

Peripheral Soluble Immune Checkpoint-Related Proteins Were Associated with Survival and Treatment Efficacy of Osteosarcoma Patients, a Cohort Study
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Baseline Data Collection, Patient Follow-Up, and Outcomes
2.3. Detection of Soluble ICK-Related Proteins in Plasma
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
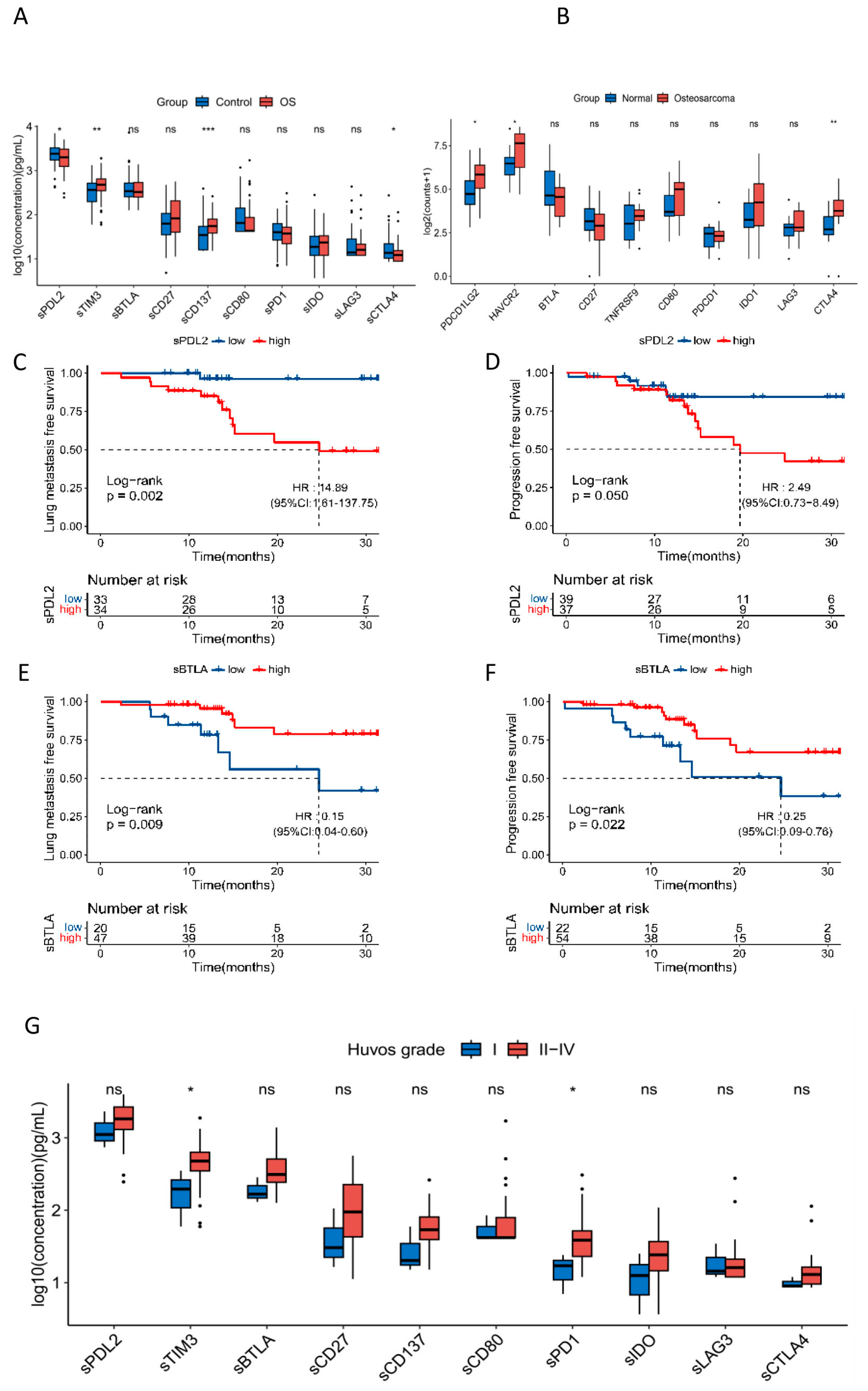
3.2. Soluble ICK-Related Proteins Were Associated with the Susceptibility of OS
3.3. Soluble ICK-Related Proteins Were Associated with Lung Metastasis and Treatment Efficacy of OS Patients
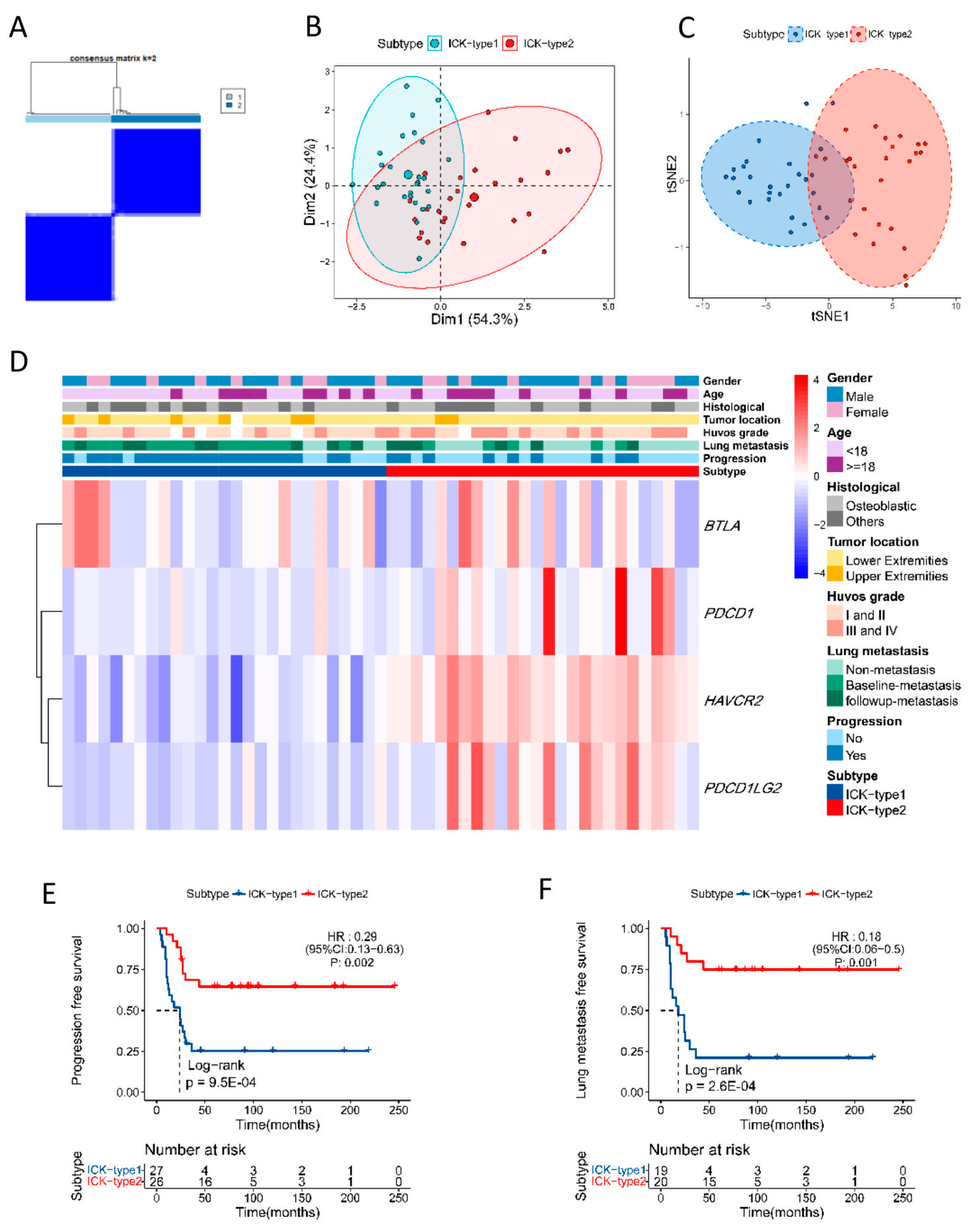
3.4. Immune Subtype of OS Based on Soluble ICK-Related Proteins
3.5. Functional Exploration of Immune Subtypes in OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cole, S.; Gianferante, D.M.; Zhu, B.; Mirabello, L. Osteosarcoma: A Surveillance, Epidemiology, and End Results program-based analysis from 1975 to 2017. Cancer 2022, 128, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- Sarcoma, Soft Tissue: Statistics. Available online: https://www.cancer.net/cancer-types/sarcoma-soft-tissue/statistics (accessed on 20 September 2020).
- Bao, P.; Zhou, Y.; Lu, W.; Wu, C.; Wang, C.; Sun, Y.; Zhang, C.; Xiao, J.; Lu, J.; Kong, L.; et al. Incidence and Mortality of Sarcomas in Shanghai, China, During 2002–2014. Front. Oncol. 2019, 9, 662. [Google Scholar] [CrossRef]
- Stiller, C.; Craft, A.; Corazziari, I.; Group, E.W. Survival of children with bone sarcoma in Europe since 1978: Results from the EUROCARE study. Eur. J. Cancer 2001, 37, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Mialou, V.; Philip, T.; Kalifa, C.; Perol, D.; Gentet, J.C.; Marec-Berard, P.; Pacquement, H.; Chastagner, P.; Defaschelles, A.S.; Hartmann, O. Metastatic osteosarcoma at diagnosis: Prognostic factors and long-term outcome—The French pediatric experience. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2005, 104, 1100–1109. [Google Scholar] [CrossRef]
- Link, M.P.; Goorin, A.M.; Miser, A.W.; Green, A.A.; Pratt, C.B.; Belasco, J.B.; Pritchard, J.; Malpas, J.S.; Baker, A.R.; Kirkpatrick, J.A.; et al. The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N. Engl. J. Med. 1986, 314, 1600–1606. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]
- Meltzer, P.S.; Helman, L.J. New Horizons in the Treatment of Osteosarcoma. N. Engl. J. Med. 2021, 385, 2066–2076. [Google Scholar] [CrossRef]
- Birdi, H.K.; Jirovec, A.; Cortes-Kaplan, S.; Werier, J.; Nessim, C.; Diallo, J.S.; Ardolino, M. Immunotherapy for sarcomas: New frontiers and unveiled opportunities. J. Immunother. Cancer 2021, 9, e001580. [Google Scholar] [CrossRef] [PubMed]
- Le Cesne, A.; Marec-Berard, P.; Blay, J.Y.; Gaspar, N.; Bertucci, F.; Penel, N.; Bompas, E.; Cousin, S.; Toulmonde, M.; Bessede, A.; et al. Programmed cell death 1 (PD-1) targeting in patients with advanced osteosarcomas: Results from the PEMBROSARC study. Eur. J. Cancer 2019, 119, 151–157. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- Sorenson, L.; Fu, Y.; Hood, T.; Warren, S.; McEachron, T.A. Targeted transcriptional profiling of the tumor microenvironment reveals lymphocyte exclusion and vascular dysfunction in metastatic osteosarcoma. Oncoimmunology 2019, 8, e1629779. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Ao, X.; Yang, Y.; Chen, Z.; Xu, X. Soluble immune checkpoints in cancer: Production, function and biological significance. J. Immunother. Cancer 2018, 6, 132. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; He, Y.; Li, W.; Xu, X.; Hu, Q.; Bian, Z.; Xu, A.; Tu, H.; Wu, M.; Wu, X. Soluble immune checkpoint-related proteins in blood are associated with invasion and progression in non-small cell lung cancer. Front. Immunol. 2022, 13, 887916. [Google Scholar] [CrossRef]
- Wang, Q.; Ye, Y.; Yu, H.; Lin, S.-H.; Tu, H.; Liang, D.; Chang, D.W.; Huang, M.; Wu, X. Immune checkpoint-related serum proteins and genetic variants predict outcomes of localized prostate cancer, a cohort study. Cancer Immunol. Immunother. 2021, 70, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Arooj, S.; Wang, H. Soluble B7-CD28 Family Inhibitory Immune Checkpoint Proteins and Anti-Cancer Immunotherapy. Front. Immunol. 2021, 12, 651634. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, J.; Tu, H.; Liang, D.; Chang, D.; Ye, Y.; Wu, X. Soluble immune checkpoint-related proteins as predictors of tumor recurrence, survival, and T cell phenotypes in clear cell renal cell carcinoma patients. J. Immunother. Cancer 2019, 7, 334. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Asanuma, K.; Yoshida, K.; Hagi, T.; Iino, T.; Nakamura, T.; Sudo, A. The role of soluble CD80 in patients with soft tissue tumors. J. Orthop. Surg. Res. 2022, 17, 404. [Google Scholar] [CrossRef] [PubMed]
- Meftahpour, V.; Aghebati-Maleki, A.; Fotouhi, A.; Safarzadeh, E.; Aghebati-Maleki, L. Prognostic significance and therapeutic potentials of immune checkpoints in osteosarcoma. EXCLI J. 2022, 21, 250–268. [Google Scholar] [CrossRef] [PubMed]
- Jawad, M.U.; Scully, S.P. In brief: Classifications in brief: Enneking classification: Benign and malignant tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 2010, 468, 2000–2002. [Google Scholar] [CrossRef]
- Rosen, G.; Caparros, B.; Huvos, A.G.; Kosloff, C.; Nirenberg, A.; Cacavio, A.; Marcove, R.C.; Lane, J.M.; Mehta, B.; Urban, C. Preoperative chemotherapy for osteogenic sarcoma: Selection of postoperative adjuvant chemotherapy based on the response of the primary tumor to preoperative chemotherapy. Cancer 1982, 49, 1221–1230. [Google Scholar] [CrossRef]
- Walsh, C.P.; Lindsay, E.K.; Grosse, P.; Natale, B.N.; Fairlie, S.; Bwint, A.; Schaffer, L.; McMahon, K.; Del Duke, C.; Forse, J.; et al. A systematic review and meta-analysis of the stability of peripheral immune markers in healthy adults. Brain Behav. Immun. 2023, 107, 32–46. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, K.; Shahmoradgoli, M.; Martinez, E.; Vegesna, R.; Kim, H.; Torres-Garcia, W.; Trevino, V.; Shen, H.; Laird, P.W.; Levine, D.A.; et al. Inferring tumour purity and stromal and immune cell admixture from expression data. Nat. Commun. 2013, 4, 2612. [Google Scholar] [CrossRef] [PubMed]
- Ning, Z.; Liu, K.; Xiong, H. Roles of BTLA in Immunity and Immune Disorders. Front. Immunol. 2021, 12, 654960. [Google Scholar] [CrossRef]
- Quan, L.; Lan, X.; Meng, Y.; Guo, X.; Guo, Y.; Zhao, L.; Chen, X.; Liu, A. BTLA marks a less cytotoxic T-cell subset in diffuse large B-cell lymphoma with high expression of checkpoints. Exp. Hematol. 2018, 60, 47–56.e1. [Google Scholar] [CrossRef] [PubMed]
- Fourcade, J.; Sun, Z.; Pagliano, O.; Guillaume, P.; Luescher, I.F.; Sander, C.; Kirkwood, J.M.; Olive, D.; Kuchroo, V.; Zarour, H.M. CD8+ T cells specific for tumor antigens can be rendered dysfunctional by the tumor microenvironment through upregulation of the inhibitory receptors BTLA and PD-1. Cancer Res. 2012, 72, 887–896. [Google Scholar] [CrossRef]
- Bian, B.; Fanale, D.; Dusetti, N.; Roque, J.; Pastor, S.; Chretien, A.S.; Incorvaia, L.; Russo, A.; Olive, D.; Iovanna, J. Prognostic significance of circulating PD-1, PD-L1, pan-BTN3As, BTN3A1 and BTLA in patients with pancreatic adenocarcinoma. Oncoimmunology 2019, 8, e1561120. [Google Scholar] [CrossRef]
- Han, L.; Wang, W.; Fang, Y.; Feng, Z.; Liao, S.; Li, W.; Li, Y.; Li, C.; Maitituoheti, M.; Dong, H.; et al. Correction: Soluble B and T Lymphocyte Attenuator Possesses Antitumor Effects and Facilitates Heat Shock Protein 70 Vaccine-Triggered Antitumor Immunity against a Murine TC-1 Cervical Cancer Model In Vivo. J. Immunol. 2020, 204, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Kraehenbuehl, L.; Weng, C.H.; Eghbali, S.; Wolchok, J.D.; Merghoub, T. Enhancing immunotherapy in cancer by targeting emerging immunomodulatory pathways. Nat. Rev. Clin. Oncol. 2022, 19, 37–50. [Google Scholar] [CrossRef]
- Wang, Y.; Du, J.; Gao, Z.; Sun, H.; Mei, M.; Wang, Y.; Ren, Y.; Zhou, X. Evolving landscape of PD-L2: Bring new light to checkpoint immunotherapy. Br. J. Cancer 2023, 128, 1196–1207. [Google Scholar] [CrossRef]
- Muraro, E.; Romano, R.; Fanetti, G.; Vaccher, E.; Turturici, I.; Lupato, V.; La Torre, F.B.; Polesel, J.; Fratta, E.; Giacomarra, V.; et al. Tissue and circulating PD-L2: Moving from health and immune-mediated diseases to head and neck oncology. Crit. Rev. Oncol. Hematol. 2022, 175, 103707. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, T.L. Tumor-Derived Exosomes and Their Role in Tumor-Induced Immune Suppression. Vaccines 2016, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhao, B.; Wang, X. Tumor infiltrating immune cells (TIICs) as a biomarker for prognosis benefits in patients with osteosarcoma. BMC Cancer 2020, 20, 1022. [Google Scholar] [CrossRef] [PubMed]
- Ren, T.; Zheng, B.; Huang, Y.; Wang, S.; Bao, X.; Liu, K.; Guo, W. Osteosarcoma cell intrinsic PD-L2 signals promote invasion and metastasis via the RhoA-ROCK-LIMK2 and autophagy pathways. Cell Death Dis. 2019, 10, 261. [Google Scholar] [CrossRef] [PubMed]
- Makkouk, A.; Chester, C.; Kohrt, H.E. Rationale for anti-CD137 cancer immunotherapy. Eur. J. Cancer 2016, 54, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Wang, L.; Wu, C.; Huang, L.; Ruan, Y.; Xue, W. Tumor-derived Exosomes Induced M2 Macrophage Polarization and Promoted the Metastasis of Osteosarcoma Cells Through Tim-3. Arch. Med. Res. 2021, 52, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Cao, Y.; Wang, Z.; Zhang, T.; Hua, Y.; Cai, Z. Identification of two immune subtypes in osteosarcoma based on immune gene sets. Int. Immunopharmacol. 2021, 96, 107799. [Google Scholar] [CrossRef]
- Genova, C.; Dellepiane, C.; Carrega, P.; Sommariva, S.; Ferlazzo, G.; Pronzato, P.; Gangemi, R.; Filaci, G.; Coco, S.; Croce, M. Therapeutic Implications of Tumor Microenvironment in Lung Cancer: Focus on Immune Checkpoint Blockade. Front. Immunol. 2021, 12, 799455. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Osteosarcoma (N = 76) | Health Control (N = 76) | p | ||
|---|---|---|---|---|
| Age | 0.09 | |||
| Mean (SD) | 25.62 (18.59) | 30.41 (15.45) | ||
| Gender | 1.00 | |||
| Female | 20 (26.32) | 20 (26.32) | ||
| Male | 56 (73.68) | 56 (73.68) | ||
| BMI | 0.01 | |||
| Mean (SD) | 20.90 (4.47) | 22.84 (4.90) | ||
| Missing | 0 (0.00) | 6 (7.89) | ||
| Tumor location | - | |||
| Extremities | 66 (86.84) | - | ||
| Non-extremities | 10 (13.16) | - | ||
| Tumor size | - | |||
| <8 cm | 43 (56.58) | - | ||
| ≥8 cm | 31 (40.79) | - | ||
| Missing | 2 (2.63) | - | ||
| Enneking stage | - | |||
| IB | 1 (1.32) | - | ||
| IIA | 4 (5.26) | - | ||
| IIB | 62 (81.58) | - | ||
| III | 9 (11.84) | - | ||
| Pathological fracture | - | |||
| Yes | 13 (17.11) | - | ||
| No | 63 (82.89) | - | ||
| Neoadjuvant chemotherapy | - | |||
| Yes | 62 (81.58) | - | ||
| No | 13 (17.11) | - | ||
| Missing | 1 (1.31) | - | ||
| Huvos grade | - | |||
| I | 3 (3.95) | - | ||
| II | 21 (27.63) | - | ||
| III | 23 (30.26) | - | ||
| IV | 12 (15.79) | - | ||
| Missing | 17 (22.37) | - | ||
| ALP level at diagnosis | <0.001 | |||
| <300 U/mL | 55 (72.37) | 56 (73.68) | ||
| ≥300 U/mL | 20 (26.32) | 0 (0.00) | ||
| Missing | 1(1.31) | 20 (26.32) | ||
| LDH level at diagnosis | 0.00 | |||
| ≤250 U/mL | 54 (71.05) | 45 (59.21) | ||
| >250 U/mL | 22 (28.95) | 1 (1.32) | ||
| Missing | 0 (0.00) | 30 (39.47) | ||
| Lung metastasis | - | |||
| Non-metastasis | 54 (71.05) | - | ||
| Baseline metastasis | 9 (11.84) | - | ||
| Follow-up metastasis | 13 (17.11) | - | ||
| Progression | ||||
| Yes | 19 (25.00) | - | ||
| No | 57 (75.00) | - | ||
| Dead | - | |||
| Yes | 8 (10.53) | - | ||
| No | 68 (89.47) | - | ||
| Markers | Univariable Logistic | Multivariable Logistic | ||
|---|---|---|---|---|
| High vs. Low a | OR (95%CI) | p Value | Adjusted OR (95%CI) b | p Value |
| sTIM3 | 2.11 (1.11–4.06) | 0.0239 | 2.29 (1.05–5.11) | 0.0392# |
| sCD137 | 2.94 (1.53–5.74) | 0.0013 | 2.72 (1.22–6.25) | 0.0158# |
| sCD27 | 1.37 (0.73–2.61) | 0.3309 | 1.59 (0.74–3.48) | 0.2394 |
| sCTLA4 | 0.53 (0.28–1.00) | 0.0526 | 0.35 (0.15–0.77) | 0.0112 |
| sIDO | 1.23 (0.65–2.34) | 0.5166 | 2.49 (1.13–5.68) | 0.0259 |
| sLAG3 | 1.53 (0.81–2.91) | 0.1952 | 1.58 (0.73–3.45) | 0.2473 |
| sBTLA | 0.90 (0.48–1.70) | 0.7456 | 1.10 (0.51–2.39) | 0.8113 |
| sCD80 | 0.66 (0.34–1.24) | 0.1952 | 0.65 (0.30–1.41) | 0.2765 |
| sPD1 | 0.81 (0.43–1.53) | 0.5166 | 0.94 (0.43–2.05) | 0.8825 |
| sPDL2 | 0.73 (0.38–1.38) | 0.3309 | 1.17 (0.53–2.58) | 0.7038 |
| Markers | Lung Metastasis | Progression | ||
|---|---|---|---|---|
| High vs. Low a | Adjusted HR (95%CI) b | p Value | Adjusted HR (95%CI) b | p Value |
| sTIM3 | 6.58 (0.99–43.9) | 0.052 | 4.40 (1.16–16.67) | 0.029 |
| sCD137 | 0.60 (0.16–2.31) | 0.459 | 0.88 (0.30–2.55) | 0.811 |
| sCD27 | 5.73 (1.11–29.67) | 0.037 | 2.61 (0.83–8.21) | 0.102 |
| sCTLA4 | 3.53 (0.89–14.07) | 0.074 | 1.66 (0.53–5.24) | 0.385 |
| sIDO | 3.34 (0.88–12.64) | 0.076 | 2.46 (0.84–7.17) | 0.099 |
| sLAG3 | 0.54 (0.16–1.85) | 0.325 | 0.68 (0.25–1.83) | 0.441 |
| sBTLA | 0.15 (0.04–0.60) | 0.007# | 0.25 (0.09–0.76) | 0.014# |
| sCD80 | 0.28 (0.07–1.23) | 0.092 | 0.50 (0.17–1.46) | 0.204 |
| sPD1 | 0.39 (0.11–1.39) | 0.145 | 0.37 (0.13–1.06) | 0.065 |
| sPDL2 | 14.89 (1.61–137.75) | 0.017# | 2.49 (0.73–8.49) | 0.145 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, B.; Wang, Q.; Luo, Y.; Wang, S.; Pan, S.; Zhao, W.; Ye, Z.; Wu, X. Peripheral Soluble Immune Checkpoint-Related Proteins Were Associated with Survival and Treatment Efficacy of Osteosarcoma Patients, a Cohort Study. Cancers 2024, 16, 1628. https://doi.org/10.3390/cancers16091628
Li B, Wang Q, Luo Y, Wang S, Pan S, Zhao W, Ye Z, Wu X. Peripheral Soluble Immune Checkpoint-Related Proteins Were Associated with Survival and Treatment Efficacy of Osteosarcoma Patients, a Cohort Study. Cancers. 2024; 16(9):1628. https://doi.org/10.3390/cancers16091628
Chicago/Turabian StyleLi, Binghao, Qinchuan Wang, Yihong Luo, Sicong Wang, Sai Pan, Wenting Zhao, Zhaoming Ye, and Xifeng Wu. 2024. "Peripheral Soluble Immune Checkpoint-Related Proteins Were Associated with Survival and Treatment Efficacy of Osteosarcoma Patients, a Cohort Study" Cancers 16, no. 9: 1628. https://doi.org/10.3390/cancers16091628