A Multicenter Study to Assess EGFR Mutational Status in Plasma: Focus on an Optimized Workflow for Liquid Biopsy in a Clinical Setting

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Patient Cohort
2.2. Sample Characteristics
2.3. Pre-Analytical Variables
2.3.1. Effect of Pre-Analytical Variables on Plasma Volume and Hemolysis
2.3.2. Effect of Pre-Analytical Variables on Reached Assay Sensitivity
3. cfDNA Analysis
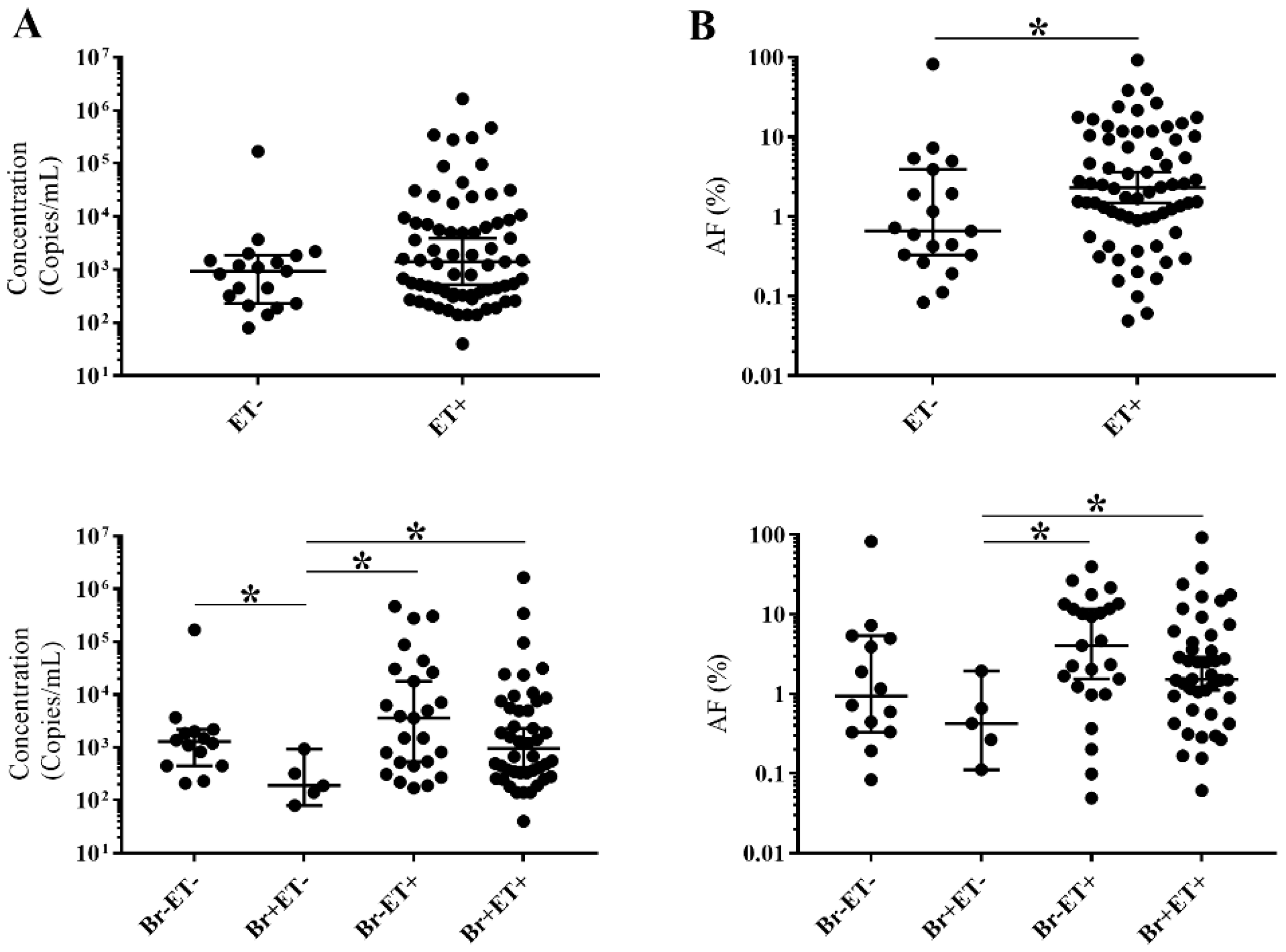
3.1. CtDNA Detection
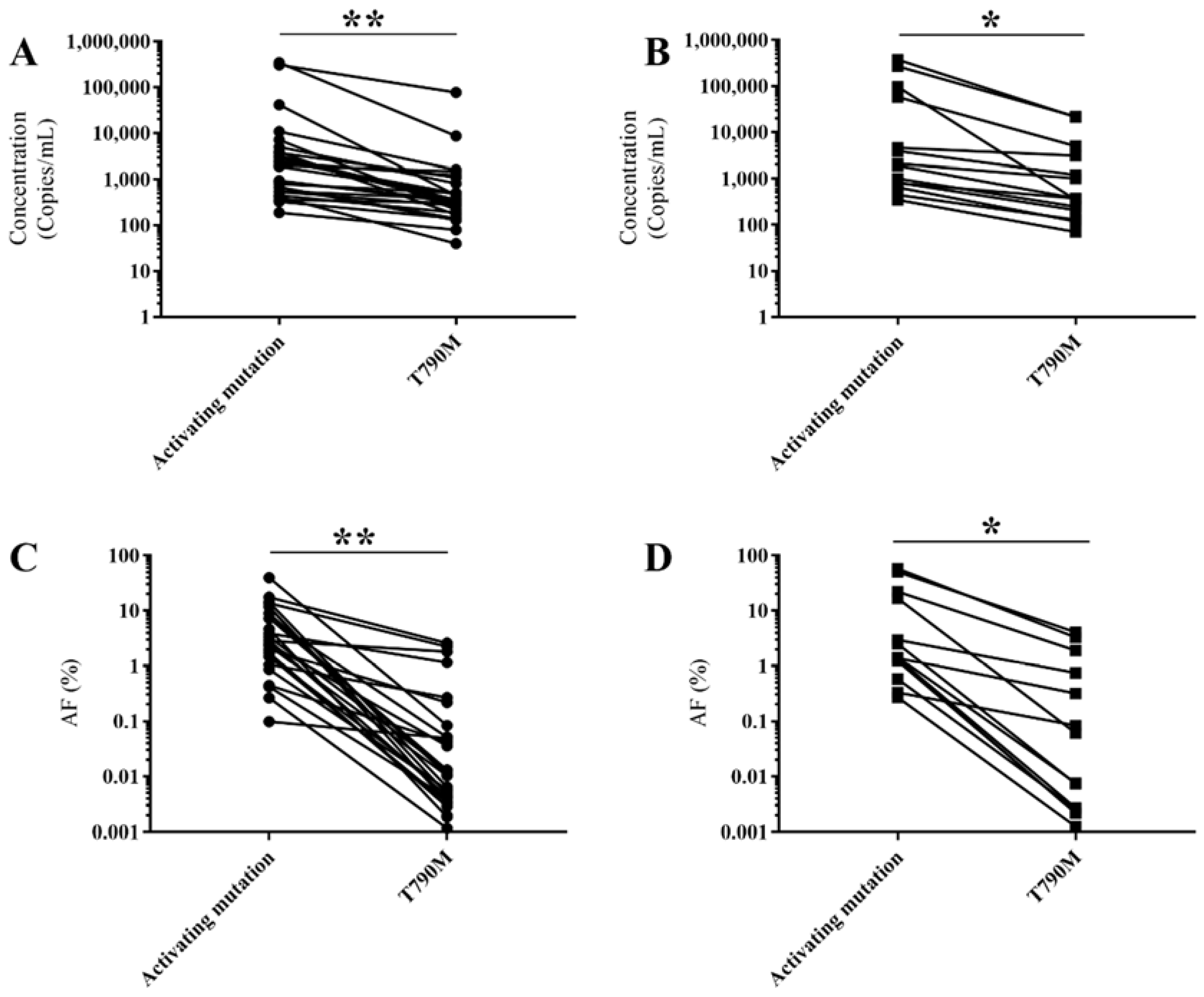
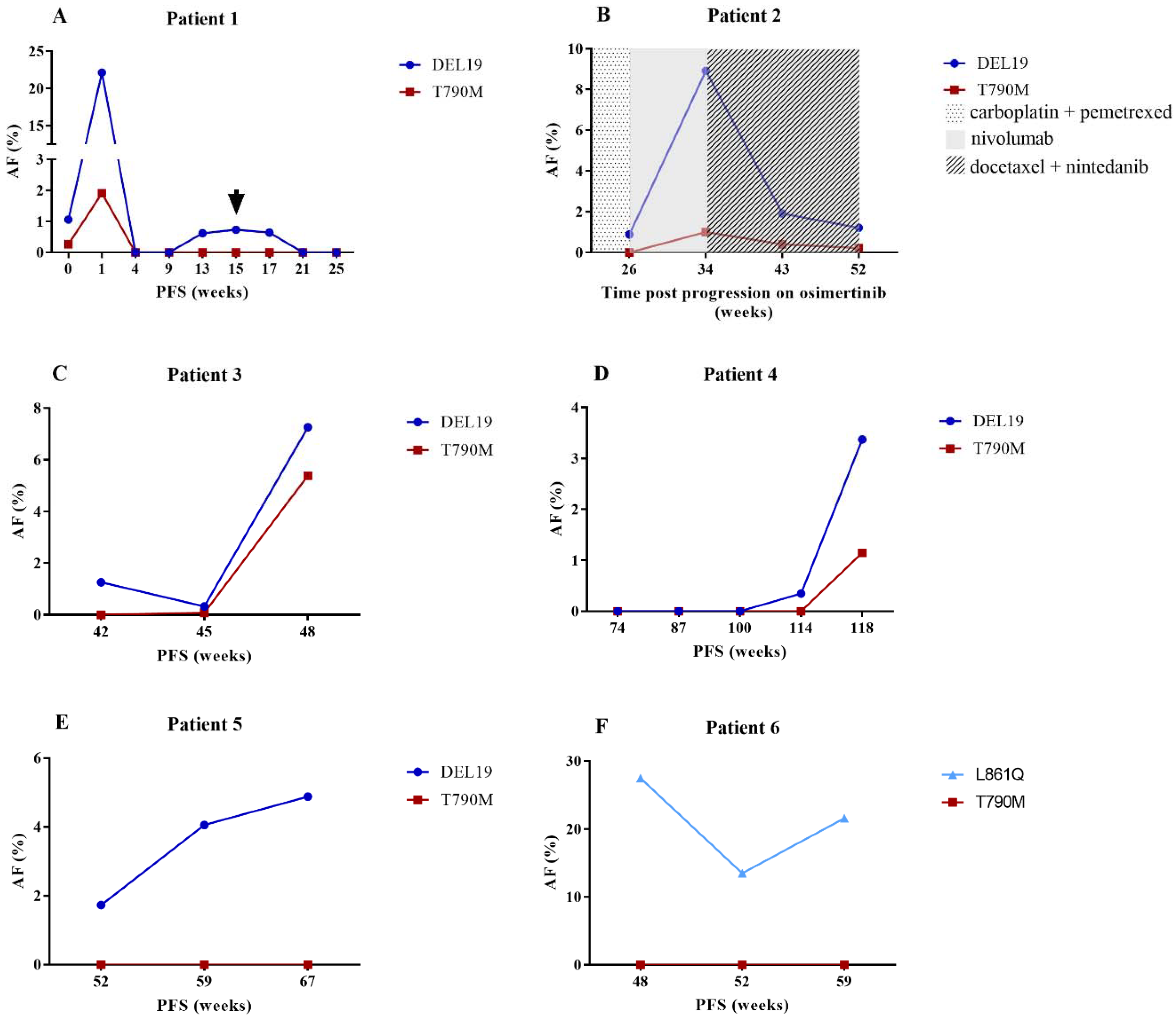
3.2. ctDNA Characteristics
4. Discussion
5. Material and Methods
5.1. Study Design
5.2. Sample Collection and Processing
5.3. CfDNA Isolation and Analysis
5.4. Statistical Analysis
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S., Jr.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic therapy for stage iv non-small-cell lung cancer: American society of clinical oncology clinical practice guideline update. J. Clin. Oncol. 2017, 35, 3484–3515. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated egfr. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.K.; et al. Genotypic and histological evolution of lung cancers acquiring resistance to egfr inhibitors. Sci. Transl. Med. 2011, 3, 75ra26. [Google Scholar] [CrossRef] [PubMed]
- Sorber, L.; Zwaenepoel, K.; Deschoolmeester, V.; Van Schil, P.E.; Van Meerbeeck, J.; Lardon, F.; Rolfo, C.; Pauwels, P. Circulating cell-free nucleic acids and platelets as a liquid biopsy in the provision of personalized therapy for lung cancer patients. Lung Cancer 2017, 107, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.M.; Kothari, P.D.; Mouliere, F.; Mair, R.; Somnay, S.; Benayed, R.; Zehir, A.; Weigelt, B.; Dawson, S.J.; Arcila, M.E.; et al. The value of cell-free DNA for molecular pathology. J. Pathol. 2018, 244, 616–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Reckamp, K.L.; Melnikova, V.O.; Karlovich, C.; Sequist, L.V.; Camidge, D.R.; Wakelee, H.; Perol, M.; Oxnard, G.R.; Kosco, K.; Croucher, P.; et al. A highly sensitive and quantitative test platform for detection of nsclc egfr mutations in urine and plasma. J. Thorac. Oncol. 2016, 11, 1690–1700. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.W.; Karlovich, C.; Sequist, L.V.; Melnikova, V.; Franovic, A.; Gadgeel, S.M.; Reckamp, K.L.; Camidge, D.R.; Pérol, M.; Ou, S.-H.I.; et al. Egfr genotyping of matched urine, plasma, and tumor tissue in patients with non-small-cell lung cancer treated with rociletinib, an egfr tyrosine kinase inhibitor. Precis. Oncol. 2018, 2, 1–13. [Google Scholar] [CrossRef]
- Cobas EGFR Mutation Test v2. Available online: http://www.Fda.Gov/drugs/informationondrugs/approveddrugs/ucm504540.Htm (accessed on 2 June 2016).
- Oxnard, G.R.; Thress, K.S.; Alden, R.S.; Lawrance, R.; Paweletz, C.P.; Cantarini, M.; Yang, J.C.; Barrett, J.C.; Janne, P.A. Association between plasma genotyping and outcomes of treatment with osimertinib (azd9291) in advanced non-small-cell lung cancer. J. Clin. Oncol. 2016, 34, 3375–3382. [Google Scholar] [CrossRef] [PubMed]
- Sacher, A.G.; Paweletz, C.; Dahlberg, S.E.; Alden, R.S.; O’Connell, A.; Feeney, N.; Mach, S.L.; Janne, P.A.; Oxnard, G.R. Prospective validation of rapid plasma genotyping for the detection of egfr and kras mutations in advanced lung cancer. JAMA Oncol. 2016, 2, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, N.; Spencer, E.; Torkamani, A.; Nicholson, L. Liquid biopsies for cancer: Coming to a patient near you. J. Clin. Med. 2017, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Qing, X.; Xiumin, W.; Yali, B.; Chi, S.; Bak, S.H.; Lee, H.Y.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; et al. Longitudinal monitoring of egfr mutations in plasma predicts outcomes of nsclc patients treated with egfr tkis: Korean lung cancer consortium (klcc-12-02). Oncotarget 2016, 7, 6984–6993. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.; Diaz, I.M. Controlling Pre-Analytical Variables in Liquid Biopsy Assay Development. Available online: http://www.healthtech.com/streck/controlling-pre-analytical-variables/ (accessed on 26 January 2017).
- Streck. Cell-free DNA bct: Instructions for use. Available online: https://www.streck.com/collection/cell-free-dna-bct/ (accessed on 23 August 2018).
- Sherwood, J.L.; Corcoran, C.; Brown, H.; Sharpe, A.D.; Musilova, M.; Kohlmann, A. Optimised pre-analytical methods improve kras mutation detection in circulating tumour DNA (ctdna) from patients with non-small cell lung cancer (nsclc). PLoS ONE 2016, 11, e0150197. [Google Scholar] [CrossRef] [PubMed]
- Diaz, I.M.; Nocon, A.; Mehnert, D.H.; Fredebohm, J.; Diehl, F.; Holtrup, F. Performance of streck cfdna blood collection tubes for liquid biopsy testing. PloS ONE 2016, 11, e0166354. [Google Scholar]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra224. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Paweletz, C.P.; Kuang, Y.; Mach, S.L.; O’Connell, A.; Messineo, M.M.; Luke, J.J.; Butaney, M.; Kirschmeier, P.; Jackman, D.M.; et al. Noninvasive detection of response and resistance in egfr-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin. Cancer Res. 2014, 20, 1698–1705. [Google Scholar] [CrossRef] [PubMed]
- Ariyasu, R.; Nishikawa, S.; Uchibori, K.; Oh-Hara, T.; Yoshizawa, T.; Dotsu, Y.; Koyama, J.; Saiki, M.; Sonoda, T.; Kitazono, S.; et al. High ratio of t790m to egfr activating mutations correlate with the osimertinib response in non-small-cell lung cancer. Lung Cancer 2018, 117, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Ye, X.; Zhang, M.Z.; Sun, Y.; Wang, J.Y.; Ni, J.; Zhang, H.P.; Zhang, L.; Luo, J.; Zhang, J.; et al. Plasma egfr t790m ctdna status is associated with clinical outcome in advanced nsclc patients with acquired egfr-tki resistance. Sci. Rep. 2016, 6, 20913. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.J.; Mok, T.S.; Chen, Z.H.; Guo, A.L.; Zhang, X.C.; Su, J.; Wu, Y.L. Clinicopathologic and molecular features of epidermal growth factor receptor t790m mutation and c-met amplification in tyrosine kinase inhibitor-resistant chinese non-small cell lung cancer. Pathol. Oncol. Res. 2009, 15, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Nosaki, K.; Otsubo, K.; Azuma, K.; Sakata, S.; Ouchi, H.; Morinaga, R.; Wataya, H.; Fujii, A.; Nakagaki, N.; et al. Acquisition of the t790m resistance mutation during afatinib treatment in egfr tyrosine kinase inhibitor-naive patients with non-small cell lung cancer harboring egfr mutations. Oncotarget 2017, 8, 68123–68130. [Google Scholar] [CrossRef] [PubMed]
- Garrigou, S.; Perkins, G.; Garlan, F.; Normand, C.; Didelot, A.; Le Corre, D.; Peyvandi, S.; Mulot, C.; Niarra, R.; Aucouturier, P.; et al. A study of hypermethylated circulating tumor DNA as a universal colorectal cancer biomarker. Clin. Chem. 2016, 62, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.J.; Zhang, H.B.; Liu, Y.H.; Zhang, F.L.; Zhu, Y.Z.; Li, Y.; Bai, J.P.; Liu, L.R.; Qu, Y.C.; Qu, X.; et al. Estimation of cell-free circulating egfr mutation concentration predicts outcomes in nsclc patients treated with egfr-tkis. Oncotarget 2017, 8, 13195–13205. [Google Scholar] [CrossRef] [PubMed]
- Karachaliou, N.; Mayo-de las Casas, C.; Queralt, C.; de Aguirre, I.; Melloni, B.; Cardenal, F.; Garcia-Gomez, R.; Massuti, B.; Sanchez, J.M.; Porta, R.; et al. Association of egfr l858r mutation in circulating free DNA with survival in the eurtac trial. JAMA Oncol. 2015, 1, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Douillard, J.Y.; Ostoros, G.; Cobo, M.; Ciuleanu, T.; Cole, R.; McWalter, G.; Walker, J.; Dearden, S.; Webster, A.; Milenkova, T.; et al. Gefitinib treatment in egfr mutated caucasian nsclc: Circulating-free tumor DNA as a surrogate for determination of egfr status. J. Thorac. Oncol. 2014, 9, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Sorber, L.; Zwaenepoel, K.; Winne, K.D.; Jacobs, J.; Peeters, M.; Meerbeeck, J.V.; Rolfo, C.; Pauwels, P. Two-step, high-seed centrifugation yields higher plasma amount and less genomic DNA contamination. University of Antwerp: Wilrijk, Belgium, Unpublished work. 2018. [Google Scholar]
- Goethals, S.; De Wilde, A.; Lesage, K.; Smits, E.; Pauwels, P.; Peeters, M. Tumorbank@uza: A collection of tissue, fluid samples and associated data of oncology patients for the use in translational research. Open J. Bioresources 2018, 5, 4. [Google Scholar] [CrossRef]
- Sorber, L.; Zwaenepoel, K.; Deschoolmeester, V.; Roeyen, G.; Lardon, F.; Rolfo, C.; Pauwels, P. A comparison of cell-free DNA isolation kits: Isolation and quantification of cell-free DNA in plasma. J. Mol. Diagn. 2017, 19, 162–168. [Google Scholar] [CrossRef] [PubMed]


 : brain MRI.
: brain MRI.
: brain MRI.
: brain MRI.

{kind=link}
{kind=link}
{kind=link}
| Parameters | N (%) |
|---|---|
| EGFR WT (n = 124) | |
| Median age (years) | 67 |
| Stage at inclusion | |
| I | 13 (10.48) |
| II | 5 (4.03) |
| III | 26 (20.97) |
| IV | 75 (60.78) |
| Unspecified | 5 (4.03) |
| EGFR mutated (n = 110) | |
| Median age (years) | 67.5 |
| Stage at inclusion | |
| I | 4 (3.64) |
| II | 4 (3.64) |
| III | 10 (9.09) |
| IV | 89 (80.91) |
| Unspecified | 3 (2.73) |
| EGFR modification as defined by tissue and/or plasma analysis | |
| DEL19 | 63 (57.27) |
| T790M mutated | 26 (41.26) |
| L858R | 32 (29.09) |
| T790M mutated | 6 (18.75) |
| L861Q | 3 (2.73) |
| T790M mutated | 1 (33.33) |
| G719X | 4 (3.64) |
| T790M mutated | 1 (25) |
| Other | 8 (7.27) |
| Therapy (n = 101 *) | |
| erlotinib | 42 |
| PFS (months) | 12.3 |
| gefitinib | 20 |
| PFS (months) | 12.7 |
| afatinib | 21 |
| PFS (months) | 11.4 |
| osimertinib | 16 |
| PFS (months) | 8.5 |
| Metastases (at inclusion) | |
| Brain | |
| yes | 26 (23.64) |
| no | 75 (68.18) |
| na | 9 (8.18) |
| Extrathoracic | |
| yes | 40 (36.36) |
| no | 61 (55.46) |
| na | 9 (8.18) |
| Sampling Time | EGFR Mutational Stage | ctDNA Sensitivity Adequate | Plasma Volume mL | Transit Time Days | Average Temperature °C | Centrifugation Protocol Two-Step | Hemolysis Status Present |
|---|---|---|---|---|---|---|---|
| PtT (50) | WT (16) | 9 (56.3%) | 3.00 | 1.77 | 13.0 | 5 (38.5%) | 3 (18.8%) |
| Mutated (34) | 21 (61.8%) | 3.00 | 1.59 | 11.0 | 10 (34.5%) | 7 (20.6%) | |
| PD (69) | WT (21) | 12 (60%) | 2.85 | 1.67 | 11.6 | 8 (40%) | 6 (28.6%) |
| Mutated (48) | 29 (61.7%) | 3.00 | 1.34 | 12.5 | 14 (35.9%) | 5 (10.4%) |
| Variables | Protocol | Specifications |
|---|---|---|
| Pre-analytical variables | Streck tubes | |
| Centrifugation protocol | Two-step, high speed: ↑ plasma volume & ↓ gDNA contamination | |
| Transit time | Short: to ensure proper cell and cfDNA stabilization in Streck tubes | |
| Temperature | >10 °C: to ensure proper cell and cfDNA stabilization in Streck tubes | |
| EDTA tubes | ||
| Processing | Within 2 hours: no liquid biopsy-specific preservatives present | |
| Centrifugation protocol | Two step: ↓ gDNA contamination | |
| Analytical & biological variables | ddPCR | |
| Reached assay sensitivitiy | Indication of cfDNA concentration | |
| T790M mutation | Test the majority of the isolated cfDNA: lower concentration & AF than activating mutation↑ ctDNA detection | |
| Metastases | ||
| Extrathoracic | ||
| Intrathoracic | Very high sensitivity is necessary due to low ctDNA concentrations | |
| Brain | Disruption of BBB ↑ ctDNA detection | |
| Interpretation | ctDNA detection | |
| No EGFR mutation | Tissue biopsy | |
| EGFR activating mutation | ||
| Prior to therapy | EGFR TKI therapy is recommended | |
| Without T790M mutation at progressive disease to EGFR TKI therapy | ||
| Low AF | New blood sample in a few weeks time | |
| High AF | Tissue biopsy | |
| EGFR (activating &) T790M mutation | Osimertinib therapy is recommended |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorber, L.; Zwaenepoel, K.; De Winne, K.; Van Casteren, K.; Augustus, E.; Jacobs, J.; Zhang, X.H.; Galdermans, D.; De Droogh, E.; Lefebure, A.; et al. A Multicenter Study to Assess EGFR Mutational Status in Plasma: Focus on an Optimized Workflow for Liquid Biopsy in a Clinical Setting. Cancers 2018, 10, 290. https://doi.org/10.3390/cancers10090290
Sorber L, Zwaenepoel K, De Winne K, Van Casteren K, Augustus E, Jacobs J, Zhang XH, Galdermans D, De Droogh E, Lefebure A, et al. A Multicenter Study to Assess EGFR Mutational Status in Plasma: Focus on an Optimized Workflow for Liquid Biopsy in a Clinical Setting. Cancers. 2018; 10(9):290. https://doi.org/10.3390/cancers10090290
Chicago/Turabian StyleSorber, Laure, Karen Zwaenepoel, Koen De Winne, Kaat Van Casteren, Elien Augustus, Julie Jacobs, Xiang Hua Zhang, Daniëlla Galdermans, Els De Droogh, Anneke Lefebure, and et al. 2018. "A Multicenter Study to Assess EGFR Mutational Status in Plasma: Focus on an Optimized Workflow for Liquid Biopsy in a Clinical Setting" Cancers 10, no. 9: 290. https://doi.org/10.3390/cancers10090290
APA StyleSorber, L., Zwaenepoel, K., De Winne, K., Van Casteren, K., Augustus, E., Jacobs, J., Zhang, X. H., Galdermans, D., De Droogh, E., Lefebure, A., Morel, A.-M., Saenen, E., Bustin, F., Demedts, I., Himpe, U., Pieters, T., Germonpré, P., Derijcke, S., Deschepper, K., ... Pauwels, P. (2018). A Multicenter Study to Assess EGFR Mutational Status in Plasma: Focus on an Optimized Workflow for Liquid Biopsy in a Clinical Setting. Cancers, 10(9), 290. https://doi.org/10.3390/cancers10090290