, meat intake and the risk of gestational diabetes mellitus. Diabetologia 2007, 49, 2604–2613. [Google Scholar]
- Fung, T.T.; Willett, W.C.; Stampfer, M.J.; Manson, J.E.; Hu, F.B. Dietary patterns and the risk of coronary heart disease in women. Arch. Intern. Med. 2001, 161, 1857–1862. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Dietary patterns and markers of systemic inflammation among Iranian women. J. Nutr. 2007, 137, 992–998. [Google Scholar]
- Sakamoto, M. Mediterranean diet and life style: Comparison with Japanese and other eastern diets. Int. J. Vitam. Nutr. Res. 2001, 71, 159–165. [Google Scholar] [CrossRef]
- Willcox, D.C.; Willcox, B.J.; Todoriki, H.; Suzuki, M. The Okinawan diet: Health implications of a low-calorie, nutrient-dense, antioxidant-rich dietary pattern low in glycemic load. J. Am. Coll. Nutr. 2009, 28, 500S–516S. [Google Scholar] [CrossRef]
- Serra-Majem, L. Japomediterranean diet? Eur. J. Clin. Nutr. 2004, 58, 1324–1325. [Google Scholar] [CrossRef]
- Saura-Calixto, F.; Goñi, I. Definition of the Mediterranean diet based on bioactive compounds. Crit. Rev. Food Sci. Nutr. 2009, 49, 145–152. [Google Scholar] [CrossRef]
- Su, Q.; Rowley, K.G.; Itsiopoulos, C.; O’Dea, K. Identification and quantification of major carotenoids in selected components of the Mediterranean diet: Green leafy vegetables, figs and olive oil. Eur. J. Clin. Nutr. 2002, 56, 1149–1154. [Google Scholar] [CrossRef]
- Bemelmans, W.J.; Broer, J.; de Vries, J.H.; Hulshof, K.F.; May, J.F.; Meyboom-De Jong, B. Impact of Mediterranean diet education versus posted leaflet on dietary habits and serum cholesterol in a high risk population for cardiovascular disease. Public Health Nutr. 2000, 3, 273–283. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean Diet and Nutritional Adequacy: A Review. Nutrients 2014, 6, 231-248. https://doi.org/10.3390/nu6010231
Castro-Quezada I, Román-Viñas B, Serra-Majem L. The Mediterranean Diet and Nutritional Adequacy: A Review. Nutrients. 2014; 6(1):231-248. https://doi.org/10.3390/nu6010231
Chicago/Turabian StyleCastro-Quezada, Itandehui, Blanca Román-Viñas, and Lluís Serra-Majem. 2014. "The Mediterranean Diet and Nutritional Adequacy: A Review" Nutrients 6, no. 1: 231-248. https://doi.org/10.3390/nu6010231