Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Background of Participants
2.2. Data Collection
2.3. Dietary Assessment
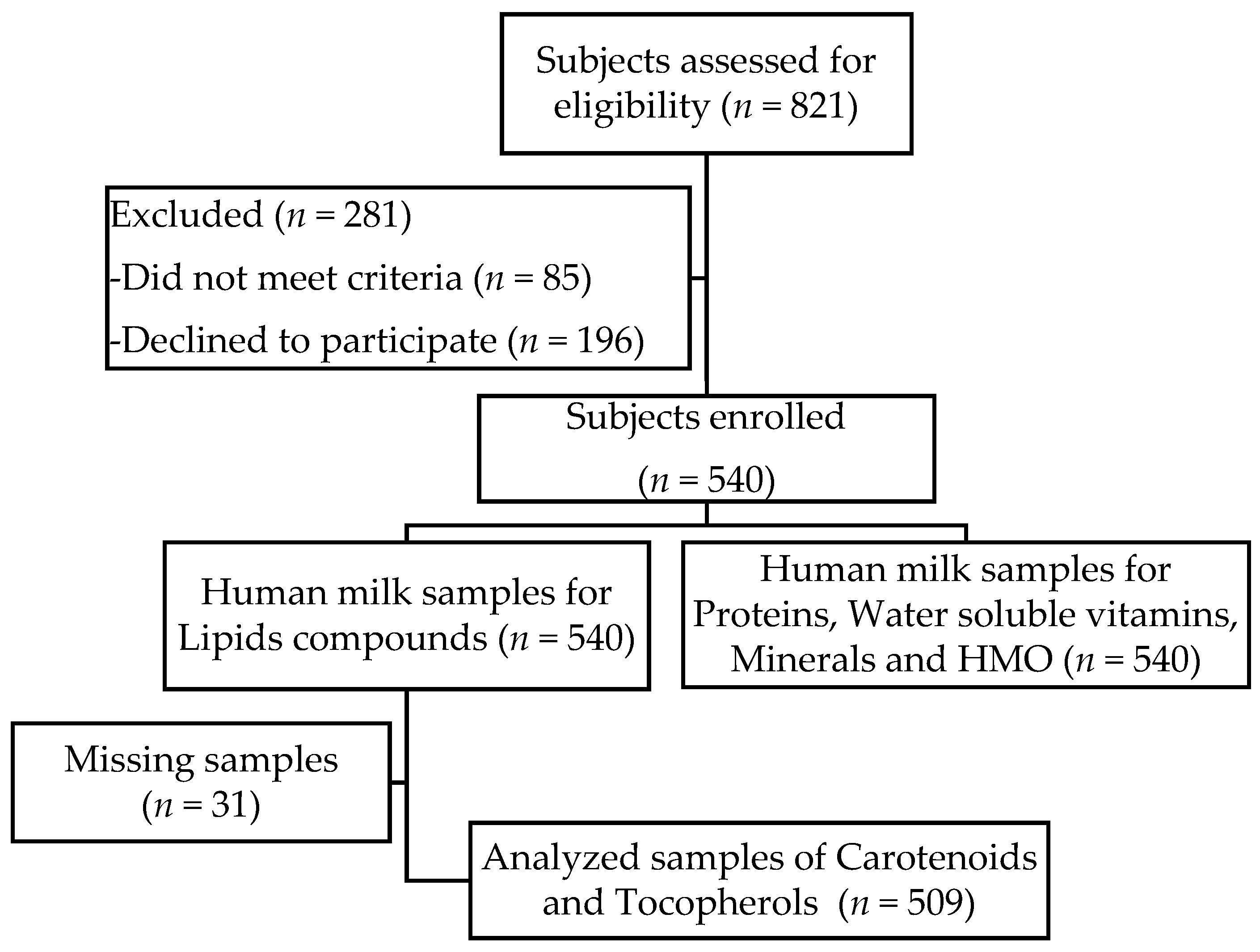
2.4. Sample Collection
2.5. Sample Preparation
2.6. Sample Analysis
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization/United Nations Children’s Fund. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Onyango, A.W.; Receveur, O.; Esrey, S.A. The contribution of breast milk to toddler diets in western Kenya. Bull. World Health Organ. 2002, 80, 292–299. [Google Scholar] [PubMed]
- Allen, L.H.; Haskell, M. Vitamin A requirements of infants under six months of age. Food Nutr. Bull. 2001, 22, 214–234. [Google Scholar] [CrossRef]
- World Health Organization and Food and Agriculture Organization. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Stam, J.; Sauer, P.J.; Boehm, G. Can we define an infant’s need from the composition of human milk? Am. J. Clin. Nutr. 2013, 98, S521–S528. [Google Scholar] [CrossRef] [PubMed]
- Powers, H.J. Vitamin requirements for term infants: Considerations for infant formulae. Nutr. Res. Rev. 1997, 10, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Ball, G.F.M. Vitamins: Their Role in the Human Body; Ball, G.F.M., Ed.; Blackwell Science Ltd.: Hoboken, NJ, USA, 2004; Chapter 7; pp. 133–187. [Google Scholar]
- Ball, G.F.M. Vitamins: Their Role in the Human Body; Ball, G.F.M., Ed.; Blackwell Science Ltd.: Hoboken, NJ, USA, 2004; Chapter 9; pp. 234–255. [Google Scholar]
- Allen, L.H. Multiple micronutrients in pregnancy and lactation: An overview. Am. J. Clin. Nutr. 2005, 81, S1206–S1212. [Google Scholar]
- Picciano, M.F. Pregnancy and lactation: Physiological adjustments, nutritional requirements and the role of dietary supplements. J. Nutr. 2003, 133, S1997–S2002. [Google Scholar]
- Qian, J.; Chen, T.; Lu, W.; Wu, S.; Zhu, J. Breast milk macro- and micronutrient composition in lactating mothers from suburban and urban Shanghai. J. Paediatr. Child Health 2010, 46, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhang, Y.; Ning, Y.; You, L.; Ma, D.; Zheng, Y.; Yang, X.; Li, W.; Wang, J.; Wang, P. Breast milk macronutrient composition and the associated factors in urban Chinese mothers. Chin. Med. J. 2014, 127, 1721–1725. [Google Scholar] [PubMed]
- Ding, M.; Li, W.; Zhang, Y.; Wang, X.; Zhao, A.; Zhao, X.; Wang, P.; Sheng, Q.H. Amino acid composition of lactating mothers’ milk and confinement diet in rural north China. Asia Pac. J. Clin. Nutr. 2010, 19, 344–349. [Google Scholar] [PubMed]
- Xiang, M.; Harbige, L.S.; Zetterstrom, R. Breast milk levels of zinc and omega-6 polyunsaturated fatty acids and growth of healthy Chinese infants. Acta Paediatr. 2007, 96, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.M.; Zhang, T.Y.; Wang, Q.; Zetterstrom, R.; Strandvik, B. Fatty acid composition in breast milk and serum phospholipids of healthy term Chinese infants during first 6 weeks of life. Acta Paediatr. 2007, 96, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; Lei, S.; Li, T.; Zetterstrom, R. Composition of long chain polyunsaturated fatty acids in human milk and growth of young infants in rural areas of northern China. Acta Paediatr. 1999, 88, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.Y.; Kwan, K.Y.; Tong, K.K.; Ratnayake, W.M.; Li, H.Q.; Leung, S.S. Breast milk fatty acid composition: A comparative study between Hong Kong and Chongqing Chinese. Lipids 1997, 32, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Wan, Z.X.; Wang, X.L.; Xu, L.; Geng, Q.; Zhang, Y. Lipid content and fatty acids composition of mature human milk in rural north China. Br. J. Nutr. 2010, 103, 913–916. [Google Scholar] [CrossRef] [PubMed]
- Ruan, C.; Liu, X.; Man, H.; Ma, X.; Lu, G.; Duan, G.; DeFrancesco, C.A.; Connor, W.E. Milk composition in women from five different regions of China: The great diversity of milk fatty acids. J. Nutr. 1995, 125, 2993–2998. [Google Scholar] [PubMed]
- Li, J.; Fan, Y.; Zhang, Z.; Yu, H.; An, Y.; Kramer, J.K.; Deng, Z. Evaluating the trans fatty acid, CLA, PUFA and erucic acid diversity in human milk from five regions in China. Lipids 2009, 44, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Canfield, L.M.; Clandinin, M.T.; Davies, D.P.; Fernandez, M.C.; Jackson, J.; Hawkes, J.; Goldman, W.J.; Pramuk, K.; Reyes, H.; Sablan, B.; et al. Multinational study of major breast milk carotenoids of healthy mothers. Eur. J. Nutr. 2003, 42, 133–141. [Google Scholar] [PubMed]
- Shi, Y.D.; Sun, G.Q.; Zhang, Z.G.; Deng, X.; Kang, X.H.; Liu, Z.D.; Ma, Y.; Sheng, Q.H. The chemical composition of human milk from Inner Mongolia of China. Food Chem. 2011, 127, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Lipkie, T.E.; Morrow, A.L.; Jouni, Z.E.; McMahon, R.J.; Ferruzzi, M.G. Longitudinal survey of carotenoids in human milk from urban cohorts in China, Mexico, and the USA. PLoS ONE 2015, 10, e0127729. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.M.; Paixao, J.A.; Ferraz, C. Fat-soluble vitamins in human lactation. Int. J. Vitam. Nutr. Res. 2007, 77, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Schweigert, F.J.; Bathe, K.; Chen, F.; Buscher, U.; Dudenhausen, J.W. Effect of the stage of lactation in humans on carotenoid levels in milk, blood plasma and plasma lipoprotein fractions. Eur. J. Nutr. 2004, 43, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Macias, C.; Schweigert, F.J. Changes in the concentration of carotenoids, vitamin A, alpha-tocopherol and total lipids in human milk throughout early lactation. Ann. Nutr. Metab. 2001, 45, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Gossage, C.P.; Deyhim, M.; Yamini, S.; Douglass, L.W.; Moser-Veillon, P.B. Carotenoid composition of human milk during the first month postpartum and the response to beta-carotene supplementation. Am. J. Clin. Nutr. 2002, 76, 193–197. [Google Scholar] [PubMed]
- Nagayama, J.; Noda, K.; Uchikawa, T.; Maruyama, I.; Shimomura, H.; Miyahara, M. Effect of maternal chlorella supplementation on carotenoid concentration in breast milk at early lactation. Int. J. Food Sci. Nutr. 2014, 65, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Canfield, L.M.; Giuliano, A.R.; Neilson, E.M.; Blashil, B.M.; Graver, E.J.; Yap, H.H. Kinetics of the response of milk and serum beta-carotene to daily beta-carotene supplementation in healthy, lactating women. Am. J. Clin. Nutr. 1998, 67, 276–283. [Google Scholar] [PubMed]
- Turner, T.; Burri, B.J.; Jamil, K.M.; Jamil, M. The effects of daily consumption of beta-cryptoxanthin-rich tangerines and beta-carotene-rich sweet potatoes on vitamin A and carotenoid concentrations in plasma and breast milk of Bangladeshi women with low vitamin a status in a randomized controlled trial. Am. J. Clin. Nutr. 2013, 98, 1200–1208. [Google Scholar] [PubMed]
- Sherry, C.L.; Oliver, J.S.; Renzi, L.M.; Marriage, B.J. Lutein supplementation increases breast milk and plasma lutein concentrations in lactating women and infant plasma concentrations but does not affect other carotenoids. J. Nutr. 2014, 144, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Stuetz, W.; Carrara, V.I.; McGready, R.; Lee, S.J.; Erhardt, J.G.; Breuer, J.; Biesalski, H.K.; Nosten, F.H. Micronutrient status in lactating mothers before and after introduction of fortified flour: Cross-sectional surveys in Maela refugee camp. Eur. J. Nutr. 2012, 51, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Lietz, G.; Mulokozi, G.; Henry, J.C.; Tomkins, A.M. Xanthophyll and hydrocarbon carotenoid patterns differ in plasma and breast milk of women supplemented with red palm oil during pregnancy and lactation. J. Nutr. 2006, 136, 1821–1827. [Google Scholar] [PubMed]
- Webb, A.L.; Aboud, S.; Furtado, J.; Murrin, C.; Campos, H.; Fawzi, W.W.; Villamor, E. Effect of vitamin supplementation on breast milk concentrations of retinol, carotenoids and tocopherols in HIV-infected Tanzanian women. Eur. J. Clin. Nutr. 2009, 63, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.S.; Dimenstein, R.; Ribeiro, K.D. Vitamin E concentration in human milk and associated factors: A literature review. J. Pediatr. 2014, 90, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Tokusoglu, O.; Tansug, N.; Aksit, S.; Dinc, G.; Kasirga, E.; Ozcan, C. Retinol and alpha-tocopherol concentrations in breast milk of Turkish lactating mothers under different socio-economic status. Int. J. Food Sci. Nutr. 2008, 59, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Mello-Neto, J.; Rondo, P.H.; Oshiiwa, M.; Morgano, M.A.; Zacari, C.Z.; Domingues, S. The influence of maternal factors on the concentration of vitamin A in mature breast milk. Clin. Nutr. 2009, 28, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Szlagatys-Sidorkiewicz, A.; Zagierski, M.; Luczak, G.; Macur, K.; Baczek, T.; Kaminska, B. Maternal smoking does not influence vitamin A and E concentrations in mature breastmilk. Breastfeed. Med. 2012, 7, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Sethom, M.M.; Kacem, S.; Ksibi, I.; Feki, M.; Jebnoun, S.; Kaabachi, N. Retinol and alpha-tocopherol in the colostrum of lactating Tunisian women delivering prematurely: Associations with maternal characteristics. Pediatr. Neonatol. 2016, 57, 120–126. [Google Scholar] [CrossRef] [PubMed]
- De Azeredo, V.B.; Trugo, N.M. Retinol, carotenoids, and tocopherols in the milk of lactating adolescents and relationships with plasma concentrations. Nutrition 2008, 24, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Xu, L.; Guo, Y.; Ronsmans, C. Factors influencing rising caesarean section rates in China between 1988 and 2008. Bull. World Health Organ. 2012, 90, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Li, G.; Zou, L.; Li, C.; Chen, Y.; Yuan, Y.; Wang, X.; Jia, C.; Zhang, W. Cesarean delivery rate and indications in mainland China: A cross sectional study in 2011. Zhonghua Fu Chan Ke Za Zhi 2014, 49, 728–735. [Google Scholar] [PubMed]
- Cui, Z.; Dibley, M.J. Trends in dietary energy, fat, carbohydrate and protein intake in Chinese children and adolescents from 1991 to 2009. Br. J. Nutr. 2012, 108, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Yaktine, A.L. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; Pan, X.C. China Food Composition Tables (Book 1), 2nd ed.; Beijing Medical University Press: Beijing, China, 2009. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; Pan, X.C. China Food Composition Tables 2004 (Book 2), 2nd ed.; Beijing Medical University Press: Beijing, China, 2005. [Google Scholar]
- Agency, S.A.T. Standard Tables of Food Composition in Japan (In Japanese), 4th ed.; Ishiyaku Shuppan Publishers, Inc.: Tokyo, Japan, 2005. [Google Scholar]
- Szlagatys-Sidorkiewicz, A.; Zagierski, M.; Jankowska, A.; Luczak, G.; Macur, K.; Baczek, T.; Korzon, M.; Krzykowski, G.; Martysiak-Zurowska, D.; Kaminska, B. Longitudinal study of vitamins A, E and lipid oxidative damage in human milk throughout lactation. Early Hum. Dev. 2012, 88, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Martysiak-Zurowska, D.; Szlagatys-Sidorkiewicz, A.; Zagierski, M. Concentrations of alpha- and gamma-tocopherols in human breast milk during the first months of lactation and in infant formulas. Matern. Child Nutr. 2013, 9, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Marcuzzi, A.; Vecchi Brumatti, L.; Caruso, L.; Copertino, M.; Davanzo, R.; Radillo, O.; Comar, M.; Monasta, L. Presence of IL-9 in paired samples of human colostrum and transitional milk. J. Hum. Lact. 2013, 29, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Khodayar-Pardo, P.; Mira-Pascual, L.; Collado, M.C.; Martínez-Costa, C. Impact of lactation stage, gestational age and mode of delivery on breast milk microbiota. J. Perinatol. 2014, 34, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Pons, S.M.; Bargalló, A.C.; Folgoso, C.C.; López Sabater, M.C. Triacylglycerol composition in colostrum, transitional and mature human milk. Eur. J. Clin. Nutr. 2000, 54, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, T.; Furukawa, M.; Asoh, M.; Kanno, T.; Kojima, T.; Yonekubo, A. Fat-soluble and water-soluble vitamin contents of breast milk from Japanese women. J. Nutr. Sci. Vitaminol. 2005, 51, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Kamao, M.; Tsugawa, N.; Suhara, Y.; Wada, A.; Mori, T.; Murata, K.; Nishino, R.; Ukita, T.; Uenishi, K.; Tanaka, K.; et al. Quantification of fat-soluble vitamins in human breast milk by liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2007, 859, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Song, B.J.; Jouni, Z.E.; Ferruzzi, M.G. Assessment of phytochemical content in human milk during different stages of lactation. Nutrition 2013, 29, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Antonakou, A.; Chiou, A.; Andrikopoulos, N.K.; Bakoula, C.; Matalas, A.L. Breast milk tocopherol content during the first six months in exclusively breastfeeding Greek women. Eur. J. Nutr. 2011, 50, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Tijerina-Saenz, A.; Innis, S.M.; Kitts, D.D. Antioxidant capacity of human milk and its association with vitamins A and E and fatty acid composition. Acta Paediatr. 2009, 98, 1793–1798. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.C.; Zhou, L.S.; Zhang, G.F. Alpha-tocopherol content of breast milk in China. J. Nutr. Sci. Vitaminol. 1993, 39, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.C.; Zhang, G.F.; Zhou, L.S.; Guo, X.G.; Quan, Y.F. Alpha-tocopherol concentrations in human milk from mothers of preterm and full-term infants in China. Biomed. Environ. Sci. 1993, 6, 259–264. [Google Scholar] [PubMed]
- Grilo, E.C.; Lira, L.Q.; Dimenstein, R.; Ribeiro, K.D. Influence of prematurity and birth weight on the concentration of alpha-tocopherol in colostrum milk. Rev. Paul. Pediatr. 2013, 31, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Monsen, E.R. Dietary reference intakes for the antioxidant nutrients: Vitamin C, vitamin E, selenium, and carotenoids. J. Am. Diet. Assoc. 2000, 100, 637–640. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Viroonudomphol, D.; Pongpaew, P.; Tungtrongchitr, R.; Changbumrung, S.; Tungtrongchitr, A.; Phonrat, B.; Vudhivai, N.; Schelp, F.P. The relationships between anthropometric measurements, serum vitamin A and E concentrations and lipid profiles in overweight and obese subjects. Asia Pac. J. Clin. Nutr. 2003, 12, 73–79. [Google Scholar] [PubMed]
- Dizdar, E.A.; Sari, F.N.; Degirmencioglu, H.; Canpolat, F.E.; Oguz, S.S.; Uras, N.; Dilmen, U. Effect of mode of delivery on macronutrient content of breast milk. J. Matern. Fetal Neonatal Med. 2014, 27, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Simsek, Y.; Karabiyik, P.; Polat, K.; Duran, Z.; Polat, A. Mode of delivery changes oxidative and antioxidative properties of human milk: A prospective controlled clinical investigation. J. Matern. Fetal Neonatal Med. 2015, 28, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Grune, T.; Lietz, G.; Palou, A.; Ross, A.C.; Stahl, W.; Tang, G.; Thurnham, D.; Yin, S.A.; Biesalski, H.K. Beta-carotene is an important vitamin A source for humans. J. Nutr. 2010, 140, S2268–S2285. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Xiao, H.; Wu, K.; Yu, Z.; Ren, Y.; Zhao, Y.; Li, K.; Li, J.; Li, D. Retinol and α-tocopherol in human milk and their relationship with dietary intake during lactation. Food Funct. 2016, 7, 1985–1991. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 0–4 Days (n = 77) | 5–11 Days (n = 89) | 12–30 Days (n = 73) | 31–60 Days (n = 90) | 61–120 Days (n = 90) | 121–240 Days (n = 90) | p-Value | |
|---|---|---|---|---|---|---|---|
| Age, years 1 | 0.097 | ||||||
| <25 | 22 (28.6) | 27 (30.3) | 26 (35.6) | 18 (20.0) | 26 (28.9) | 36 (40.0) | |
| 25–30 | 35 (45.5) | 41 (46.1) | 29 (39.7) | 44 (48.9) | 50 (55.6) | 39 (43.3) | |
| >30 | 20 (26.0) | 21 (23.6) | 18 (24.7) | 28 (31.1) | 14 (15.6) | 15 (16.7) | |
| Offspring gender 1 | 0.158 | ||||||
| Male | 35 (45.5) | 51 (57.3) | 39 (53.4) | 48 (53.3) | 54 (60.0) | 43 (47.8) | |
| Female | 42 (54.5) | 38 (42.7) | 31 (42.5) | 39 (43.3) | 36 (40.0) | 44 (48.9) | |
| Education 1 | 0.003 * | ||||||
| Middle school or below | 17 (22.1) | 12 (13.5) | 16 (21.9) | 26 (28.9) | 22 (24.4) | 39 (43.3) | |
| High school | 23 (29.9) | 31 (34.8) | 27 (37.0) | 22 (24.4) | 25 (27.8) | 23 (25.6) | |
| College or above | 36 (46.8) | 45 (50.6) | 29 (39.7) | 42 (46.7) | 41 (45.6) | 26 (28.9) | |
| Family’s per capita income, Yuan/month 1 | 0.140 | ||||||
| <2000 | 16 (20.8) | 19 (21.3) | 16 (21.9) | 24 (26.7) | 26 (28.9) | 31 (34.4) | |
| 2000–4000 | 30 (39.0) | 37 (41.6) | 34 (46.6) | 41 (45.6) | 40 (44.4) | 41 (45.6) | |
| >4000 | 27 (35.1) | 30 (33.7) | 17 (23.3) | 23 (25.6) | 22 (24.4) | 18 (20.0) | |
| Unclear | 4 (5.2) | 3 (3.4) | 6 (8.2) | 2 (2.2) | 2 (2.2) | 0 (0.0) | |
| Delivery mode 1 | 0.002 * | ||||||
| Vaginal delivery | 29 (37.7) | 50 (56.2) | 35 (47.9) | 37 (41.1) | 55 (61.1) | 55 (61.1) | |
| Cesarean delivery | 48 (62.3) | 37 (41.6) | 38 (52.1) | 53 (58.9) | 35 (38.9) | 34 (37.8) | |
| Present BMI 1 | 0.075 | ||||||
| Underweight | 1 (1.3) | 5 (5.6) | 2 (2.7) | 2 (2.2) | 4 (4.4) | 8 (8.9) | |
| Normal | 48 (62.3) | 54 (60.7) | 47 (64.4) | 57 (63.3) | 69 (76.7) | 65 (72.2) | |
| Overweight | 24 (31.2) | 26 (29.2) | 23 (31.5) | 26 (28.9) | 16 (17.8) | 16 (17.8) | |
| Obesity | 4 (5.2) | 3 (3.4) | 1 (1.4) | 5 (5.6) | 1 (1.1) | 1 (1.1) | |
| Gestational weight gain 1 | 0.300 | ||||||
| Inadequate | 17 (22.1) | 11 (12.4) | 14 (19.2) | 17 (18.9) | 19 (21.1) | 26 (28.9) | |
| Adequate | 27 (35.1) | 29 (32.6) | 28 (38.4) | 32 (35.6) | 36 (40.0) | 25 (27.8) | |
| Excessive | 33 (42.9) | 48 (53.9) | 29 (39.7) | 41 (45.6) | 34 (37.8) | 39 (43.3) | |
| Dietary supplements intake 1 | 0.028 * | ||||||
| Yes | 5 (6.5) | 13 (14.6) | 17 (23.3) | 17 (18.9) | 22 (24.4) | 13 (14.4) | |
| No | 72 (93.5) | 76 (85.4) | 56 (76.7) | 73 (81.1) | 68 (75.6) | 77 (85.6) | |
| Pregnancy duration, weeks 2 | 39 (38–40) | 39 (39–40) | 39 (38–40) | 39 (38–40) | 39.5 (39–40) | 40 (39–40) | 0.332 |
| 0–4 Days (n = 77) | 5–11 Days (n = 89) | 12–30 Days (n = 73) | 31–60 Days (n = 90) | 61–120 Days (n = 90) | 121–240 Days (n = 90) | p-Value 1 | Post hoc Test 2 | |
|---|---|---|---|---|---|---|---|---|
| β-carotene | 8.0 (4.7–15.2) | 2.8 (2.0–4.4) | 2.1 (1.4–3.1) | 1.7 (1.3–3.0) | 1.9 (1.4–2.7) | 1.8 (1.4–2.6) | <0.001 * | P1 > P2 > P3 = P4 = P5 = P6 |
| β-cryptoxanthin | 6.2 (2.4–12.9) | 3.4 (1.7–5.7) | 2.4 (1.1–3.9) | 1.7 (1.1–2.6) | 1.8 (1.0–4.0) | 2.1 (1.1–3.7) | <0.001 * | P1 > P2 > P3 = P4 = P5 = P6 |
| Lutein | 5.7 (2.9–10.2) | 7.0 (4.6–10.3) | 2.2 (1.2–6.3) | 2.9 (0.9–5.9) | 2.8 (1.2–6.5) | 3.7 (2.4–5.9) | <0.001 * | P1 = P2 > P3 =P4 = P5 = P6 |
| Lycopene | 6.3 (4.0–9.9) | 2.5 (1.7–4.3) | 1.8 (1.2–2.6) | 1.4 (1.1–2.0) | 1.4 (1.0–2.0) | 1.5 (1.3–2.0) | <0.001 * | P1 > P2 > P3 = P4 = P5 = P6 |
| Zeaxanthin | 1.0 (0.6–1.5) | 1.4 (1.0–2.2) | 0.8 (0.4–1.5) | 0.8 (0.4–1.4) | 1.0 (0.4–1.4) | 1.1 (0.8–1.4) | <0.001 * | P2 > P1 = P3 = P4 = P5 = P6 |
| α-tocopherol | 645 (388–1176) | 382 (236–551) | 239 (145–396) | 206 (126–345) | 212 (112–300) | 211 (135–326) | <0.001 * | P1 > P2 > P3 = P4 = P5 = P6 |
| γ-tocopherol | 68 (48–121) | 63 (43–103) | 70 (39–104) | 73 (41–120) | 68 (39–112) | 88 (56–137) | <0.033 * | P2 = P3 < P6; P1 = P4 = P5 = P6 |
| Beijing (n = 151) | Suzhou (n = 180) | Guangzhou (n = 178) | p-Value 1 | Post hoc Test 2 | |
|---|---|---|---|---|---|
| B-carotene | 1.7 (1.3–3.2) | 2.4 (1.7–4.3) | 2.7 (1.7–5.0) | <0.001 * | C1 < C2 = C3 |
| β-cryptoxanthin | 1.1 (0.8–2.0) | 3.6 (2.1–7.7) | 2.8 (1.7–5.2) | <0.001 * | C1 < C3 < C2 |
| Lutein | 2.2 (1.0–4.1) | 4.9 (2.6–7.9) | 5.8 (2.9–8.7) | <0.001 * | C1 < C2 = C3 |
| Lycopene | 1.7 (1.3–2.8) | 1.7 (1.3–2.7) | 2.1 (1.4–3.8) | 0.006 * | C1 = C2 < C3 |
| Zeaxanthin | 0.8 (0.4–1.4) | 1.1 (0.7–2.0) | 1.1 (0.7–1.5) | <0.001 * | C1 < C2 = C3 |
| α-tocopherol | 215 (117–333) | 296 (208–478) | 285 (148–479) | <0.001 * | C1 < C2 = C3 |
| γ-tocopherol | 71 (48–107) | 94 (59–148) | 53 (31–88) | <0.001 * | C3 < C1 < C2 |
| β-carotene | β-cryptoxanthin | Lutein | Zeaxanthin | |||||
|---|---|---|---|---|---|---|---|---|
| Adjusted 1 β (95% CI) | SEM | Adjusted 1 β (95% CI) | SEM | Adjusted 1 β (95% CI) | SEM | Adjusted 1 β (95% CI) | SEM | |
| Age, years | ||||||||
| <25 | −0.05 (−0.18, 0.08) | 0.07 | 0.11 (−0.06, 0.28) | 0.09 | −0.13 (−0.35, 0.08) | 0.11 | −0.01 (−0.14, 0.15) | 0.07 |
| 25–30 | Reference | Reference | Reference | Reference | ||||
| >30 | 0.10 (−0.03, 0.23) | 0.07 | 0.11 (−0.07, 0.29) | 0.09 | −0.03 (−0.15, 0.19) | 0.11 | 0.12 (−0.03, 0.27) | 0.08 |
| Education | ||||||||
| Middle school or below | Reference | Reference | Reference | Reference | ||||
| High school | 0.03 (−0.11, 0.17) | 0.07 | −0.18 (−0.36, 0.01) | 0.09 | 0.12 (−0.11, 0.35) | 0.12 | −0.14 (−0.30, 0.02) | 0.08 |
| College or above | 0.09 (−0.04, 0.23) | 0.07 | −0.12 (−0.30, 0.06) | 0.09 | 0.08 (−0.14, 0.31) | 0.11 | −0.15 (−0.31, −0.00) * | 0.08 |
| Delivery mode | 0 | |||||||
| Vaginal delivery | 0.04 (−0.07, 0.15) | 0.05 | 0.03 (−0.11, 0.17) | 0.07 | 0.14 (−0.04, 0.31) | 0.09 | 0.13 (0.02, 0.25) * | 0.06 |
| Cesarean delivery | Reference | Reference | Reference | Reference | ||||
| Current BMI | 0 | |||||||
| Underweight | 0.01 (−0.25, 0.26) | 0.13 | −0.02 (−0.35, 0.32) | 0.17 | 0.32 (−0.09, 0.74) | 0.21 | 0.29 (0.01, 0.57) * | 0.14 |
| Normal | Reference | Reference | Reference | Reference | ||||
| Overweight | −0.17 (−0.29, −0.05) * | 0.06 | −0.16 (−0.32, 0.00) | 0.08 | −0.11 (−0.31, 0.09) | 0.10 | −0.07 (−0.21, 0.07) | 0.07 |
| Obesity | −0.24 (−0.54, 0.07) | 0.16 | −0.16 (−0.57, 0.24) | 0.21 | 0.16 (−0.34, 0.66) | 0.26 | −0.18 (−0.52, 0.16) | 0.17 |
| β-carotene | β-cryptoxanthin | Lutein | Lycopene | Zeaxanthin | α-tocopherol | γ-tocopherol | ||
|---|---|---|---|---|---|---|---|---|
| Dietary intake of vitamin A | R | 0.022 | 0.026 | 0.027 | −0.007 | 0.075 | - | - |
| p 1 | 0.618 | 0.562 | 0.537 | 0.881 | 0.093 | - | - | |
| Dietary intake of total carotenoids | R | 0.055 | 0.002 | 0.007 | −0.038 | 0.003 | - | - |
| p 1 | 0.220 | 0.963 | 0.880 | 0.398 | 0.948 | - | - | |
| Dietary intake of vitamin E | R | - | - | - | - | - | −0.083 | 0.006 |
| p 1 | - | - | - | - | - | 0.063 | 0.885 | |
| Dietary intake of α-tocopherol | R | - | - | - | - | - | −0.033 | −0.084 |
| p 1 | - | - | - | - | - | 0.456 | 0.058 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, Y.; Campos-Giménez, E.; Redeuil, K.M.; Lévèques, A.; Actis-Goretta, L.; Vinyes-Pares, G.; Zhang, Y.; Wang, P.; Thakkar, S.K. Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study. Nutrients 2017, 9, 1229. https://doi.org/10.3390/nu9111229
Xue Y, Campos-Giménez E, Redeuil KM, Lévèques A, Actis-Goretta L, Vinyes-Pares G, Zhang Y, Wang P, Thakkar SK. Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study. Nutrients. 2017; 9(11):1229. https://doi.org/10.3390/nu9111229
Chicago/Turabian StyleXue, Yong, Esther Campos-Giménez, Karine Meisser Redeuil, Antoine Lévèques, Lucas Actis-Goretta, Gerard Vinyes-Pares, Yumei Zhang, Peiyu Wang, and Sagar K. Thakkar. 2017. "Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study" Nutrients 9, no. 11: 1229. https://doi.org/10.3390/nu9111229
APA StyleXue, Y., Campos-Giménez, E., Redeuil, K. M., Lévèques, A., Actis-Goretta, L., Vinyes-Pares, G., Zhang, Y., Wang, P., & Thakkar, S. K. (2017). Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study. Nutrients, 9(11), 1229. https://doi.org/10.3390/nu9111229