Update on Immunohistochemistry for the Diagnosis of Lung Cancer


Division of Pathology, The Cancer Institute, Japanese Foundation for Cancer Research, 3-8-31 Ariake, Koto-ku, Tokyo 135-8550, Japan
Cancers 2018, 10(3), 72; https://doi.org/10.3390/cancers10030072
Submission received: 3 February 2018
/
Revised: 9 March 2018
/
Accepted: 13 March 2018
/
Published: 14 March 2018
(This article belongs to the Special Issue Immunohistochemistry and Cancer Diagnosis)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Immunohistochemistry is a widely available technique that is less challenging and can provide clinically meaningful results quickly and cost-efficiently in comparison with other techniques. In addition, immunohistochemistry allows for the evaluation of cellular localization of proteins in the context of tumor structure. In an era of precision medicine, pathologists are required to classify lung cancer into specific subtypes and assess biomarkers relevant to molecular-targeted therapies. This review summarizes the hot topics of immunohistochemistry in lung cancer, including (i) adenocarcinoma vs squamous cell carcinoma; (ii) neuroendocrine markers; (iii) ALK, ROS1, and EGFR; (iv) PD-L1 (CD274); (v) lung carcinoma vs malignant mesothelioma; and (vi) NUT carcinoma. Major pitfalls in evaluating immunohistochemical results are also described.
1. Introduction
In an era of precision medicine, immunohistochemistry plays a critical role in the classification of tumors into subtypes and for assessing biomarkers for timely and accurate therapeutic decision-making [1,2,3,4,5]. Compared with other techniques, immunohistochemistry has a number of advantages, including being widely available, technically less challenging, and cost-efficient with a rapid turn-around time. Thus, molecular-specific immunohistochemical assays have huge potential as practical screening tools for the detection of druggable genetic alterations and for the assessment of biomarkers for molecular-targeted therapy. In addition, immunohistochemistry can be interpreted using fewer tumor cells than are required for other molecular techniques. Moreover, immunohistochemistry allows for the evaluation of cellular localization and staining patterns in the context of tumor structures; thus, a greater range of information is provided.
Lung cancer is the leading cause of cancer-related deaths worldwide, regardless of gender. It is categorized into two main groups: small cell lung carcinoma (SCLC, 15% of all lung cancers) and non-SCLC (NSCLC, 85% of all lung cancers). Accumulating evidence suggests that lung cancer represents a group of histologically and molecularly heterogeneous diseases [6,7,8,9,10,11,12,13,14,15,16,17]. In addition, increasing knowledge of the molecular pathology of lung cancers has led to their classification into specific subtypes according to appropriate treatments and molecular-targeted therapies. This review provides updated knowledge of the use of immunohistochemistry in lung cancer. Hot topics of immunohistochemistry in lung cancer are discussed, including (i) the differential diagnosis between adenocarcinoma and squamous cell carcinoma (SqCC); (ii) neuroendocrine markers; (iii) driver genetic alterations (ALK, ROS1, and EGFR); (iv) PD-L1 (CD274) expression; (v) the differential diagnosis between lung carcinoma and malignant mesothelioma; and (vi) NUT carcinoma. Major pitfalls in correctly evaluating immunohistochemical results are also described.
2. Adenocarcinoma vs. Squamous Cell Carcinoma
The 2015 World Health Organization (WHO) classification was recently modified based on newly identified molecular profiles and druggable genetic alterations in lung cancer [6]. In particular, the 2011 International Association for the Study of Lung Cancer (IASLC), the American Thoracic Society, and the European Respiratory Society classification [18] was mostly adopted in the current WHO classification for lung adenocarcinoma. Advancements in oncology, molecular biology, pathology, radiology, and surgery were considered for the classification of lung cancer into specific subtypes with the aid of immunohistochemistry for therapeutic purposes. In older WHO classifications, the definition of lung cancer subtypes was based on surgical specimens; however, the current WHO categorization is based on small biopsy and cytology specimens, which need to be diagnosed with the help of immunohistochemistry as most lung cancers are detected at later stages.
When possible, differential diagnosis between adenocarcinoma and SqCC is beneficial because targetable driver genetic alterations are mostly identified in adenocarcinoma, and inappropriate drugs need to be avoided for patients with SqCC. Before the 2015 WHO classification, the definitions of adenocarcinoma and SqCC were based on their morphological features with or without mucin staining. Adenocarcinoma was defined as carcinoma with an acinar/tubular structure or mucin production, whereas SqCC was defined as carcinoma with keratinization or intercellular bridges. In the current classification, a solid carcinoma without glandular structures or mucin production, but with immunohistochemical positivity for “adenocarcinoma markers”, i.e., TTF-1 (NKX2-1) and/or Napsin A, is diagnosed as an adenocarcinoma. Similarly, a solid carcinoma without keratinization or intercellular bridges, but with immunohistochemical positivity for “SqCC markers”, such as p40, CK5/6, and TP63 (p63), is diagnosed as SqCC. These modifications using immunohistochemical evaluations have markedly minimized the proportion of NSCLC diagnosed as large cell carcinoma [19].
There exist several pitfalls in differential diagnosis between adenocarcinoma and SqCC [20,21,22]. While performing a differential diagnosis between adenocarcinoma and SqCC using an anti-TTF-1 antibody, a clone of the antibody should be paid attention to. SPT24 and 8G7G3/1 are major clones of the anti-TTF-1 antibody. Whereas TTF-1 (clone SPT24) is less specific (positive in 17% of SqCC) but more sensitive (positive in 72‒84%), TTF-1 (clone 8G7G3/1) is more specific (positive in 1% of SqCC) but less sensitive (positive in 65‒77%) for adenocarcinoma when differentiated from SqCC [21,23,24,25]. Among “SqCC markers”, p40 is the best marker in terms of specificity (positive in 3% of adenocarcinoma) and sensitivity (positive in 100%) [26]. Conversely, TP63 is sensitive (positive in 100%) but less specific (positive in 31% of adenocarcinoma) [26]. Collectively, it should be noted that a significant number of SqCCs or adenocarcinomas show a positivity for TTF-1 (clone SPT24) or TP63, respectively. As another pitfall, trapped benign pneumocytes (positive for TTF-1 and Napsin A) and tumor-infiltrated macrophages (positive for Napsin A) should not be misinterpreted.
3. Neuroendocrine Markers
In the 2015 WHO classification [6], the category of “neuroendocrine tumors” was newly recognized. Invasive neuroendocrine tumors comprise three subtypes: SCLC, large cell neuroendocrine carcinoma (LCNEC), and carcinoid tumor (typical/atypical). Although high-grade neuroendocrine tumors (HGNETs), comprising SCLCs and LCNECs, belong to the same category as carcinoid tumors, their clinical characteristics are substantially different. HGNET is an aggressive and deadly subtype characterized by patients with a history of heavy smoking. In contrast, carcinoid tumors usually follow a benign clinical course and frequently occur in patients without a history of smoking. Despite their different clinical characteristics, these tumors share the features of neuroendocrine differentiation. As the definition of LCNEC in the WHO classification, the diagnosis of LCNEC requires not only neuroendocrine morphology but also immunohistochemical expression of at least one of the three neuroendocrine markers, i.e., CHGA (chromogranin A), SYP (synaptophysin), or NCAM1 (CD56).
Neuroendocrine differentiation of lung tumors is orchestrated by complex pathways as concisely displayed in Figure 1 [27,28]. The NOTCH1-HES1 signaling pathway represses neuroendocrine differentiation by inactivating INSM1 and ASCL1. INSM1 is a zinc-finger transcriptional factor originally isolated from pancreatic insulinomas [29]. NOTCH1 activates HES1, which inactivates INSM1 and ASCL1. INSM1 promotes the expression of the three neuroendocrine molecules (CHGA, SYP, and NCAM1) via the activation of the transcription factors ASCL1 and BRN2. HES1 is a known transcriptional repressor of ASCL1.
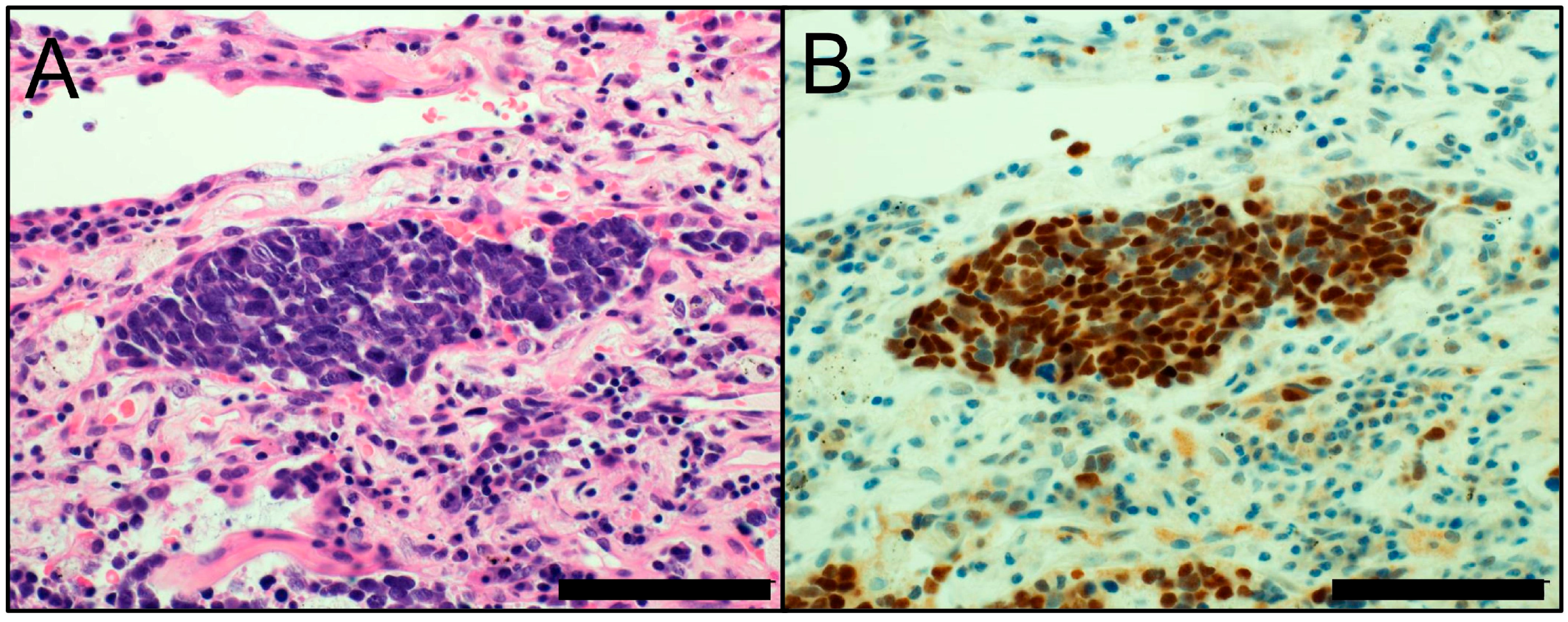
A recent study demonstrated that INSM1 was positive in 94.9% of SCLCs and 91.3% of LCNECs, compared with 74.4% and 78.3% with the combined panel of the three neuroendocrine markers (CHGA, SYP, and NCAM1). Thus, INSM1 was suggested to be more useful than the individual or combined use of CHGA, SYP, and NCAM1 for the diagnosis of lung HGNETs [30]. INSM1 appears to be a novel, sensitive, and specific immunohistochemical marker that may serve as a standalone first-line marker of neuroendocrine differentiation (Figure 2).
4. ALK, ROS1, and EGFR
Various somatic genetic alterations in tyrosine kinase have emerged as druggable molecular targets by tyrosine kinase inhibitors (TKIs), particularly in lung adenocarcinoma [31]. With a prudent evaluation of genetic-alteration-specific immunostaining, immunohistochemistry has enormous potential to be used as a practical screening tool to detect certain actionable genetic alterations amenable to molecular-targeted therapies.
ALK-rearranged lung adenocarcinoma, comprising 4‒5% of lung adenocarcinomas, is clinicopathologically characterized by a TTF-1 cell lineage, an acinar structure with mucin/signet-ring cell morphology, non-/light-smoking history, and young onset [32,33,34,35]. Various clinical trials have demonstrated the clinical efficacy of TKIs or ALK inhibitors in patients with ALK-rearranged NSCLC [36,37,38]. Immunohistochemistry for ALK represents a cost-effective and widely available method that is an effective screening tool to detect the presence of ALK rearrangement, in addition to conventional fluorescence in situ hybridization (FISH) [39]. According to recent studies, ALK antibody clones D5F3 and 5A4 show the highest sensitivity and specificity compared with several available anti-ALK antibodies [40]. Recently, the U.S. Food and Drug Administration (FDA) approved an immunohistochemical assay using the ALK D5F3 antibody as a companion diagnostic assay for patients with ALK-rearranged NSCLC. Therefore, patients with ALK-positive NSCLC, as confirmed by immunostaining using clone D5F3, are candidates for ALK inhibitor treatment. Of note, immunohistochemistry using the ALK D5F3 antibody appears to be not only a candidate but also the most important test for ALK testing. There are several studies suggesting the superiority of the ALK immunohistochemistry with the D5F3 antibody compared with ALK FISH at predicting response to ALK inhibitors [41,42,43,44].
Immunohistochemically, ALK-rearranged lung cancers show cytoplasmic ALK staining. Intracellular mucin vacuoles are frequently observed in ALK-rearranged adenocarcinoma; thus, inadequate cytoplasmic immunostaining can cause these to be carelessly missed (Figure 3). In addition, nonspecific immunostaining can be observed in some neuroendocrine carcinomas without ALK rearrangement [2].
ROS1 rearrangement is an oncogenic driver in a subset (1‒2%) of lung adenocarcinomas [45,46,47]. ROS1-rearranged adenocarcinoma is clinicopathologically characterized by solid growth with signet-ring cells or a cribriform morphology with abundant extracellular mucus, and typically occurs in younger non-smoking females [48]. Clinical trials have demonstrated the clinical efficacy of TKIs or ROS1 inhibitors in patients with NSCLC with ROS1 rearrangement confirmed by FISH assays [47,49]. As with ALK-rearranged NSCLCs, immunohistochemistry provides high sensitivity and specificity for the detection of ROS1 rearrangements. Immunohistochemical assay using the specific rabbit monoclonal antibody clone D4D6 is a cost-efficient and widely available method for screening patients with ROS1-rearranged NSCLCs [50,51]. However, there is no benign tissue that can be used as a positive control for ROS1. This contrasts with ALK, where ganglion cells and nerves of the appendix can be used as a positive control. Therefore, tumors or cell lines with confirmed ROS1 rearrangement need to be used as an external positive control [52]. Further, the ROS1 staining pattern depends on the partner genes of ROS1 fusion. Adenocarcinomas with CD74-ROS1 fusion, which is the most frequent fusion gene, usually shows globular cytoplasmic ROS1 immunoreactivity, whereas adenocarcinomas with EZR-ROS1 fusion usually show membranous immunostaining [48]. Similar to ALK-rearranged adenocarcinomas, an intracellular mucin vacuole is frequently observed in ROS1-rearranged adenocarcinomas; therefore, inadequate immunostaining should not be missed. It should be also noted that benign hyperplastic pneumocytes and macrophages frequently show weak ROS1 immunostaining [53]. Furthermore, the possibility of false-positive tumors in ever-smoking patients has been suggested [54]. Currently, screening by immunohistochemistry for ROS1, followed by the subsequent confirmation of ROS1-positive cases by FISH, is required. TKIs or ROS1 inhibitors should be applied only to cases that are positive for ROS1 rearrangement, as confirmed by both immunohistochemical and FISH analyses [2].
The EGFR mutation is one of the most common driver mutations in lung adenocarcinoma, and EGFR-mutated adenocarcinoma is characterized by East Asian ethnicity, female gender, and non-/light-smoking history [55]. Pathologically, EGFR-mutated lung adenocarcinoma typically shows nuclear TTF-1 immunoreactivity and hobnail cell morphology. In addition, adenocarcinoma with micropapillary morphology has a higher frequency of EGFR mutations than adenocarcinoma without this morphology [56]. In the gene coding for the receptor, EGFR mutations are divided into four major types: point mutations in exon 18, deletions in exon 19, insertions in exon 20, and point mutations in exon 21. Approximately 90% of EGFR mutations in NSCLCs involve in-frame deletions in exon 19 and the point mutation L858R in exon 21. These mutations, particularly exon 19 deletions, are associated with a superior and prolonged clinical response to EGFR TKIs [57,58]. EGFR mutation-specific antibodies, recognizing a 15-bp deletion in exon 19 (clone: 6B6) and an L858R point mutation in exon 21 (clone: 43B2), have been developed [59]. However, immunohistochemical analysis using these antibodies has not been recommended for screening EGFR mutations due to its low sensitivity.
5. PD-L1 (CD274)
PD-L1 (CD274) is an immune modulator that promotes immunosuppression by binding to PD-1 (PDCD1). PD-L1 on the surface of tumor cells inhibits an immune-mediated attack by binding to PD-1 on cytotoxic T-cells [60,61]. Although various studies have reported the association of PD-L1 positivity in tumor cells with prognosis in lung cancer, the results are conflicting and inconclusive [62,63,64,65,66,67,68,69,70]. A possible reason for the discordant results lies in cohort-dependent non-standardized immunohistochemical assays. Another possible reason is that the association of PD-L1 positivity with clinical outcome truly differs depending on the cohorts. Anti-PD-1/PD-L1 antibodies inhibit PD-L1 binding to PD-1, thus allowing immune-mediated attacks against tumor cells at this immune checkpoint. Multiple clinical trials using these antibodies for the treatment of malignancies, including NSCLCs, have shown great promise in prolonging survival [71,72,73]. According to a clinical trial for PD-1 inhibitor, pembrolizumab, for the treatment of NSCLCs [74], NSCLCs with at least 50% positivity for PD-L1 were associated with a higher response rate and longer survival than NSCLCs with less than 50% positivity. Of importance, although a response rate is lower than NSCLCs with at least 50% positivity for PD-L1, a certain subset of NSCLCs with less than 1% positivity still responded to pembrolizumab. Given this result, there remains an urgent need for the identification of more reliable biomarkers that predict the responsiveness to immune checkpoint inhibitors.
Specific immunohistochemical assays for different PD-1/PD-L1 inhibitors have been designed to estimate sensitivities to these treatments [75]. Currently, there are five different PD-1/PD-L1 inhibitors that require specific immunohistochemical assays using different anti-PD-L1 antibodies. These include nivolumab with clone 28-8, pembrolizumab with clone 22C3, atezolizumab with clone SP142, durvalumab with clone SP263, and avelumab with clone 73-10 [60,76,77,78]. For assays using the 22C3, 28-8, SP263, and 73-10, complete circumferential or partial membranous immunostaining of any intensity is considered to be positive. In an assay using the SP142, the presence of PD-L1-positive immune cells is also considered while determining the PD-L1 positivity. The U.S. FDA has currently approved a companion diagnostic PD-L1 test for pembrolizumab (assay using the 22C3 antibody) and the complementary diagnostic PD-L1 tests for nivolumab (assay using the 28-8 antibody) and atezolizumab (assay using the SP142 antibody), whereas clinical trials with the two agents durvalumab (assay using the SP263 antibody) and avelumab (assay using the 73-10 antibody) have also demonstrated promising results [3,79,80,81]. The requirement for different kits, instruments, and interpretative criteria for each drug is challenging for pathology laboratories and pathologists. To know whether one of these assays can be used to select eligible patients for anti-PD-1/PD-L1 inhibitors, comparisons of the difference among these assays have been made by several studies [82,83,84,85,86] including the Blueprint project [82], which is an industrial–academic collaborative partnership among the IASLC and the American Association for Cancer Research, pharmaceutical companies, and diagnostics venders. According to these studies, the 22C3, 28-8, and SP263 assays showed a similar membranous staining on tumor cells; however, the SP142 assay consistently had fewer PD-L1 tumor cells expressing PD-L1. As for the PD-L1 expression on immune cells, low concordance rates were observed among these assays, indicating a requirement for specific standardization of immune cell scoring.
As an external positive control for PD-L1, human tonsils, placenta, or PD-L1-positive cell lines can be used. In addition, at least 100 viable tumor cells need to present in one PD-L1-immunostained slide to determine the percentage of PD-L1-positive cells. Of note, the careful observation of both hematoxylin-eosin (HE)-stained slides and immunostained slides is required to correctly evaluate PD-L1 positivity, as PD-L1 can be immunostained in inflammatory cells, including macrophages and lymphocytes. When PD-L1-positive macrophages and/or lymphocytes exist around PD-L1-negative tumor cells, misinterpretation should be carefully avoided. In addition, tumor cells with cytoplasmic granular immunostaining, but without membranous staining, should not be misinterpreted as positive [2,3].
6. Lung Carcinoma vs. Malignant Mesothelioma
Malignant mesothelioma (MM) is a rare and fatal malignant tumor arising from mesothelial cells. Malignant mesothelioma is one of the important tumors that need to be distinguished from lung cancer while diagnosing lung cancer. Asbestos exposure is the main risk factor for developing MMs, which are generally classified into three major histologic subtypes: epithelioid (60–80%), sarcomatoid (<10%), and biphasic (10–15%). Epithelioid MM is the most common subtype and shows a relatively better prognosis than sarcomatoid or biphasic MM [6]. MM needs to be diagnosed based on the patient’s clinical and radiologic findings in conjunction with morphological and immunohistochemical features. The differential diagnoses between MM and benign mesothelial proliferation, as well as between MM and lung carcinoma, are sometimes challenging.
Reactive mesothelial proliferations occasionally mimic MMs, because reactive mesothelial proliferations sometimes exhibit cellular and structural atypia typically observed in MMs. Therefore, differential diagnosis between MM and reactive mesothelial proliferation is often difficult. The loss of BAP1, confirmed by immunohistochemistry, and homozygous CDKN2A (p16) deletions, identified by FISH, have recently emerged as potential indicators of MM. Loss of nuclear BAP1 immunostaining is often observed in MMs, particularly the epithelioid/biphasic subtype, but not in active mesothelial proliferations. However, BAP1 loss is relatively uncommon in the sarcomatoid subtype. Therefore, BAP1 immunohistochemistry has a relatively high specificity, but low sensitivity [87,88,89]. In contrast to BAP1 loss, the CDKN2A deletion is observed more frequently in the sarcomatoid subtype than in the epithelioid/biphasic subtype [88,89,90].
Lung carcinomas can also show pseudomesotheliomatous spreads. As no immunohistochemical marker is completely specific for each type of tumor, the International Mesothelioma Interest Group recommends at least two mesothelial and two carcinoma markers, in addition to cytokeratins, to be included in the differential diagnosis between MM and carcinoma. Mesothelial markers include calretinin (nuclear and cytoplasmic staining), podoplanin (clone D2-40; membranous staining), CK5 or CK5/6 (cytoplasmic staining), and WT1 (nuclear staining) [91]. For differential diagnosis between MM and lung adenocarcinoma, TTF-1, Napsin A, CEA, claudin 4 (CLDN4), Ber-EP4, and MOC31 are useful markers suggesting lung adenocarcinoma. A recent study has demonstrated that the positive rates of DAB2 and Intelectin-1 (INLT1) expression were 80% and 76% in epithelioid MM, and 3% and 0% in lung adenocarcinoma, respectively. This study indicates that DAB2 and Intelectin-1 are novel positive immunohistochemical markers of epithelioid MM, and should allow for its differentiation from lung adenocarcinoma [92]. For sarcomatoid MM, a recent study has suggested MUC4 as a novel negative immunohistochemical marker of sarcomatoid MM for its differentiation from lung sarcomatoid carcinoma [93].
Collectively, immunohistochemistry plays an essential role in the differential diagnosis of MM; thus, the appropriate selection of immunohistochemical markers is essential. Morphological, clinical, and radiological features are also needed for correct diagnosis.
7. NUT Carcinoma
NUT carcinoma has been recently recognized as a subtype of lung cancer in the 2015 WHO classification [6]. Because NUT carcinoma is frequently misdiagnosed as different malignancy, it needs to be considered in the differential diagnosis of malignancies in lung. NUT carcinoma is defined by a gene rearrangement between the NUT (NUTM1) gene on chromosome 15q14 and one of the other partner genes. The NUT gene is fused to the bromodomain family member BRD3 on chromosome 19p13.1 (comprising 70% of NUT carcinomas), BRD4 on chromosome 9q (6%), or the other partner genes. The methyltransferase NSD3 on chromosome 8q11.23 was newly recognized as a fusion partner of NUT [6,94,95,96,97,98,99]. These rearrangements lead to global epigenetic reprogramming and loss of cell differentiation [98,99,100]. Although NUT carcinoma occasionally exhibits abrupt foci of keratinization in morphology, NUT carcinomas show few cytogenetic alterations with the exception of chromosomal translocation involving NUT. This contrasts with lung SqCCs, which are characterized by complex and multiple cytogenetic alterations [6,100]. In terms of the simple cytogenetic alterations, NUT carcinomas closely resemble hematological tumors, which are similarly characterized by simple cytogenetic alterations.
Clinically, NUT carcinoma shows an extremely aggressive behavior with dismal prognosis, and a median overall survival of 2.2 months. NUT carcinoma occurs with no predominance of gender, and affects people of any age and smoking history, although it was originally reported in young individuals [6,94,101]. Although NUT carcinoma lacks benefit from chemotherapy or radiotherapy [94,98], molecular-targeted therapies against bromodomain may be beneficial as either a single agent or in combination with other agents [102,103].
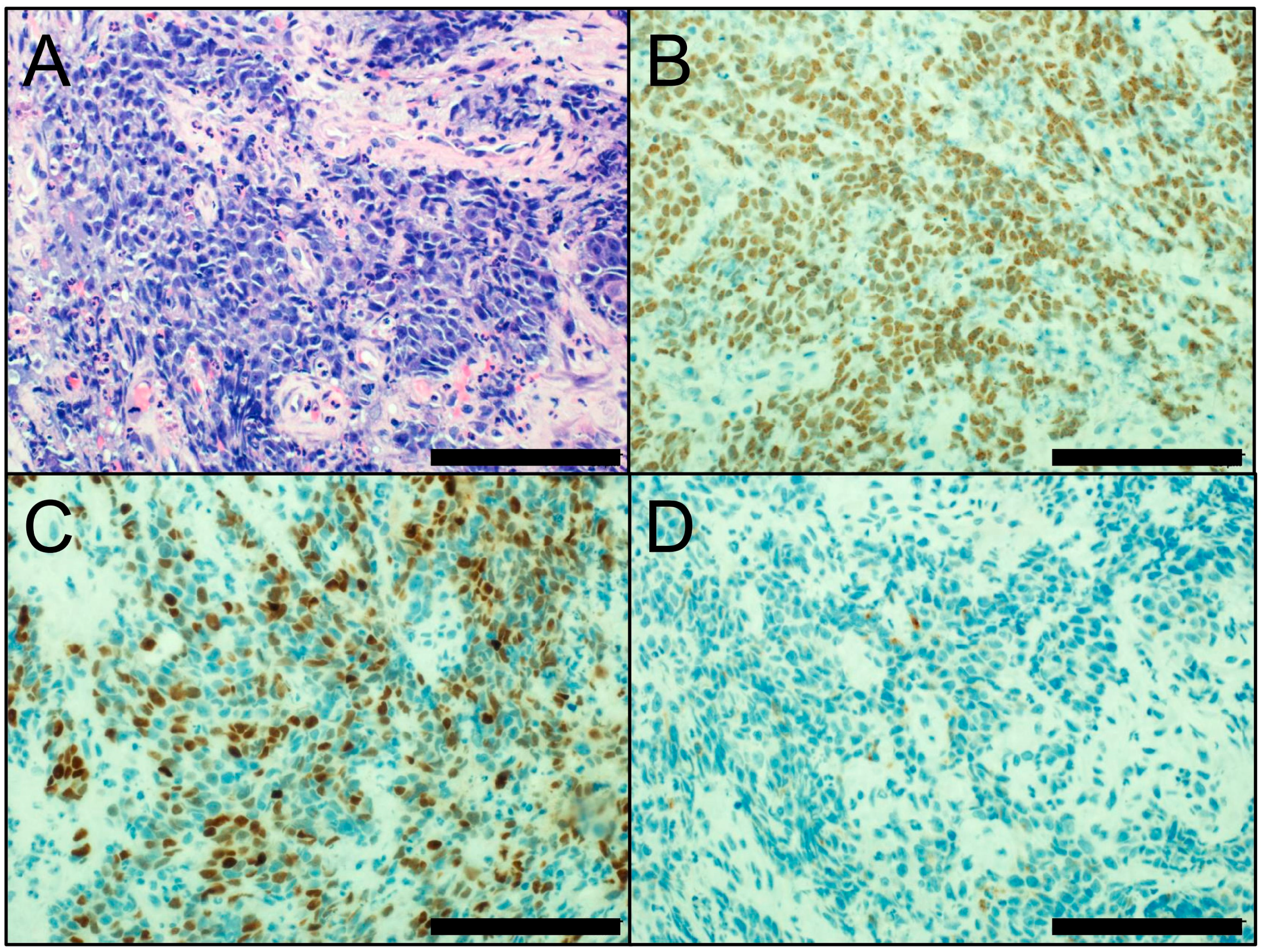
Morphologically, NUT carcinoma is characterized by sheets and nests of small- to intermediate-sized monotonous, primitive-appearing tumor cells (Figure 4A), with the occasional abrupt foci of keratinization. The lack of a pathognomonic appearance leads to the frequent misdiagnosis of NUT carcinoma as basaloid SqCC, SCLC, lymphoma, or germ cell tumor [6,94,101].
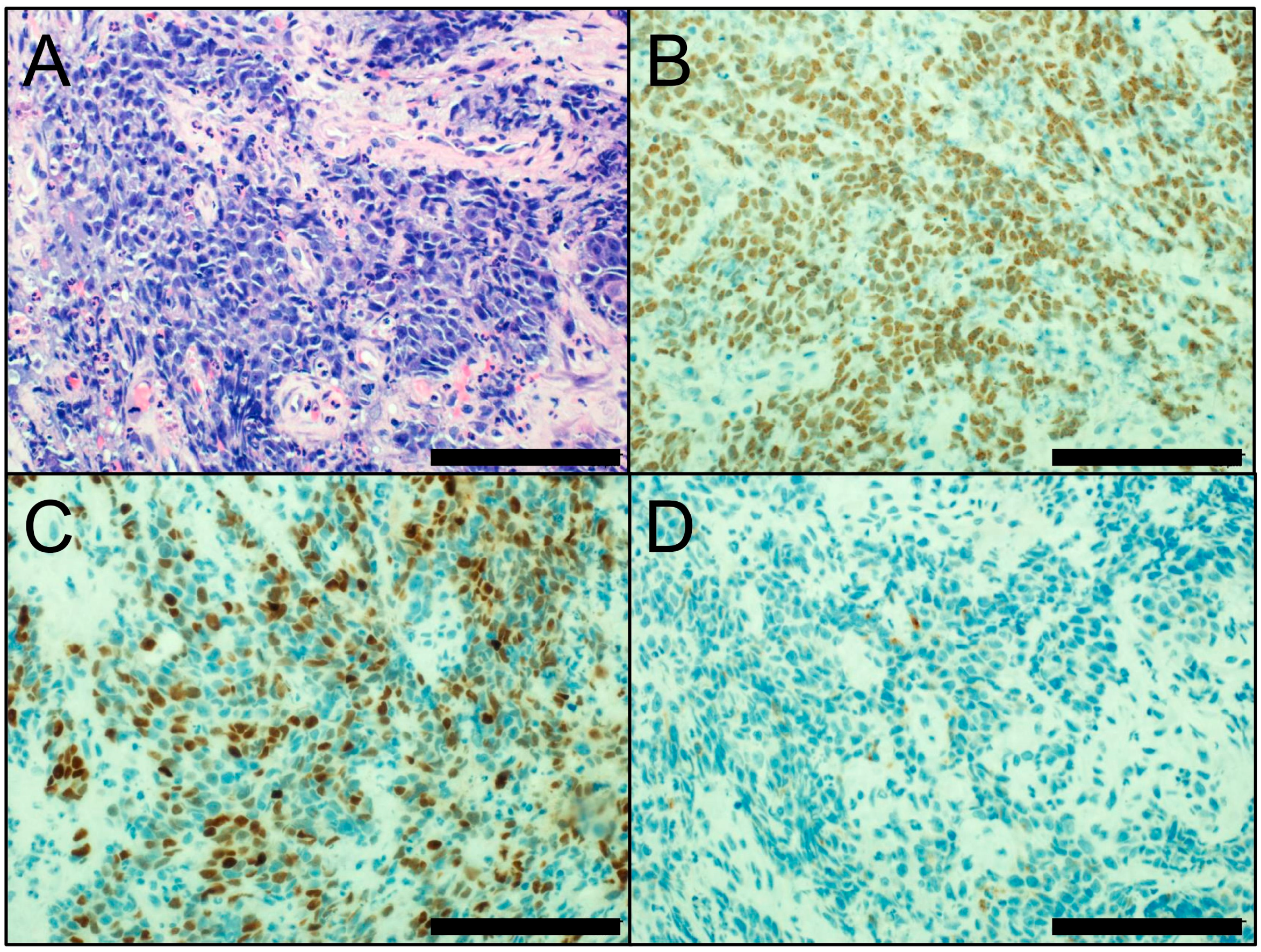
Immunohistochemical detection of the nuclear NUT protein facilitates a rapid and cost-effective diagnosis of NUT carcinoma, with the aid of highly specific and sensitive monoclonal NUT antibodies [104]. NUT carcinoma typically shows speckled nuclear positivity for NUT (Figure 4B). Both morphological and immunohistochemical features contribute to the correct diagnosis of NUT carcinoma. Because seminomas may show weak and focal NUT immunostaining, careful observation of the NUT staining pattern is required [105]. In addition, NUT carcinoma is usually positive for broad-spectrum cytokeratins and often shows nuclear staining for p40, suggesting lineage from SqCC (Figure 4C) [106]. Due to its morphological and immunohistochemical similarities with basaloid SqCC, it is important that NUT carcinoma not be diagnosed as basaloid SqCC. NUT carcinoma can be immunostained for the neuroendocrine markers CHGA and SYP (Figure 4D). In addition, because NUT carcinoma shares morphological similarity (small- to intermediate-sized monotonous appearances and crush artifacts) and neuroendocrine differentiation with SCLC, a misdiagnosis as SCLC should be avoided. Immunohistochemical assessment of NUT nuclear expression needs to be considered in cases of poorly differentiated carcinomas, particularly in young patients without a history of smoking [6,94,101].
8. Conclusions and Future Directions
Immunohistochemical techniques play critical roles as diagnostic and screening tools for lung cancer. However, the limitations of immunohistochemistry should be fully apprehended to avoid inappropriate results from immunohistochemical assays [2,107]. The results of immunohistochemical assays are affected by variable pre-analytical handling of the specimen, including delay in fixation, inappropriate fixation time, inappropriate fixative solution, and issues regarding paraffin embedding [108]. The immunohistochemical results are also influenced by analytic variables, including antigen retrieval, concentration of the antibody, incubation time/temperature, and signal enhancement. There also exists a problem of inter- and intra-observer variability in evaluating immunostainings. Although digital pathology has a potential to overcome subjectivity and improve reproducibility, the capability of digital pathology remains impractical in most cases. The immunostaining data still require interpretation by experienced pathologists, who need to acquire proficiency in immunohistochemistry updates. Also, immunohistochemical evaluation should be performed concurrently with detailed observations of corresponding HE slides. Conversely, immunohistochemistry has several advantages in comparison with other assays, including as a cost-effective and widely available technique with a rapid turn-around time. Immunohistochemical assays can also be performed with fewer tumor cells, and they allow for the evaluation of cellular localization of proteins in the context of tumor structure. In the current WHO classification, immunohistochemical analysis is indispensable to the determination of lung cancer subtypes. Furthermore, immunohistochemical assays have been approved by the U.S. FDA as companion or complimentary diagnostic assays for molecular-targeted therapies. Moreover, an increasing number of targeted therapies will require immunohistochemical evaluation in order to determine the eligibility of patients for certain treatments. Thus, molecular-specific immunohistochemical assays will be performed more frequently to determine specific subtypes, make differential diagnoses, and evaluate relevant biomarkers in lung cancer. Collectively, as part of the current era of precision medicine, immunohistochemical techniques have great promise for improving the diagnosis and treatment of lung cancer.
Acknowledgments
The author thanks Tomoyo Kakita for her technical assistance and Yuki Takano and Chikako Yoshida for their secretarial expertise. This study was supported by JSPS KAKENHI Grant Number JP16K08679; and the Ministry of the Environment, Japan.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
| FDA | Food and Drug Administration |
| FISH | fluorescence in situ hybridization |
| HE | hematoxylin-eosin |
| HGNET | high-grade neuroendocrine tumor |
| IASLC | International Association for the Study of Lung Cancer |
| INSM1 | insulinoma-associated protein 1 |
| LCNEC | large cell neuroendocrine carcinoma |
| MM | malignant mesothelioma |
| NSCLC | non-small cell lung carcinoma |
| SCLC | small cell lung carcinoma |
| SqCC | squamous cell carcinoma |
| TKI | tyrosine kinase inhibitor |
| WHO | World Health Organization |
References
- Cagle, P.T.; Allen, T.C.; Bernicker, E.H.; Ge, Y.; Haque, A.; Barrios, R. Impact of recent developments in lung cancer on the practice of pathology. Arch. Pathol. Lab. Med. 2016, 140, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Thunnissen, E.; Allen, T.C.; Adam, J.; Aisner, D.L.; Beasley, M.B.; Borczuk, A.C.; Cagle, P.T.; Capelozzi, V.L.; Cooper, W.; Hariri, L.P.; et al. Immunohistochemistry of pulmonary biomarkers: A perspective from members of the pulmonary pathology society. Arch. Pathol. Lab. Med. 2018, 142. [Google Scholar] [CrossRef] [PubMed]
- Mino-Kenudson, M. Immunohistochemistry for predictive biomarkers in non-small cell lung cancer. Transl. Lung Cancer Res. 2017, 6, 570–587. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.S.; Reddy, O.L.; Koo, M.; Xiong, Y.; Li, F.; Xu, H. Application of Immunohistochemistry in the Diagnosis of Pulmonary and Pleural Neoplasms. Arch. Pathol. Lab. Med. 2017, 141, 1195–1213. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.; Ragazzi, M.; Tamagnini, I.; Mengoli, M.C.; Vincenzi, G.; Barbieri, F.; Piccioli, S.; Bisagni, A.; Vavala, T.; Righi, L.; et al. Does immunohistochemistry represent a robust alternative technique in determining drugable predictive gene alterations in non-small cell lung cancer? Curr. Drug Targets 2017, 18, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2015. [Google Scholar]
- The Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar]
- The Cancer Genome Atlas Research Network. Comprehensive genomic characterization of squamous cell lung cancers. Nature 2012, 489, 519–525. [Google Scholar]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretic, L.; Kong, G.; Leenders, F.; Lu, X.; Fernandez-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Peifer, M.; Fernandez-Cuesta, L.; Sos, M.L.; George, J.; Seidel, D.; Kasper, L.H.; Plenker, D.; Leenders, F.; Sun, R.; Zander, T.; et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 2012, 44, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.M.; Durinck, S.; Stawiski, E.W.; Poirier, J.T.; Modrusan, Z.; Shames, D.S.; Bergbower, E.A.; Guan, Y.; Shin, J.; Guillory, J.; et al. Comprehensive genomic analysis identifies SOX2 as a frequently amplified gene in small-cell lung cancer. Nat. Genet. 2012, 44, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.H.; Sholl, L.M.; Rojas-Rudilla, V.; Hall, D.L.; Shivdasani, P.; Garcia, E.P.; MacConaill, L.E.; Vivero, M.; Hornick, J.L.; Kuo, F.C.; et al. KRAS and NKX2-1 mutations in invasive mucinous adenocarcinoma of the lung. J. Thorac. Oncol. 2016, 11, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Polley, E.; Kunkel, M.; Evans, D.; Silvers, T.; Delosh, R.; Laudeman, J.; Ogle, C.; Reinhart, R.; Selby, M.; Connelly, J.; et al. Small Cell Lung Cancer Screen of Oncology Drugs, Investigational Agents, and Gene and microRNA Expression. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [PubMed]
- Thunnissen, E.; van der Oord, K.; den Bakker, M. Prognostic and predictive biomarkers in lung cancer. A review. Virchows Arch. 2014, 464, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Sabir, S.R.; Yeoh, S.; Jackson, G.; Bayliss, R. EML4-ALK Variants: Biological and Molecular Properties, and the Implications for Patients. Cancers 2017, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K. Diagnostic and Therapeutic Potential of MicroRNAs in Lung Cancer. Cancers 2017, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K. Lung Cancer: Understanding Its Molecular Pathology and the 2015 WHO Classification. Front. Oncol. 2017, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Rekhtman, N.; Ang, D.C.; Sima, C.S.; Travis, W.D.; Moreira, A.L. Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. Mod. Pathol. 2011, 24, 1348–1359. [Google Scholar] [CrossRef] [PubMed]
- Kadota, K.; Nitadori, J.; Rekhtman, N.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. Reevaluation and reclassification of resected lung carcinomas originally diagnosed as squamous cell carcinoma using immunohistochemical analysis. Am. J. Surg. Pathol. 2015, 39, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Micke, P.; Mattsson, J.S.; Djureinovic, D.; Nodin, B.; Jirstrom, K.; Tran, L.; Jonsson, P.; Planck, M.; Botling, J.; Brunnstrom, H. The Impact of the Fourth Edition of the WHO Classification of Lung Tumours on Histological Classification of Resected Pulmonary NSCCs. J. Thorac. Oncol. 2016, 11, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Matoso, A.; Singh, K.; Jacob, R.; Greaves, W.O.; Tavares, R.; Noble, L.; Resnick, M.B.; Delellis, R.A.; Wang, L.J. Comparison of thyroid transcription factor-1 expression by 2 monoclonal antibodies in pulmonary and nonpulmonary primary tumors. Appl. Immunohistochem. Mol. Morphol. 2010, 18, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Comperat, E.; Zhang, F.; Perrotin, C.; Molina, T.; Magdeleinat, P.; Marmey, B.; Regnard, J.F.; Audouin, J.; Camilleri-Broet, S. Variable sensitivity and specificity of TTF-1 antibodies in lung metastatic adenocarcinoma of colorectal origin. Mod. Pathol. 2005, 18, 1371–1376. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, D. A study of DeltaNp63 expression in lung non-small cell carcinomas. Am. J. Surg. Pathol. 2012, 36, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Teruya-Feldstein, J.; Westra, W.H.; Pelosi, G.; Travis, W.D.; Rekhtman, N. p40 (DeltaNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Mod. Pathol. 2012, 25, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Fujino, K.; Motooka, Y.; Hassan, W.A.; Ali Abdalla, M.O.; Sato, Y.; Kudoh, S.; Hasegawa, K.; Niimori-Kita, K.; Kobayashi, H.; Kubota, I.; et al. Insulinoma-Associated Protein 1 Is a Crucial Regulator of Neuroendocrine Differentiation in Lung Cancer. Am. J. Pathol. 2015, 185, 3164–3177. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.; Wildner, H.; Birchmeier, C. Insm1 controls the differentiation of pulmonary neuroendocrine cells by repressing Hes1. Dev. Biol. 2015, 408, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Goto, Y.; De Silva, M.G.; Toscani, A.; Prabhakar, B.S.; Notkins, A.L.; Lan, M.S. A novel human insulinoma-associated cDNA, IA-1, encodes a protein with “zinc-finger” DNA-binding motifs. J. Biol. Chem. 1992, 267, 15252–15257. [Google Scholar] [PubMed]
- Rooper, L.M.; Sharma, R.; Li, Q.K.; Illei, P.B.; Westra, W.H. INSM1 Demonstrates Superior Performance to the Individual and Combined Use of Synaptophysin, Chromogranin and CD56 for Diagnosing Neuroendocrine Tumors of the Thoracic Cavity. Am. J. Surg. Pathol. 2017, 41, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Hsu, P.P.; Awad, M.M.; Engelman, J.A. Tyrosine kinase gene rearrangements in epithelial malignancies. Nat. Rev. Cancer 2013, 13, 772–787. [Google Scholar] [CrossRef] [PubMed]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.; Watanabe, H.; Kurashina, K.; Hatanaka, H.; et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 2007, 448, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Takeuchi, K.; Togashi, Y.; Nomura, K.; Ninomiya, H.; Okui, M.; Satoh, Y.; Okumura, S.; Nakagawa, K.; Soda, M.; et al. EML4-ALK fusion is linked to histological characteristics in a subset of lung cancers. J. Thorac. Oncol. 2008, 3, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Yeap, B.Y.; Mino-Kenudson, M.; Digumarthy, S.R.; Costa, D.B.; Heist, R.S.; Solomon, B.; Stubbs, H.; Admane, S.; McDermott, U.; et al. Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J. Clin. Oncol. 2009, 27, 4247–4253. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Takeuchi, K.; Togashi, Y.; Hatano, S.; Ninomiya, H.; Motoi, N.; Mun, M.Y.; Sakao, Y.; Okumura, S.; Nakagawa, K.; et al. EML4-ALK lung cancers are characterized by rare other mutations, a TTF-1 cell lineage, an acinar histology, and young onset. Mod. Pathol. 2009, 22, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.L.; Bang, Y.J.; Camidge, D.R.; Shaw, A.T.; Solomon, B.; Maki, R.G.; Ou, S.H.; Dezube, B.J.; Janne, P.A.; Costa, D.B.; et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, D.W.; Mehra, R.; Tan, D.S.; Felip, E.; Chow, L.Q.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; et al. Ceritinib in ALK-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 370, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P. ALK in Non-Small Cell Lung Cancer (NSCLC) Pathobiology, Epidemiology, Detection from Tumor Tissue and Algorithm Diagnosis in a Daily Practice. Cancers 2017, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- Conklin, C.M.; Craddock, K.J.; Have, C.; Laskin, J.; Couture, C.; Ionescu, D.N. Immunohistochemistry is a reliable screening tool for identification of ALK rearrangement in non-small-cell lung carcinoma and is antibody dependent. J. Thorac. Oncol. 2013, 8, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Van der Wekken, A.J.; Pelgrim, R.; ’t Hart, N.; Werner, N.; Mastik, M.F.; Hendriks, L.; van der Heijden, E.; Looijen-Salamon, M.; de Langen, A.J.; Staal-van den Brekel, J.; et al. Dichotomous ALK-IHC Is a Better Predictor for ALK Inhibition Outcome than Traditional ALK-FISH in Advanced Non-Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 4251–4258. [Google Scholar] [CrossRef] [PubMed]
- Thorne-Nuzzo, T.; Williams, C.; Catallini, A.; Clements, J.; Singh, S.; Amberson, J.; Dickinson, K.; Gatalica, Z.; Ho, S.N.; Loftin, I.; et al. A sensitive ALK immunohistochemistry companion diagnostic test identifies patients eligible for treatment with Crizotinib. J. Thorac. Oncol. 2017, 12, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Di Lorito, A.; Pace, M.V.; Iezzi, M.; Felicioni, L.; D’Antuono, T.; Filice, G.; Guetti, L.; Mucilli, F.; Buttitta, F. ALK Protein Analysis by IHC Staining after Recent Regulatory Changes: A Comparison of Two Widely Used Approaches, Revision of the Literature, and a New Testing Algorithm. J. Thorac. Oncol. 2016, 11, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Wynes, M.W.; Sholl, L.M.; Dietel, M.; Schuuring, E.; Tsao, M.S.; Yatabe, Y.; Tubbs, R.R.; Hirsch, F.R. An international interpretation study using the ALK IHC antibody D5F3 and a sensitive detection kit demonstrates high concordance between ALK IHC and ALK FISH and between evaluators. J. Thorac. Oncol. 2014, 9, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Bergethon, K.; Shaw, A.T.; Ou, S.H.; Katayama, R.; Lovly, C.M.; McDonald, N.T.; Massion, P.P.; Siwak-Tapp, C.; Gonzalez, A.; Fang, R.; et al. ROS1 rearrangements define a unique molecular class of lung cancers. J. Clin. Oncol. 2012, 30, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.D.; Le, A.T.; Theodoro, M.F.; Skokan, M.C.; Aisner, D.L.; Berge, E.M.; Terracciano, L.M.; Cappuzzo, F.; Incarbone, M.; Roncalli, M.; et al. Identifying and targeting ROS1 gene fusions in non-small cell lung cancer. Clin. Cancer Res. 2012, 18, 4570–4579. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Ou, S.H.; Bang, Y.J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, A.; Tsuta, K.; Wakai, S.; Arai, Y.; Asamura, H.; Shibata, T.; Furuta, K.; Kohno, T.; Kushima, R. Immunohistochemical detection of ROS1 is useful for identifying ROS1 rearrangements in lung cancers. Mod. Pathol. 2014, 27, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.M.; Kim, H.R.; Lee, J.S.; Lee, K.H.; Lee, Y.G.; Min, Y.J.; Cho, E.K.; Lee, S.S.; Kim, B.S.; Choi, M.Y.; et al. Open-label, multicenter, phase II study of ceritinib in patients with non-small-cell lung cancer harboring ROS1 rearrangement. J. Clin. Oncol. 2017, 35, 2613–2618. [Google Scholar] [CrossRef] [PubMed]
- Boyle, T.A.; Masago, K.; Ellison, K.E.; Yatabe, Y.; Hirsch, F.R. ROS1 immunohistochemistry among major genotypes of non-small-cell lung cancer. Clin. Lung Cancer 2015, 16, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Mescam-Mancini, L.; Lantuejoul, S.; Moro-Sibilot, D.; Rouquette, I.; Souquet, P.J.; Audigier-Valette, C.; Sabourin, J.C.; Decroisette, C.; Sakhri, L.; Brambilla, E.; et al. On the relevance of a testing algorithm for the detection of ROS1-rearranged lung adenocarcinomas. Lung Cancer 2014, 83, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Buttner, R.; Al-Dayel, F.; Dietel, M.; Elmberger, G.; Kerr, K.; Lopez-Rios, F.; Marchetti, A.; Oz, B.; Pauwels, P.; et al. Testing for ROS1 in non-small cell lung cancer: A review with recommendations. Virchows Arch. 2016, 469, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Sholl, L.M.; Sun, H.; Butaney, M.; Zhang, C.; Lee, C.; Janne, P.A.; Rodig, S.J. ROS1 immunohistochemistry for detection of ROS1-rearranged lung adenocarcinomas. Am. J. Surg. Pathol. 2013, 37, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.J.; Lee, J.S.; Kim, H.R.; Lim, S.M.; Cho, B.C.; Lee, C.Y.; Shim, H.S. Screening of ROS1 rearrangements in lung adenocarcinoma by immunohistochemistry and comparison with ALK rearrangements. PLoS ONE 2014, 9, e103333. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.M.; Lee, H.; Toyooka, S.; Shimizu, N.; et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Ninomiya, H.; Ishikawa, Y.; Matsubara, O. Is the epidermal growth factor receptor status in lung cancers reflected in clinicopathologic features? Arch. Pathol. Lab. Med. 2010, 134, 66–72. [Google Scholar] [PubMed]
- Leighl, N.B.; Rekhtman, N.; Biermann, W.A.; Huang, J.; Mino-Kenudson, M.; Ramalingam, S.S.; West, H.; Whitlock, S.; Somerfield, M.R. Molecular testing for selection of patients with lung cancer for epidermal growth factor receptor and anaplastic lymphoma kinase tyrosine kinase inhibitors: American Society of Clinical Oncology endorsement of the College of American Pathologists/International Association for the study of lung cancer/association for molecular pathology guideline. J. Clin. Oncol. 2014, 32, 3673–3679. [Google Scholar] [PubMed]
- Lindeman, N.I.; Cagle, P.T.; Beasley, M.B.; Chitale, D.A.; Dacic, S.; Giaccone, G.; Jenkins, R.B.; Kwiatkowski, D.J.; Saldivar, J.S.; Squire, J.; et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: Guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J. Thorac. Oncol. 2013, 8, 823–859. [Google Scholar] [PubMed]
- Yu, J.; Kane, S.; Wu, J.; Benedettini, E.; Li, D.; Reeves, C.; Innocenti, G.; Wetzel, R.; Crosby, K.; Becker, A.; et al. Mutation-specific antibodies for the detection of EGFR mutations in non-small-cell lung cancer. Clin. Cancer Res. 2009, 15, 3023–3028. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Labarriere, N. PD-1 expression on tumor-specific T cells: Friend or foe for immunotherapy? Oncoimmunology 2017, 7, e1364828. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Boyle, T.A.; Zhou, C.; Rimm, D.L.; Hirsch, F.R. PD-L1 Expression in Lung Cancer. J. Thorac. Oncol. 2016, 11, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.H.; Kummel, A.; Gorlich, D.; Mohr, M.; Brockling, S.; Mikesch, J.H.; Grunewald, I.; Marra, A.; Schultheis, A.M.; Wardelmann, E.; et al. PD-1 and PD-L1 Expression in NSCLC Indicate a Favorable Prognosis in Defined Subgroups. PLoS ONE 2015, 10, e0136023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.Y.; Lin, M.W.; Chang, Y.L.; Wu, C.T.; Yang, P.C. Programmed cell death-ligand 1 expression in surgically resected stage I pulmonary adenocarcinoma and its correlation with driver mutations and clinical outcomes. Eur. J. Cancer 2014, 50, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Cooper, W.A.; Tran, T.; Vilain, R.E.; Madore, J.; Selinger, C.I.; Kohonen-Corish, M.; Yip, P.; Yu, B.; O’Toole, S.A.; McCaughan, B.C.; et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer 2015, 89, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Fang, W.; Zhang, Y.; Hong, S.; Kang, S.; Yan, Y.; Chen, N.; Zhan, J.; He, X.; Qin, T.; et al. The association between PD-L1 and EGFR status and the prognostic value of PD-L1 in advanced non-small cell lung cancer patients treated with EGFR-TKIs. Oncotarget 2015, 6, 14209–14219. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Lin, M.W.; Chang, Y.L.; Wu, C.T.; Yang, P.C. Programmed cell death-ligand 1 expression is associated with a favourable immune microenvironment and better overall survival in stage I pulmonary squamous cell carcinoma. Eur. J. Cancer 2016, 57, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Azuma, K.; Kawahara, A.; Yamada, K.; Imamura, Y.; Tokito, T.; Kinoshita, T.; Kage, M.; Hoshino, T. Significance of programmed cell death-ligand 1 expression and its association with survival in patients with small cell lung cancer. J. Thorac. Oncol. 2015, 10, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Yokouchi, Y.; Kobayashi, M.; Ninomiya, H.; Sakakibara, R.; Nishio, M.; Okumura, S.; Ishikawa, Y. Relationship of tumor PD-L1 (CD274) expression with lower mortality in lung high-grade neuroendocrine tumor. Cancer Med. 2017, 6, 2347–2356. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.L.; Yang, C.Y.; Huang, Y.L.; Wu, C.T.; Yang, P.C. High PD-L1 expression is associated with stage IV disease and poorer overall survival in 186 cases of small cell lung cancers. Oncotarget 2017, 8, 18021–18030. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crino, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non-Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef] [PubMed]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P. PD-L1 immunohistochemistry for non-small cell lung carcinoma: Which strategy should be adopted? Expert Rev. Mol. Diagn. 2017, 17, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; Kudchadkar, R.R.; Yu, B.; Gallenstein, D.; Horak, C.E.; Inzunza, H.D.; Zhao, X.; Martinez, A.J.; Wang, W.; Gibney, G.; et al. Safety, efficacy, and biomarkers of nivolumab with vaccine in ipilimumab-refractory or -naive melanoma. J. Clin. Oncol. 2013, 31, 4311–4318. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Yokoi, T.; McCleod, M.J.; Fischer, J.R.; Kim, Y.C.; Ballas, M.; Shi, K.; Soria, J.C. A Phase III Study of Durvalumab (MEDI4736) With or Without Tremelimumab for Previously Treated Patients with Advanced NSCLC: Rationale and Protocol Design of the ARCTIC Study. Clin. Lung Cancer 2016, 17, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.L.; Russell, J.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbe, C.; Linette, G.P.; Milella, M.; et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: A multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1374–1385. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Gulley, J.L.; Rajan, A.; Spigel, D.R.; Iannotti, N.; Chandler, J.; Wong, D.J.L.; Leach, J.; Edenfield, W.J.; Wang, D.; Grote, H.J.; et al. Avelumab for patients with previously treated metastatic or recurrent non-small-cell lung cancer (JAVELIN Solid Tumor): Dose-expansion cohort of a multicentre, open-label, phase 1b trial. Lancet Oncol. 2017, 18, 599–610. [Google Scholar] [CrossRef]
- Ilie, M.; Khambata-Ford, S.; Copie-Bergman, C.; Huang, L.; Juco, J.; Hofman, V.; Hofman, P. Use of the 22C3 anti-PD-L1 antibody to determine PD-L1 expression in multiple automated immunohistochemistry platforms. PLoS ONE 2017, 12, e0183023. [Google Scholar]
- Hirsch, F.R.; McElhinny, A.; Stanforth, D.; Ranger-Moore, J.; Jansson, M.; Kulangara, K.; Richardson, W.; Towne, P.; Hanks, D.; Vennapusa, B.; et al. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J. Thorac. Oncol. 2017, 12, 208–222. [Google Scholar] [CrossRef] [PubMed]
- Rimm, D.L.; Han, G.; Taube, J.M.; Yi, E.S.; Bridge, J.A.; Flieder, D.B.; Homer, R.; West, W.W.; Wu, H.; Roden, A.C.; et al. A Prospective, Multi-institutional, Pathologist-Based Assessment of 4 Immunohistochemistry Assays for PD-L1 Expression in Non-Small Cell Lung Cancer. JAMA Oncol. 2017, 3, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Brunnstrom, H.; Johansson, A.; Westbom-Fremer, S.; Backman, M.; Djureinovic, D.; Patthey, A.; Isaksson-Mettavainio, M.; Gulyas, M.; Micke, P. PD-L1 immunohistochemistry in clinical diagnostics of lung cancer: Inter-pathologist variability is higher than assay variability. Mod. Pathol. 2017, 30, 1411–1421. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Barberis, M.; Franco, R.; De Luca, G.; Pace, M.V.; Staibano, S.; Volante, M.; Buttitta, F.; Guerini-Rocco, E.; Righi, L.; et al. Multicenter Comparison of 22C3 PharmDx (Agilent) and SP263 (Ventana) Assays to Test PD-L1 Expression for NSCLC Patients to Be Treated with Immune Checkpoint Inhibitors. J. Thorac. Oncol. 2017, 12, 1654–1663. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, M.J.; Sharpe, A.; Midha, A.; Barker, C.; Scott, M.; Scorer, P.; Al-Masri, H.; Rebelatto, M.C.; Walker, J. Agreement between Programmed Cell Death Ligand-1 Diagnostic Assays across Multiple Protein Expression Cutoffs in Non-Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 3585–3591. [Google Scholar] [CrossRef] [PubMed]
- Cigognetti, M.; Lonardi, S.; Fisogni, S.; Balzarini, P.; Pellegrini, V.; Tironi, A.; Bercich, L.; Bugatti, M.; Rossi, G.; Murer, B.; et al. BAP1 (BRCA1-associated protein 1) is a highly specific marker for differentiating mesothelioma from reactive mesothelial proliferations. Mod. Pathol. 2015, 28, 1043–1057. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.C.; Pyott, S.; Rodriguez, S.; Cindric, A.; Carr, A.; Michelsen, C.; Thompson, K.; Tse, C.H.; Gown, A.M.; Churg, A. BAP1 Immunohistochemistry and p16 FISH in the Diagnosis of Sarcomatous and Desmoplastic Mesotheliomas. Am. J. Surg. Pathol. 2016, 40, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Hiroshima, K.; Yusa, T.; Ozaki, D.; Koh, E.; Sekine, Y.; Matsumoto, S.; Nabeshima, K.; Sato, A.; Tsujimura, T.; et al. Usefulness of p16/CDKN2A fluorescence in situ hybridization and BAP1 immunohistochemistry for the diagnosis of biphasic mesothelioma. Ann. Diagn. Pathol. 2017, 26, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Hiroshima, K.; Matsumoto, S.; Nabeshima, K.; Yusa, T.; Ozaki, D.; Fujino, M.; Yamakawa, H.; Nakatani, Y.; Tada, Y.; et al. Diagnostic usefulness of p16/CDKN2A FISH in distinguishing between sarcomatoid mesothelioma and fibrous pleuritis. Am. J. Clin. Pathol. 2013, 139, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Husain, A.N.; Colby, T.V.; Ordonez, N.G.; Allen, T.C.; Attanoos, R.L.; Beasley, M.B.; Butnor, K.J.; Chirieac, L.R.; Churg, A.M.; Dacic, S.; et al. Guidelines for Pathologic Diagnosis of Malignant Mesothelioma 2017 Update of the Consensus Statement From the International Mesothelioma Interest Group. Arch. Pathol. Lab. Med. 2018, 142, 89–108. [Google Scholar] [CrossRef] [PubMed]
- Kuraoka, M.; Amatya, V.J.; Kushitani, K.; Mawas, A.S.; Miyata, Y.; Okada, M.; Kishimoto, T.; Inai, K.; Nishisaka, T.; Sueda, T.; et al. Identification of DAB2 and Intelectin-1 as Novel Positive Immunohistochemical Markers of Epithelioid Mesothelioma by Transcriptome Microarray Analysis for Its Differentiation From Pulmonary Adenocarcinoma. Am. J. Surg. Pathol. 2017, 41, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Amatya, V.J.; Kushitani, K.; Mawas, A.S.; Miyata, Y.; Okada, M.; Kishimoto, T.; Inai, K.; Takeshima, Y. MUC4, a novel immunohistochemical marker identified by gene expression profiling, differentiates pleural sarcomatoid mesothelioma from lung sarcomatoid carcinoma. Mod. Pathol. 2017, 30, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Sholl, L.M.; Nishino, M.; Pokharel, S.; Mino-Kenudson, M.; French, C.A.; Janne, P.A.; Lathan, C. Primary Pulmonary NUT Midline Carcinoma: Clinical, Radiographic, and Pathologic Characterizations. J. Thorac. Oncol. 2015, 10, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Bauer, D.E.; Mitchell, C.M.; Strait, K.M.; Lathan, C.S.; Stelow, E.B.; Luer, S.C.; Muhammed, S.; Evans, A.G.; Sholl, L.M.; Rosai, J.; et al. Clinicopathologic features and long-term outcomes of NUT midline carcinoma. Clin. Cancer Res. 2012, 18, 5773–5779. [Google Scholar] [CrossRef] [PubMed]
- French, C.A.; Kutok, J.L.; Faquin, W.C.; Toretsky, J.A.; Antonescu, C.R.; Griffin, C.A.; Nose, V.; Vargas, S.O.; Moschovi, M.; Tzortzatou-Stathopoulou, F.; et al. Midline carcinoma of children and young adults with NUT rearrangement. J. Clin. Oncol. 2004, 22, 4135–4139. [Google Scholar] [CrossRef] [PubMed]
- French, C.A.; Miyoshi, I.; Kubonishi, I.; Grier, H.E.; Perez-Atayde, A.R.; Fletcher, J.A. BRD4-NUT fusion oncogene: A novel mechanism in aggressive carcinoma. Cancer Res. 2003, 63, 304–307. [Google Scholar] [PubMed]
- French, C.A.; Ramirez, C.L.; Kolmakova, J.; Hickman, T.T.; Cameron, M.J.; Thyne, M.E.; Kutok, J.L.; Toretsky, J.A.; Tadavarthy, A.K.; Kees, U.R.; et al. BRD-NUT oncoproteins: A family of closely related nuclear proteins that block epithelial differentiation and maintain the growth of carcinoma cells. Oncogene 2008, 27, 2237–2242. [Google Scholar] [CrossRef] [PubMed]
- French, C.A.; Rahman, S.; Walsh, E.M.; Kuhnle, S.; Grayson, A.R.; Lemieux, M.E.; Grunfeld, N.; Rubin, B.P.; Antonescu, C.R.; Zhang, S.; et al. NSD3-NUT fusion oncoprotein in NUT midline carcinoma: Implications for a novel oncogenic mechanism. Cancer Discov. 2014, 4, 928–941. [Google Scholar] [CrossRef] [PubMed]
- French, C.A. Pathogenesis of NUT midline carcinoma. Annu. Rev. Pathol. 2012, 7, 247–265. [Google Scholar] [CrossRef] [PubMed]
- French, C.A. The importance of diagnosing NUT midline carcinoma. Head Neck Pathol. 2013, 7, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Stathis, A.; Zucca, E.; Bekradda, M.; Gomez-Roca, C.; Delord, J.P.; de La Motte Rouge, T.; Uro-Coste, E.; de Braud, F.; Pelosi, G.; French, C.A. Clinical Response of Carcinomas Harboring the BRD4-NUT Oncoprotein to the Targeted Bromodomain Inhibitor OTX015/MK-8628. Cancer Discov. 2016, 6, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Stathis, A.; Bertoni, F. BET Proteins as Targets for Anticancer Treatment. Cancer Discov. 2018, 8, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Haack, H.; Johnson, L.A.; Fry, C.J.; Crosby, K.; Polakiewicz, R.D.; Stelow, E.B.; Hong, S.M.; Schwartz, B.E.; Cameron, M.J.; Rubin, M.A.; et al. Diagnosis of NUT midline carcinoma using a NUT-specific monoclonal antibody. Am. J. Surg. Pathol. 2009, 33, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Laskin, W.; Chen, Y.; French, C.A.; Cameron, M.J.; Nayar, R.; Lin, X. NUT midline carcinoma: A neoplasm with diagnostic challenges in cytology. Cytopathology 2011, 22, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.G.; French, C.A.; Cameron, M.J.; Fletcher, C.D.; Jackman, D.M.; Lathan, C.S.; Sholl, L.M. Pathologic characteristics of NUT midline carcinoma arising in the mediastinum. Am. J. Surg. Pathol. 2012, 36, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Roh, J.; Park, C.S. Immunohistochemistry for Pathologists: Protocols, Pitfalls, and Tips. J. Pathol. Transl. Med. 2016, 50, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Bass, B.P.; Engel, K.B.; Greytak, S.R.; Moore, H.M. A review of preanalytical factors affecting molecular, protein, and morphological analysis of formalin-fixed, paraffin-embedded (FFPE) tissue: How well do you know your FFPE specimen? Arch. Pathol. Lab. Med. 2014, 138, 1520–1530. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic of the complex pathways of neuroendocrine differentiation (blue) in lung tumors. INSM1 (red) is inactivated by HES1 and promotes the expression of the three neuroendocrine molecules (CHGA, SYP, and NCAM1) via activation of the transcription factors, ASCL1, and BRN2. INSM1 and ASCL1 activate each other.
Figure 1.
Schematic of the complex pathways of neuroendocrine differentiation (blue) in lung tumors. INSM1 (red) is inactivated by HES1 and promotes the expression of the three neuroendocrine molecules (CHGA, SYP, and NCAM1) via activation of the transcription factors, ASCL1, and BRN2. INSM1 and ASCL1 activate each other.

Figure 2.
(A) Morphology of small cell lung carcinoma (hematoxylin and eosin staining); (B) INSM1 immunostaining (nuclear; positive). Scale bar = 100 µm.
Figure 2.
(A) Morphology of small cell lung carcinoma (hematoxylin and eosin staining); (B) INSM1 immunostaining (nuclear; positive). Scale bar = 100 µm.
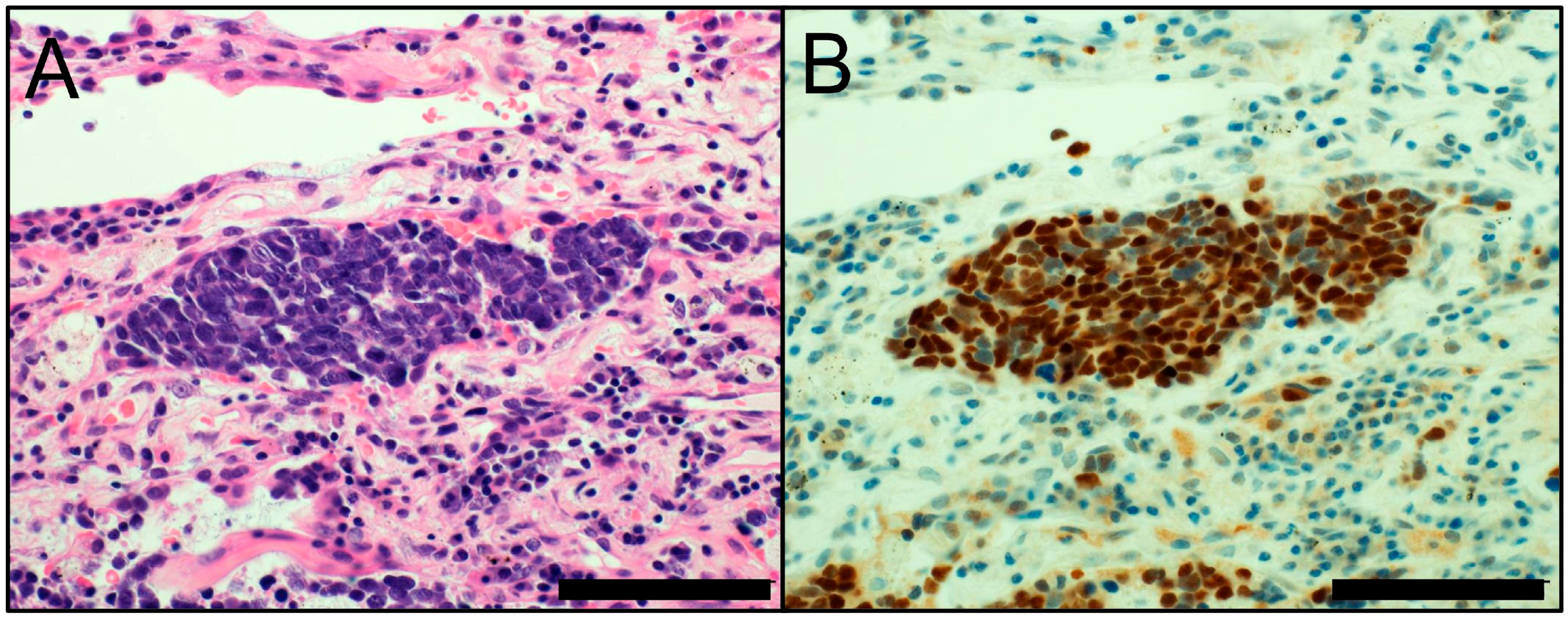
Figure 3.
(A) ALK-rearranged lung adenocarcinoma with a signet-ring cell pattern (hematoxylin and eosin staining); (B) ALK immunostaining (cytoplasmic; positive). Scale bar = 100 µm.
Figure 3.
(A) ALK-rearranged lung adenocarcinoma with a signet-ring cell pattern (hematoxylin and eosin staining); (B) ALK immunostaining (cytoplasmic; positive). Scale bar = 100 µm.
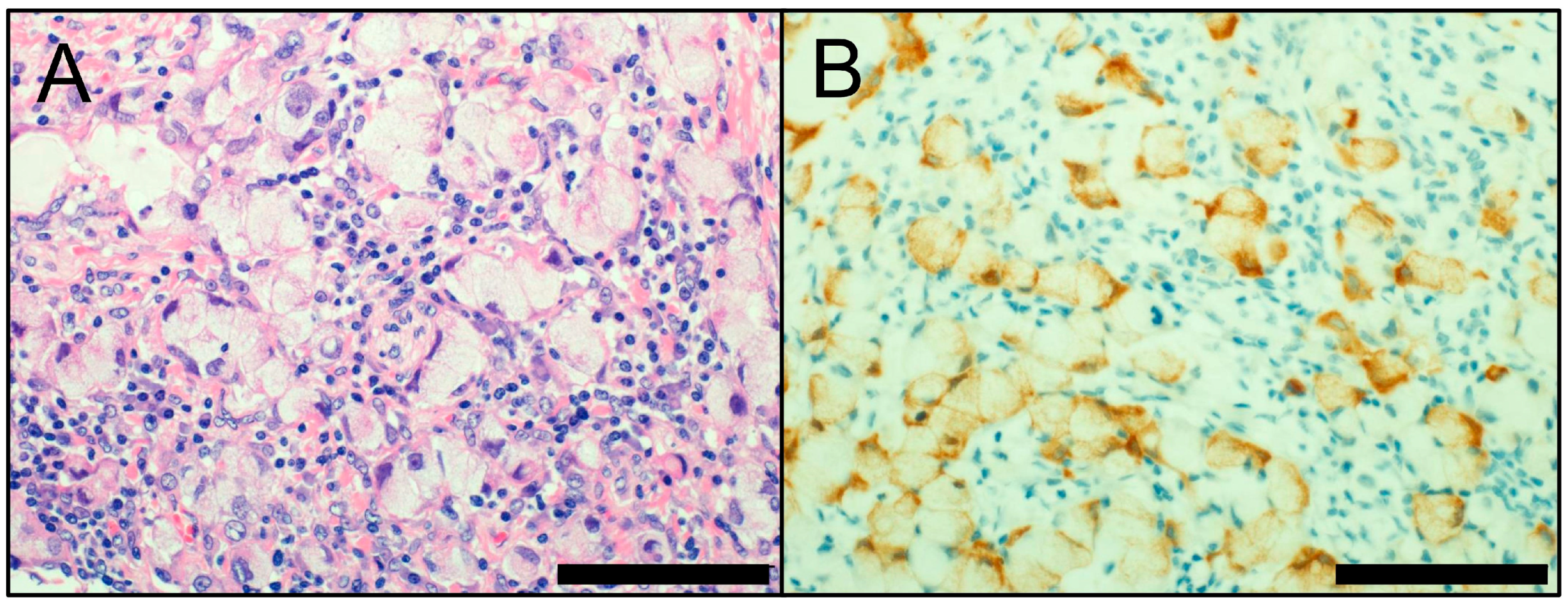
Figure 4.
(A) Morphology of NUT carcinoma (hematoxylin and eosin staining). Immunohistochemistry of NUT carcinoma; (B) NUT staining (nuclear; positive); (C) p40 staining (nuclear; focally positive); and (D) SYP staining (cytoplasmic; very focally positive). Scale bar = 100 µm.
Figure 4.
(A) Morphology of NUT carcinoma (hematoxylin and eosin staining). Immunohistochemistry of NUT carcinoma; (B) NUT staining (nuclear; positive); (C) p40 staining (nuclear; focally positive); and (D) SYP staining (cytoplasmic; very focally positive). Scale bar = 100 µm.
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Inamura, K. Update on Immunohistochemistry for the Diagnosis of Lung Cancer. Cancers 2018, 10, 72. https://doi.org/10.3390/cancers10030072
AMA Style
Inamura K. Update on Immunohistochemistry for the Diagnosis of Lung Cancer. Cancers. 2018; 10(3):72. https://doi.org/10.3390/cancers10030072
Chicago/Turabian StyleInamura, Kentaro. 2018. "Update on Immunohistochemistry for the Diagnosis of Lung Cancer" Cancers 10, no. 3: 72. https://doi.org/10.3390/cancers10030072
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.