High-Dose-Rate Brachytherapy Monotherapy versus Image-Guided Intensity-Modulated Radiotherapy with Helical Tomotherapy for Patients with Localized Prostate Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
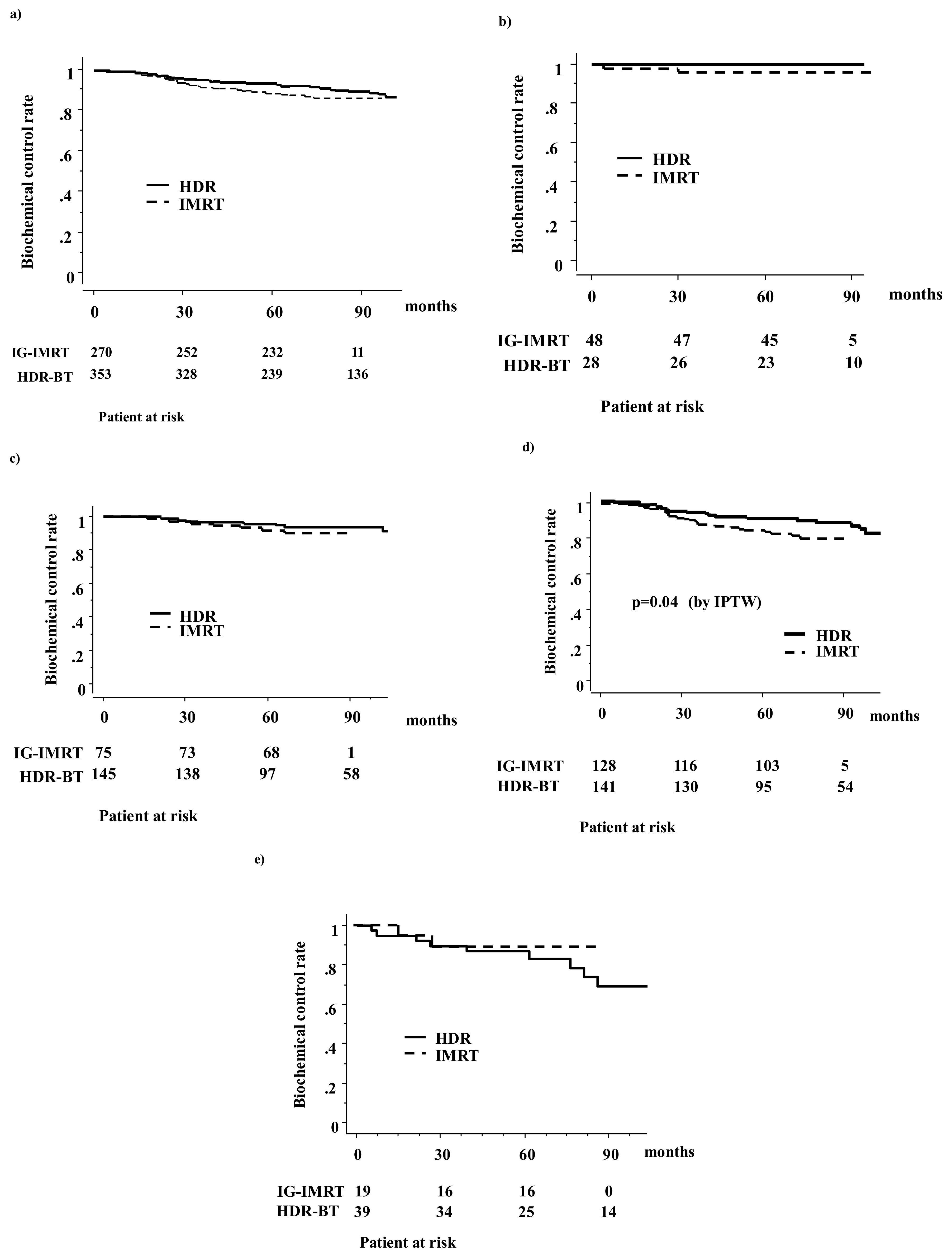
2.2. Biochemical Control and Survival
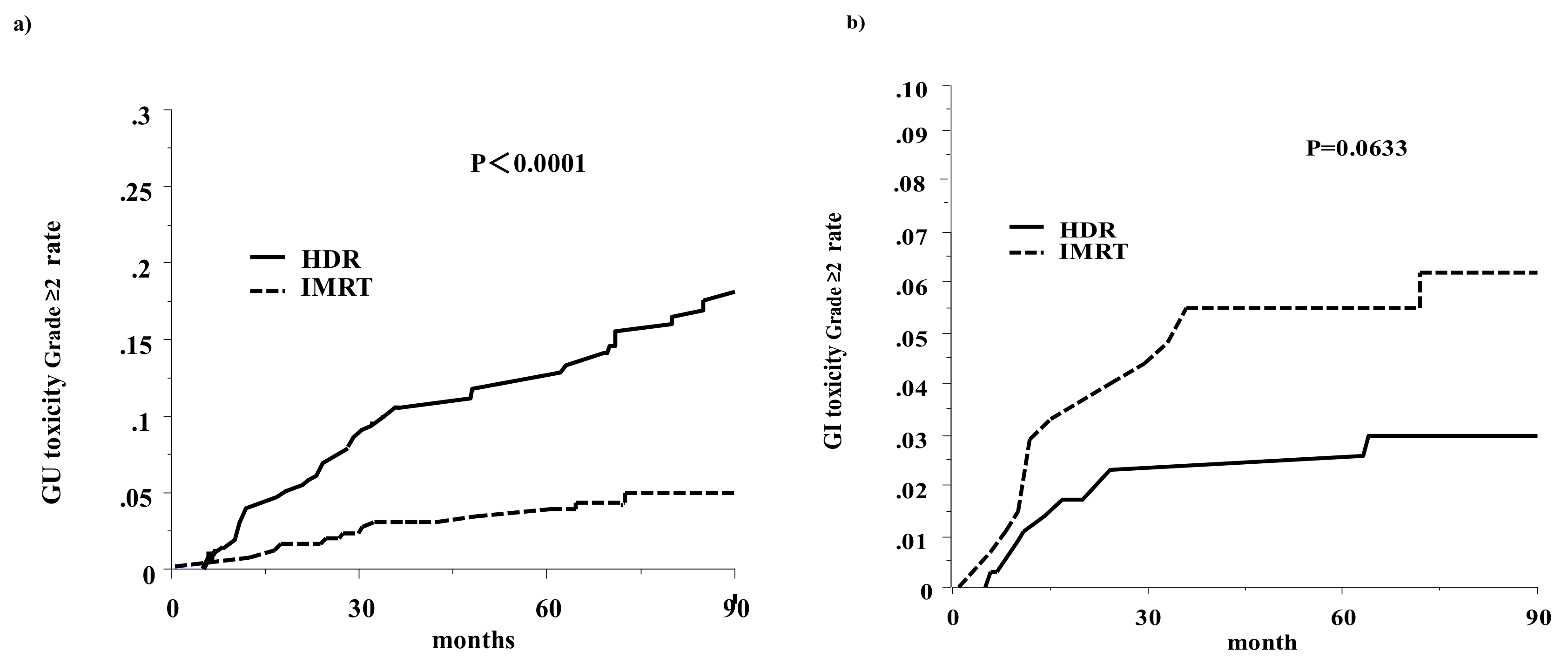
2.3. Late Toxicity
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment Planning
4.2.1. Image-Guided Intensity-Modulated Radiotherapy
4.2.2. High-Dose-Rate Interstitial Brachytherapy Monotherapy
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); Prostate Cancer 2016 Version 4; National Comprehensive Cancer Network: Fort Washington, PA, USA, 2016. [Google Scholar]
- Zelefsky, M.J.; Levin, E.J.; Hunt, M.; Yamada, Y.; Shippy, A.M.; Jackson, A.; Amols, H.I. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Zelefsky, M.J.; Kollmeier, M.; Cox, B.; Fidaleo, A.; Sperling, D.; Pei, X.; Carver, B.; Coleman, J.; Lovelock, M.; Huntm, M. Improved clinical outcomes with high-dose image guided radiotherapy compared with non-IGRT for the treatment of clinically localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Nakamura, S.; Nishimura, T.; Yoshida, K.; Yoshioka, Y.; Koizumi, M.; Ogawa, K. Transitioning from conventional radiotherapy to intensity-modulated radiotherapy for localized prostate cancer: Changing focus from rectal bleeding to detailed quality of life analysis. J. Radiat. Res. 2014, 55, 1033–1047. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, N.; Yamazaki, H.; Shimizu, D.; Suzuki, G.; Masui, K.; Nakamura, S.; Okabe, H.; Nishikawa, T.; Yoshida, K. Long-term outcomes of a dose-reduction trial to decrease late gastrointestinal toxicity in patients with prostate cancer receiving soft tissue-matched Image-guided intensity-modulated radiotherapy. Anticancer Res. 2018, 38, 385–391. [Google Scholar] [PubMed]
- Shimizu, D.; Yamazaki, H.; Nishimura, T.; Aibe, N.; Okabe, H. Long-term tumor control and late toxicity in patients with prostate cancer receiving hypofractionated (2.2 Gy) Soft-tissue-matched image-guided intensity-modulated radiotherapy. Anticancer Res. 2017, 37, 5829–5835. [Google Scholar] [PubMed]
- Chin, J.; Rumble, R.B.; Kollmeier, M.; Heath, E.; Efstathiou, J.; Dorff, T.; Berman, B.; Feifer, A.; Jacques, A.; Loblaw, D.A.; et al. Brachytherapy for Patients with Prostate Cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update. J. Clin. Oncol. 2017, 35, 1737–1743. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, Y.; Nose, T.; Yoshida, K.; Inoue, T.; Yamazaki, H.; Tanaka, E.; Shiomi, H.; Imai, A.; Nakamura, S.; Shimamoto, S.; et al. High-dose-rate interstitial brachytherapy as a monotherapy for localized prostate cancer: Treatment description and preliminary results of a phase I/II clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Yamazaki, H.; Takenaka, T.; Kotsuma, T.; Yoshida, M.; Masui, K.; Yoshioka, Y.; Narumi, Y.; Oka, T.; Tanaka, E. High-dose-rate interstitial brachytherapy in combination with androgen deprivation therapy for prostate cancer: Are high-risk patients good candidates? Strahlenther. Onkol. 2014, 190, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Zamboglou, N.; Tselis, N.; Baltas, D.; Buhleier, T.; Martin, T.; Milickovic, N.; Papaioannou, S.; Ackermann, H.; Tunn, U.W. High-dose-rate interstitial brachytherapy as monotherapy for clinically localized prostate cancer: Treatment evolution and mature results. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, P.; Rojas, A.; Lowe, G.; Bryant, L.; Ostler, P.; Hughes, R.; Milner, J.; Cladd, H. High-dose-rate brachytherapy alone for localized prostate cancer in patients at moderate or high risk of biochemical recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Morris, W.J.; Tyldesley, S.; Rodda, S.; Halperin, R.; Pai, H.; McKenzie, M.; Duncan, G.; Morton, G.; Hamm, J.; Murray, N. Androgen suppression combined with elective nodal and dose escalated radiation therapy (the ASCENDE-RT Trial): An analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high- and intermediate-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 275–285. [Google Scholar] [PubMed]
- Sathya, J.R.; Davis, I.R.; Julian, J.A.; Guo, Q.; Daya, D.; Dayes, I.S.; Lukka, H.R.; Levine, M. Randomized trial comparing iridium implant plus external-beam radiation therapy with external-beam radiation therapy alone in node-negative locally advanced cancer of the prostate. J. Clin. Oncol. 2005, 23, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, P.J.; Rojas, A.M.; Bownes, P.J.; Lowe, G.J.; Ostler, P.J.; Bryant, L. Randomized trial of external beam radiotherapy alone or combined with high-dose-rate brachytherapy boost for localized prostate cancer. Radiother. Oncol. 2012, 103, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Grimm, P.; Billiet, I.; Bostwick, D.; Dicker, A.P.; Frank, S.; Immerzeel, J.; Keyes, M.; Kupelian, P.; Lee, W.R.; Machtens, S.; et al. Comparative analysis of prostate-specific antigen free survival outcomes for patients with low, intermediate and high risk prostate cancer treatment by radical therapy. Results from the Prostate Cancer Results Study Group. BJU Int. 2012, 109 (Suppl. 1), 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spratt, D.E.; Soni, P.D.; McLaughlin, P.W.; Merrick, G.S.; Stock, R.G.; Blasko, J.C.; Zelefsky, M.J. American Brachytherapy Society Task Group Report: Combination of brachytherapy and external beam radiation for high-risk prostate cancer. Brachytherapy 2017, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, Y.; Kotsuma, T.; Komiya, A.; Kariya, S.; Konishi, K.; Nonomura, N.; Ogawa, K.; Tanaka, E.; Nishimura, K.; Fujiuchi, Y.; et al. Nationwide, Multicenter, Retrospective Study on High-Dose-Rate Brachytherapy as Monotherapy for Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Zhao, N.; Liao, A.; Wang, H.; Qu, A. Dosimetric and radiobiological comparison of volumetric modulated arc therapy, high-dose rate brachytherapy, and low-dose rate permanent seeds implant for localized prostate cancer. Med. Dosim. 2016, 41, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Pieters, B.R.; de Back, D.Z.; Koning, C.C.; Zwinderman, A.H. Comparison of three radiotherapy modalities on biochemical control and overall survival for the treatment of prostate cancer: A systematic review. Radiother. Oncol. 2009, 93, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Spratt, D.E.; Zumsteg, Z.S.; Ghadjar, P.; Kollmeier, M.A.; Pei, X.; Cohen, G.; Polkinghorn, W.; Yamada, Y.; Zelefsky, M.J. Comparison of high-dose (86.4 Gy) IMRT vs combined brachytherapy plus IMRT for intermediate-risk prostate cancer. BJU Int. 2014, 114, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Yamaguchi, T.; Hachiya, K.; Kamei, S.; Ishihara, S.; Hayashi, M.; Ogawa, S.; Nishibori, H.; Goshima, S.; Matsuo, M. Treatment outcomes and late toxicities of intensity-modulated radiation therapy for 1091 Japanese patients with localized prostate cancer. Rep. Pract. Oncol. Radiother. 2018, 23, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Masui, K.; Suzuki, G.; Nakamura, S.; Yoshida, K.; Kotsuma, T.; Tanaka, E.; Otani, K.; Yoshioka, Y.; Ogawa, K. Comparison of three moderate fractionated schedules employed in high-dose-rate brachytherapy monotherapy for clinically localized prostate cancer. Radiother. Oncol. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Budäus, L.; Bolla, M.; Bossi, A.; Cozzarini, C.; Crook, J.; Widmark, A.; Wiegel, T. Functional outcomes and complications following radiation therapy for prostate cancer: A critical analysis of the literature. Eur. Urol. 2012, 61, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Shaikh, T.; Ruth, K.; Sharda, P.; Hayes, S.B.; Sobczak, M.L.; Hallman, M.A.; Smaldone, M.C.; Chen, D.Y.T.; Horwitz, E.M. Prostate Cancer Patients with Unmanaged Diabetes or Receiving Insulin Experience Inferior Outcomes and Toxicities after Treatment with Radiation Therapy. Clin. Genitourin. Cancer 2017, 15, 326–335. [Google Scholar] [CrossRef] [PubMed]
- R-Project Home Page. Available online: https://www.r-project.org/ (accessed on 2 February 2018).



{kind=link}
{kind=link}
| Variables | Strata | IG-IMRT | HDR-BT | p-Value | |||
|---|---|---|---|---|---|---|---|
| n = 270 | n = 353 | ||||||
| No. or Median (range) | (%) | No. or Median (range) | (%) | ||||
| Age | 71 (47–86) | 71 (51–86) | 0.001 | ||||
| T category | 1 | 87 | (32%) | 95 | (27%) | 0.057 | |
| 2 | 118 | (44%) | 155 | (44%) | |||
| 3 | 64 | (24%) | 94 | (27%) | |||
| 4 | 1 | (0.4%) | 9 | (3%) | |||
| Pretreatment PSA | ng/mL | 11.82 (1.971–658) | 9.7 (4–265) | 0.002 | |||
| Gleason score | ≤6 | 86 | (32%) | 117 | (33%) | 0.0002 | |
| 7 | 77 | (29%) | 147 | (42%) | |||
| 8≤ | 107 | (40%) | 89 | (25%) | |||
| NCCN risk classification | Low | 48 | (18%) | 28 | (8%) | <0.0001 | |
| Intermediate | 75 | (28%) | 145 | (41%) | |||
| High | 128 | (47%) | 141 | (40%) | |||
| Very high | 19 | (7%) | 39 | (11%) | |||
| Prescribed dose | 74.8 Gy | 102 | (38%) | 45.5 Gy | 86 | (24%) | NA |
| 72.6 Gy | 24 | (9%) | 49 Gy | 148 | (42%) | ||
| 74 Gy | 119 | (44%) | 54 Gy | 111 | (31%) | ||
| 72 Gy | 25 | (9%) | Others | 8 | (2%) | ||
| 74.8 Gy | 102 | (38%) | |||||
| Hormonal therapy | Yes | 176 | (65%) | 275 | (78%) | 0.0005 | |
| No | 94 | (35%) | 78 | (22%) | |||
| Follow-up | Months | 74 (24–97) | 84 (19–216) | 0.001 | |||
| Variable | Strata | PT No. | IG-IMRT | PT No. | HDR-BT | p-Value | |
|---|---|---|---|---|---|---|---|
| Law Value | IPTW Correction | ||||||
| NCCN risk classification | Low | 48 | 95.8% | 28 | 100.0% | 0.28 | 0.15 |
| Intermediate | 75 | 92.0% | 145 | 95.6% | 0.42 | 0.6 | |
| High | 128 | 84.9% | 141 | 90.4% | 0.1 | 0.04 | |
| Very high | 19 | 87.1% | 39 | 89.2% | 0.38 | 0.6 | |
| Total | 270 | 92.9% | 353 | 89.1% | 0.18 | 0.07 | |
| Variable | Strata | Biochemical Control | |||||
|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | ||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age, years | <72 | 1 | (referent) | - | 1 | (referent) | - |
| 72≤ | 0.62 | 0.38–1.02 | 0.06 | 0.64 | 0.39–1.07 | 0.09 | |
| T category | T1–2 | 1 | (referent) | - | 1.00 | (referent) | - |
| T3–4 | 2.36 | 1.49–3.75 | 0.0003 | 1.97 | 1.08–3.49 | 0.02 | |
| Gleason score | ≤7 | 1 | (referent) | - | 1.00 | (referent) | - |
| 8≤ | 2.36 | 1.49–3.75 | 0.0003 | 1.97 | 1.08–3.49 | 0.02 | |
| Pretreatment PSA (ng/mL) | <20 | 1 | (referent) | - | 1.00 | (referent) | - |
| 20≤ | 2.78 | 1.75–4.41 | <0.0001 | 2.53 | 1.44–4.44 | 0.001 | |
| NCCN risk classification | Low–Intermediate | 1 | (referent) | - | NA | ||
| High–Very high | 2.85 | 1.67–4.87 | 0.0001 | ||||
| Hormonal therapy | No | 1 | (referent) | - | 1.00 | (referent) | - |
| Yes | 0.95 | 0.56–1.59 | 0.84 | 1.88 | 0.98–3.57 | 0.054 | |
| Treatment modality | HDR-BT | 1 | (referent) | - | 1.00 | (referent) | - |
| IG-IMRT | 1.38 | 0.85–2.24 | 0.18 | 0.65 | 0.39–1.08 | 0.10 | |
| Toxicities | Strata | IG-IMRT | HDR-BT | p-Value | ||
|---|---|---|---|---|---|---|
| n = 270 | n = 353 | |||||
| No. | (%) | No. | (%) | |||
| Gastrointestinal | 0 | 224 | (83%) | 310 | (87%) | 0.094 |
| 1 | 30 | (11%) | 33 | (9%) | ||
| 2 | 11 | (4%) | 10 | (3%) | ||
| 3 | 5 | (2%) | 1 | (0.3%) | ||
| Genitourinary | 0 | 222 | (82%) | 186 | (52%) | <0.0001 |
| 1 | 36 | (13%) | 100 | (28%) | ||
| 2 | 11 | (4%) | 57 | (16%) | ||
| 3 | 1 | (0%) | 10 | (3%) | ||
| Variable | Strata | Genitourinary Toxicity Grade ≥ 2 | |||||
|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | ||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age, years | 1.004 | 0.97–1.03 | 0.80 | 1.016 | 0.98–1.05 | 0.36 | |
| NCCN risk classification | Low–Intermediate | 1 | (referent) | 1 | (referent) | ||
| High–Very high | 0.86 | 0.55–1.34 | 0.51 | 0.925 | 0.57–1.43 | 0.75 | |
| Hormonal therapy | No | 1 | (referent) | - | 1 | (referent) | |
| Yes | 1.055 | 062–1.77 | 0.83 | 0.89 | 0.50–1.57 | 0.69 | |
| Treatment modality | HDR-BT | 1 | (referent) | 1 | (referent) | ||
| IG-IMRT | 3.747 | 2.00–7.00 | <0.0001 | 3.91 | 2.07–7.39 | <0.0001 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Masui, K.; Suzuki, G.; Nakamura, S.; Shimizu, D.; Nishikawa, T.; Okabe, H.; Yoshida, K.; Kotsuma, T.; Tanaka, E.; et al. High-Dose-Rate Brachytherapy Monotherapy versus Image-Guided Intensity-Modulated Radiotherapy with Helical Tomotherapy for Patients with Localized Prostate Cancer. Cancers 2018, 10, 322. https://doi.org/10.3390/cancers10090322
Yamazaki H, Masui K, Suzuki G, Nakamura S, Shimizu D, Nishikawa T, Okabe H, Yoshida K, Kotsuma T, Tanaka E, et al. High-Dose-Rate Brachytherapy Monotherapy versus Image-Guided Intensity-Modulated Radiotherapy with Helical Tomotherapy for Patients with Localized Prostate Cancer. Cancers. 2018; 10(9):322. https://doi.org/10.3390/cancers10090322
Chicago/Turabian StyleYamazaki, Hideya, Koji Masui, Gen Suzuki, Satoaki Nakamura, Daisuke Shimizu, Tatsuyuki Nishikawa, Haruumi Okabe, Ken Yoshida, Tadayuki Kotsuma, Eiichi Tanaka, and et al. 2018. "High-Dose-Rate Brachytherapy Monotherapy versus Image-Guided Intensity-Modulated Radiotherapy with Helical Tomotherapy for Patients with Localized Prostate Cancer" Cancers 10, no. 9: 322. https://doi.org/10.3390/cancers10090322