The Effect of Arthrospira platensis Capsules on CD4 T-Cells and Antioxidative Capacity in a Randomized Pilot Study of Adult Women Infected with Human Immunodeficiency Virus Not under HAART in Yaoundé, Cameroon

Abstract
:1. Introduction
2. Experimental Section

{kind=link}
{kind=link}
{kind=link}
| Nutritional Composition | A. platensis (500 mg) | Placebo (500 mg) |
|---|---|---|
| Energy | 8.9 kJ/2.1 kcal | 8.8 kJ/ 2.1 kcal |
| Protein | 310 mg | 310 mg |
| Carbohydrate | 77.5 mg | 186 mg |
| Lipid | 35.5 mg | 4 mg |
2.1. Marker Variables
2.2. Statistics
3. Results
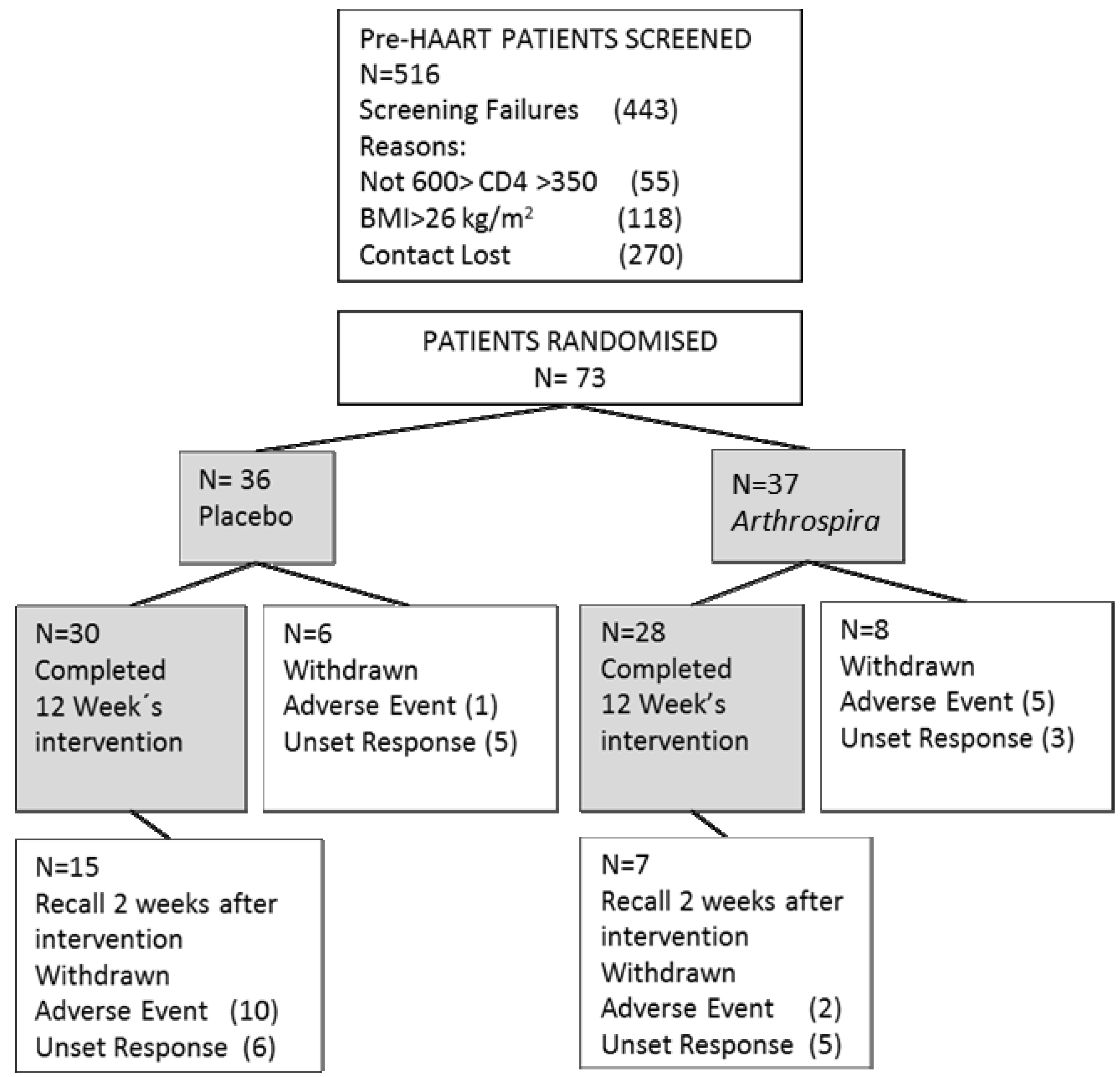
3.1. Population

3.2. Blood Analyses

| Baseline | Intervention | Difference | |||||
|---|---|---|---|---|---|---|---|
| Placebo n = 30 | Arthrospira n = 28 | Placebo n = 30 | Arthrospira n = 28 | Placebo n = 30 | Arthrospira n = 28 | ||
| Variables | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | |
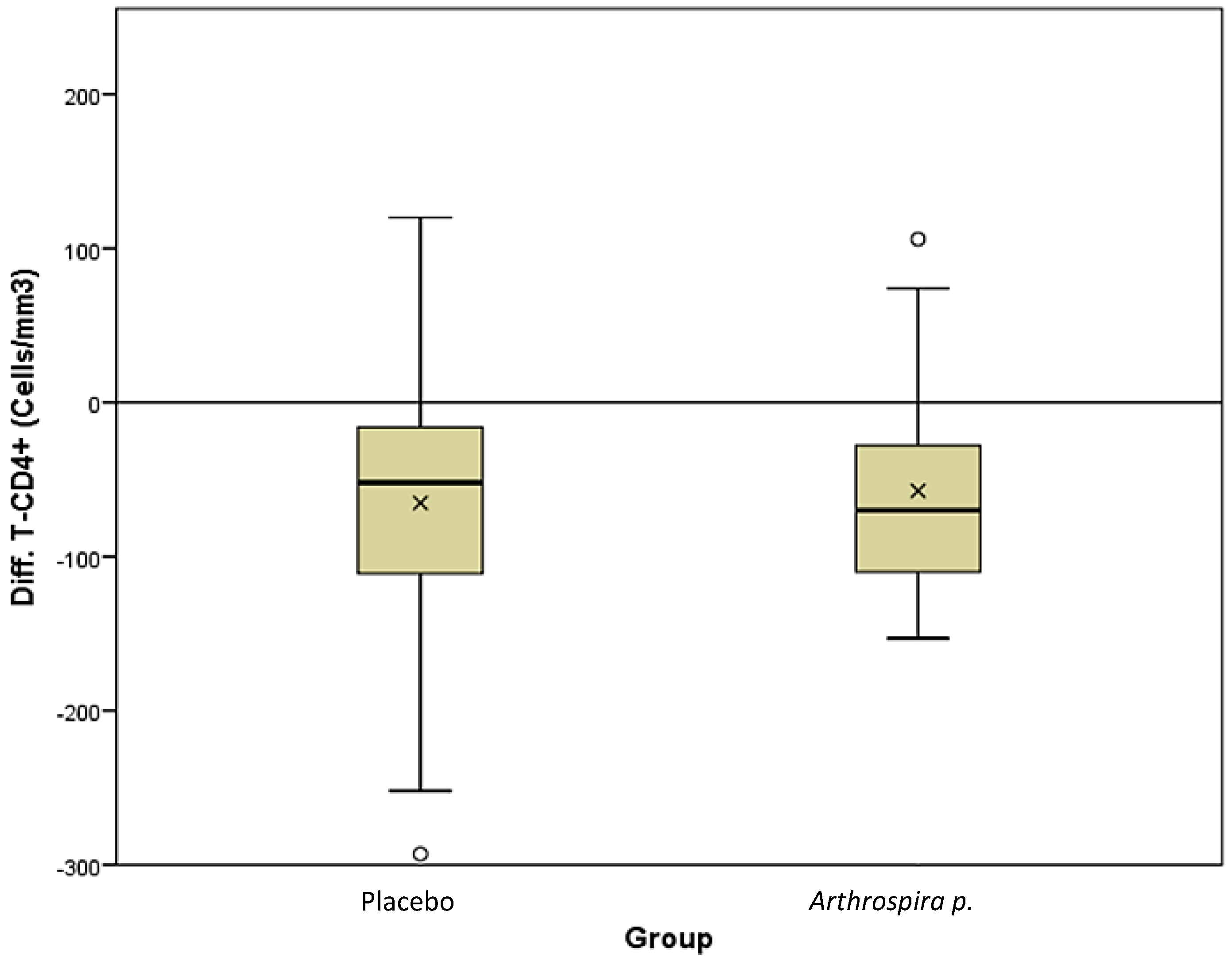
| CD4 (Cells/mm3) | 462 (413–558) | 440 (415–550) | 417 (311–486) | 406 (320–499) | −52 (−112–−16) | −66 (−111–−20) | |
| Viral load (Log10) | 5.6 (5.1–6) | 5.3 (4.3–5.8) | 5.5 (4.7–5.9) | 5.3 (4.5–5.9) | 0.0 (−0.4–0 0.2) | 0.05 (−0.2–0.4) | |
| CD8/CD38 (%) | 25.2 (17.1–37.1) | 22.4 (16.2–30.5) | 21.2 (15.5–36.3) | 24.5 (14.5–29.9) | −0.9 (−4.17–1.56) | −1.3 (−5.8–2.0) | |
| Weight (kg) | 56. 8 (54.1–61.7) | 57.3 (53.2–62.3) | 58.4 (54.9–63.1) | 57.8 (52.9–62.5) | 0.65 (−0.1–2.9) | 0.5 (−0.35–1.65) | |
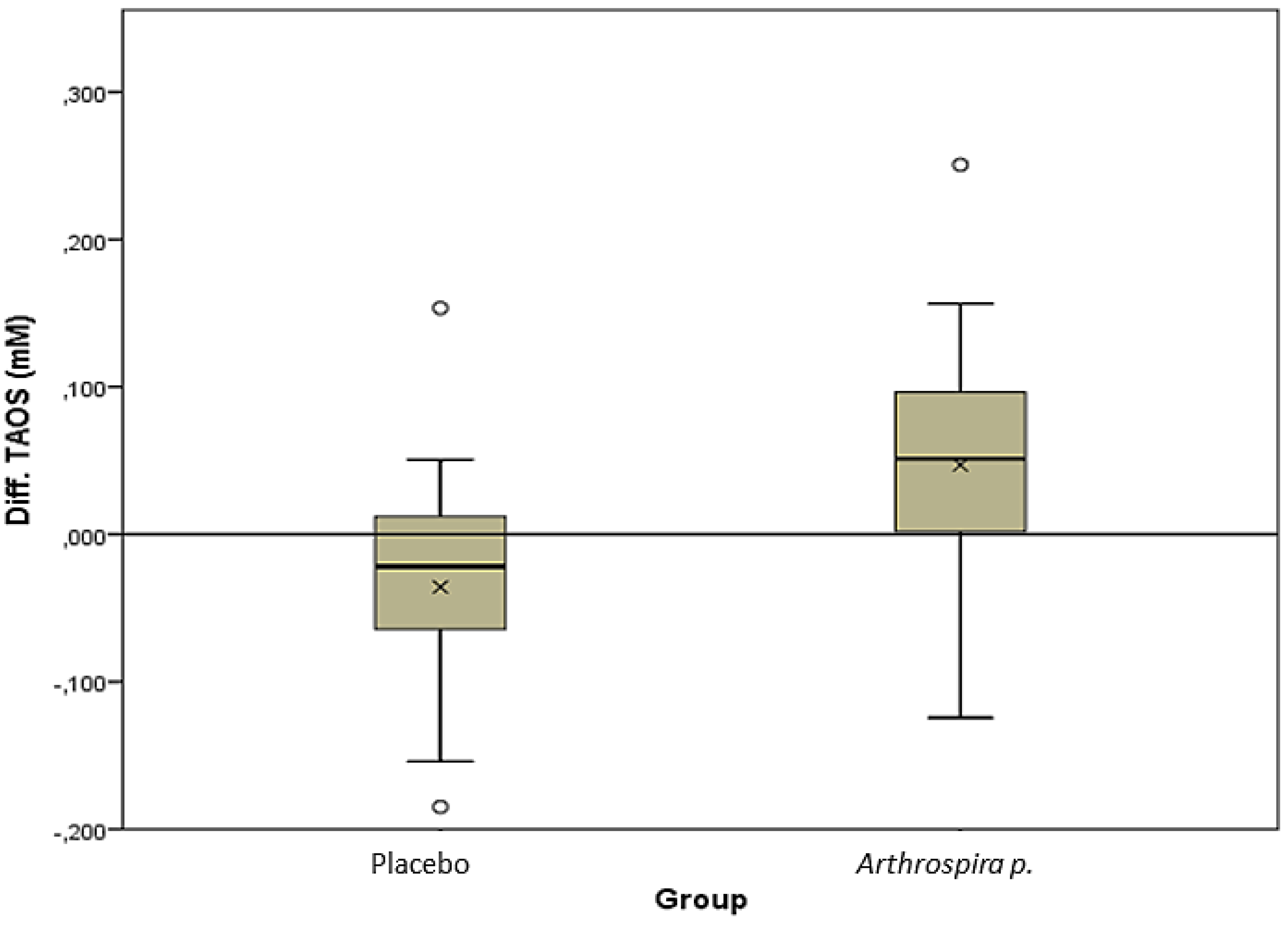
| TAOS (µM) | 357 (298–424) | 330 (275–384) | 336 (275–373) | 387 (320–430) | −22 (−64–19) | 56 (1–98) | |
| Albumin (g/L) | 49.5 (47–52) | 49 (47–51) | 47.5 (46–49) | 47 (44.5–50) | −1.5 (−4.0–1) | −3.0 (−4–0) | |
| Urea (g/L) | 0.19 (0.16–0.22) | 0.17 (0.13–0.20) | 0.18 (0.15–0.22) | 0.18 (0.12–0.22) | 0.00 (−0.30–0.04) | 0.00 (−0.35–0.03) | |
| Creatinine (mg/dL) | 0.7 (0.6–0.8) | 0.7 (0.6–0.7) | 0.7 (0.6–0.8) | 0.75 (0.6–0.85) | 0.0 (−0.1–0.1) | 0.1 (0.0–0.2) | |
| eGFR (mL/min) | 57.7 (50.5–61.1) | 59.8 (51.2–72) | 56.6 (48.7–70.5) | 51.3 (43–67.1) | 0.01 (−6.7–4.6) | −7.3 (−17.2–0.9) | |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. World Health Statistics 2011; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic 2012; UNAIDS: Geneva, Switzerland, 2012. [Google Scholar]
- Autran, B.; Carcelain, G.; Li, T.S.; Blanc, C.; Mathez, D.; Tubiana, R.; Katlama, C.; Debré, P.; Leibowitch, J. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science 1997, 277, 112–116. [Google Scholar] [CrossRef]
- WHO. Gobal HIV/AIDS Response; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic 2010; UNAIDS: Geneva, Switzerland, 2010. [Google Scholar]
- National Institute of Statistic I. Rapport Préliminaire sur la Prévalence du VIH: Institut National de la Statistique; National Institute of Statistic I: Yaoundé, Cameroon, 2011. [Google Scholar]
- CNLS. L’impact du VIH et du SIDA au Cameroun à l´horizon 2020; Yaounde; CNLS: Yaoundé, Cameroon, 2010. [Google Scholar]
- Koethe, J.R.; Heimburger, D.C. Nutritional aspects of HIV-associated wasting in sub-Saharan Africa. Am. J. Clin. Nutr. 2010, 91, 1138–1142. [Google Scholar] [CrossRef]
- Irlam, J.H.; Visser, M.M.E.; Siegfried, N. Micronutrient supplementation in children and adults with HIV infection, overreview. Cochrane Collab. 2009, 1, 1–77. [Google Scholar]
- Nkengfack, G.N.; Torimiro, J.N.; Englert, H. Effects of antioxidants on CD4 and viral load in HIV-infected women in sub-Saharan Africa—Dietary supplements vs. local diet. Int. J. Vitam. Nutr. Res. 2012, 82, 63–72. [Google Scholar] [CrossRef]
- Forrester, J.E.; Sztam, K.A. Micronutrients in HIV/AIDS: Is there evidence to change the WHO 2003 recommendations? Am. J. Clin. Nutr. 2011, 94, 1683–1689. [Google Scholar] [CrossRef]
- Rabeneck, L.; Palmer, A.; Knowles, J.B.; Seidehamel, R.J.; Harris, C.L.; Merkel, K.L.; Risser, J.M.; Akrabawi, S.S. A randomized controlled trial evaluating nutrition counseling with or without oral supplementation in malnourished HIV-infected patients. J. Am. Diet. Assoc. 1998, 98, 434–438. [Google Scholar] [CrossRef]
- Fawzi, W.W.; Msamanga, G.I.; Spiegelman, D.; Wei, R.; Kapiga, S.; Villamor, E.; Mwakagile, D.; Mugusi, F.; Hertzmark, E.; Essex, M.; et al. Randomized Trial of Multivitamin Supplements and HIV Disease Progression and Mortality. N. Engl. J. Med. 2004, 351, 23–32. [Google Scholar] [CrossRef]
- Hummelen, R.; Hemsworth, J.; Reid, G. Micronutrients, N-acetyl cysteine, probiotics and prebiotics, a review of effectiveness in reducing HIV progression. Nutrients 2010, 2, 626–651. [Google Scholar] [CrossRef]
- Shils, M.E.; Shike, M. Modern Nutrition in Health and Disease, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Pace, G.W.; Leaf, C.D. Role of oxidative stress in HIV disease. Free Radic. Biol. Med. 1995, 19, 523–528. [Google Scholar] [CrossRef]
- Fields-Gardner, C. Position of the American Dietetic Association: Nutrition Intervention and Human Immunodeficiency Virus Infection. J. Am. Diet. Assoc. 2010, 110, 1105–1119. [Google Scholar] [CrossRef]
- Kuete, V. Potential of Cameroonian plants and derived products against microbial infections: A review. Planta Med. 2010, 76, 1479–1491. [Google Scholar] [CrossRef]
- Sawadogo, W.R.; Schumacher, M.; Teiten, M.H.; Dicato, M.; Diederich, M. Traditional West African pharmacopeia, plants and derived compounds for cancer therapy. Biochem. Pharmacol. 2012, 84, 1225–1240. [Google Scholar] [CrossRef]
- WHO. Executive board 116 th Session Statement: Nutrition and HIV/AIDS; WHO Executive Board: Geneva, Cameroon, 2005. [Google Scholar]
- Chandrasekhar, A.; Gupta, A. Nutrition and disease progression pre-highly active antiretroviral therapy (HAART) and post-HAART: Can good nutrition delay time to HAART and affect response to HAART? Am. J. Clin. Nutr. 2011, 94, 1703S–1715S. [Google Scholar] [CrossRef]
- Nuhu, A.A. Spirulina (Arthrospira): An Important Source of Nutritional and Medicinal Compounds. J. Mar. Biol. 2013, 2013. [Google Scholar] [CrossRef]
- Khan, Z.; Bhadouria, P.; Bisen, P.S. Nutritional and therapeutic potential of Spirulina. Curr. Pharm. Biotechnol. 2005, 6, 373–379. [Google Scholar] [CrossRef]
- Nikiéma, J.B.; Djierro, K.; Simpore, J.; Sia, D.; Sourabié, S.; Gnoula, C.; Guissou, I.P. Stratégie d’utilisation des substances naturelles dans la prise en charge des personnes vivant avec le VIH: Expérience du Burkina Faso. Ethnopharmacologia 2009, 43, 47–51. [Google Scholar]
- Yu, B.; Wang, J.; Suter, P.M.; Russell, R.M.; Grusak, M.A.; Wang, Y.; Wang, Z.; Yin, S.; Tang, G. Spirulina is an effective dietary source of zeaxanthin to humans. Br. J. Nutr. 2012, 108, 1–9. [Google Scholar] [CrossRef]
- Marles, R.; Barrett, M.; Barnes, J.; Chavez, M.; Gardiner, P.; Ko, R.; Mahady, G.B.; Low Dog, T.; Sarma, N.D.; Giancaspro, G.I.; et al. United States pharmacopeia safety evaluation of spirulina. Crit. Rev. Food Sci. Nutr. 2011, 51, 593–604. [Google Scholar] [CrossRef]
- Rechter, S.; Konig, T.; Auerochs, S.; Hulke, S.; Walter, H.; Dornenburg, H.; Walter, C.; Marschall, M. Antiviral activity of Arthrospira-derived spirulan-like substances. Antiviral Res. 2006, 72, 197–206. [Google Scholar] [CrossRef]
- Deng, R.; Chow, T.J. Hypolipidemic, antioxidant, and antiinflammatory activities of microalgae Spirulina. Cardiovasc. Ther. 2010, 28, e33–e45. [Google Scholar] [CrossRef]
- Kim, M.Y.; Cheong, S.H.; Lee, J.H.; Kim, M.J.; Sok, D.E.; Kim, M.R. Spirulina improves antioxidant status by reducing oxidative stress in rabbits fed a high-cholesterol diet. J. Med. Food 2010, 13, 420–426. [Google Scholar] [CrossRef]
- Teas, J.; Irhimeh, M.R. Dietary algae and HIV/AIDS: Proof of concept clinical data. J. Appl. Phycol. 2012, 24, 575–582. [Google Scholar] [CrossRef]
- Teas, J.; Hebertb, R.B.; Fittonc, J.H.; Zimbad, P.V. Algae—A poor man’s HAART? Med. Hypotheses 2004, 62, 507–510. [Google Scholar] [CrossRef]
- Mariken, J.T.J.; Dallinga, J.S.; Voss, H.-P.; Haenen, G.; Bast, A. A new approach to assess the total antioxidant capacity using the TEAC assay. Food Chem. 2004, 88, 567–570. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Sabin, C.A.; Devereux, H.; Phillips, A.N.; Hill, A.; Janossy, G.; Lee, C.A.; Loveday, C. Course of viral load throughout HIV-1 infection. J. Acquir. Immun. Defic. Syndr. 2000, 23, 172–177. [Google Scholar] [CrossRef]
- Cuevas, A.; Saavedra, N.; Salazar, L.A.; Abdalla, D.S. Modulation of immune function by polyphenols: Possible contribution of epigenetic factors. Nutrients 2013, 5, 2314–2332. [Google Scholar] [CrossRef]
- Hayashi, T.; Hayashit, K. Calcium Spirulan, an Inhibitor of Enveloped Virus Replication, from a Blue-Green Alga Spirulina platensis. J. Nat. Prod. 1996, 59, 83–87. [Google Scholar] [CrossRef]
- Schwarz, K.B. Oxidative stress during viral infection: A review. Free Radic. Biol. Med. 1996, 21, 641–649. [Google Scholar] [CrossRef]
- Ghiselli, A.; Serafini, M.; Natella, F.; Scaccini, C. Total antioxidant capacity as a tool to assess redox status: Critical view and experimental data. Free Radic. Biol. Med. 2000, 29, 1106–1114. [Google Scholar] [CrossRef]
- Coaccioli, S.; Crapa, G.; Fantera, M.; Del Giorno, R.; Lavagna, A.; Standoli, M.L.; Frongillo, R.; Biondi, R.; Puxeddu, A. Oxidant/antioxidant status in patients with chronic HIV infection. Clin. Ther. 2010, 161, 55–58. [Google Scholar]
- Schreck, R.; Rieber, P.; Baeuerle, P.A. Reactive oxygen intermediates as apparently widely used messengers in the activation of the NF-kappa B transcription factor and HIV-1. EMBO J. 1991, 10, 2247–2258. [Google Scholar]
- Kabe, Y.; Ando, K.; Hirao, S.; Yoshida, M.; Handa, H. Redox regulation of NF-kappaB activation: Distinct redox regulation between the cytoplasm and the nucleus. Antioxid. Redox Signal. 2005, 7, 395–403. [Google Scholar] [CrossRef]
- Yamani, E.; Kaba-Mebri, J.; Mouala, C.; Gresenguet, G.; Rey, J.L. Use of spirulina supplement for nutritional management of HIV-infected patients: Study in Bangui, Central African Republic. Med. Trop. 2009, 69, 66–70. [Google Scholar]
- Selmi, C.; Leung, P.S.C.; Fischer, L.; German, B.; Yang, C.-Y.; Kenny, T.P.; Cysewski, G.R.; Gershwin, M.E. The effects of Spirulina on anemia and immune function in senior citizens. Cell. Mol. Immunol. 2011, 8, 248–254. [Google Scholar] [CrossRef]
- Simpore, J.; Pignatelli, S.; Musumeci, S. The effects of Spiruline on the immune functions of HIV-infected undernourished children. J. Infect. Dev. Ctries. 2007, 1, 112–117. [Google Scholar]
- Azabji-Kenfack, M.; Ekali, L.G.; Eugene, S.; Arnold, O.E.; Sandrine, E.D.; von der Weid, D.; Gbaguidi, E.; Ngogang, J.; Mbanya, J.C. The effect of Spirulina platensis versus soybean on insulin resistance in HIV-infected patients: A randomized pilot study. Nutrients 2011, 3, 712–724. [Google Scholar] [CrossRef]
- Azabji-Kenfack, M.; Dikosso, S.E.; Loni, E.G.; Onana, E.A.; Sobngwi, E.; Gbaguidi, E.; Gbaguidi, A.L.; Ngougni Kana, G.; Nguefack-Tsague, D.; von der Weid, O.; et al. Potential of Spirulina Platensis as a Nutritional Supplement in Malnourished HIV-Infected Adults in Sub-Saharan Africa: A Randomised, Single-Blind Study. Nutr. Metab. Insights 2011, 4, 29–37. [Google Scholar]
- Nielsen, C.H.; Balachandran, P.; Christensen, O.; Pugh, N.D.; Tamta, H.; Sufka, K.J.; Wu, X.; Walsted, A.; Schjørring-Thyssen, M.; Enevold, C.; et al. Enhancement of natural killer cell activity in healthy subjects by Immulina(R), a Spirulina extract enriched for Braun-type lipoproteins. Planta Med. 2010, 76, 1802–1808. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Winter, F.S.; Emakam, F.; Kfutwah, A.; Hermann, J.; Azabji-Kenfack, M.; Krawinkel, M.B. The Effect of Arthrospira platensis Capsules on CD4 T-Cells and Antioxidative Capacity in a Randomized Pilot Study of Adult Women Infected with Human Immunodeficiency Virus Not under HAART in Yaoundé, Cameroon. Nutrients 2014, 6, 2973-2986. https://doi.org/10.3390/nu6072973
Winter FS, Emakam F, Kfutwah A, Hermann J, Azabji-Kenfack M, Krawinkel MB. The Effect of Arthrospira platensis Capsules on CD4 T-Cells and Antioxidative Capacity in a Randomized Pilot Study of Adult Women Infected with Human Immunodeficiency Virus Not under HAART in Yaoundé, Cameroon. Nutrients. 2014; 6(7):2973-2986. https://doi.org/10.3390/nu6072973
Chicago/Turabian StyleWinter, Frank Stéphane, Francois Emakam, Anfumbom Kfutwah, Johannes Hermann, Marcel Azabji-Kenfack, and Michael B. Krawinkel. 2014. "The Effect of Arthrospira platensis Capsules on CD4 T-Cells and Antioxidative Capacity in a Randomized Pilot Study of Adult Women Infected with Human Immunodeficiency Virus Not under HAART in Yaoundé, Cameroon" Nutrients 6, no. 7: 2973-2986. https://doi.org/10.3390/nu6072973