

Breast Tissue Restoration after the Partial Mastectomy Using Polycaprolactone Scaffold
 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Fabrication of PCL Scaffold for Patial Mastectomy
2.2. Mechanical Property of PCL Scaffold for Patial Mastectomy
2.3. PCL Scaffold Implantation after Patial Mastectomy in Rat Model
2.4. Histological Analysis
2.5. Evaluation of Soft Tissue Restoration within PCL Scaffold
2.6. Evaluation of Inflammation after PCL Scaffold Implantation
2.7. Alizarin Red S Staining after PCL Scaffold Implantation
2.8. Statistical Analysis
3. Results
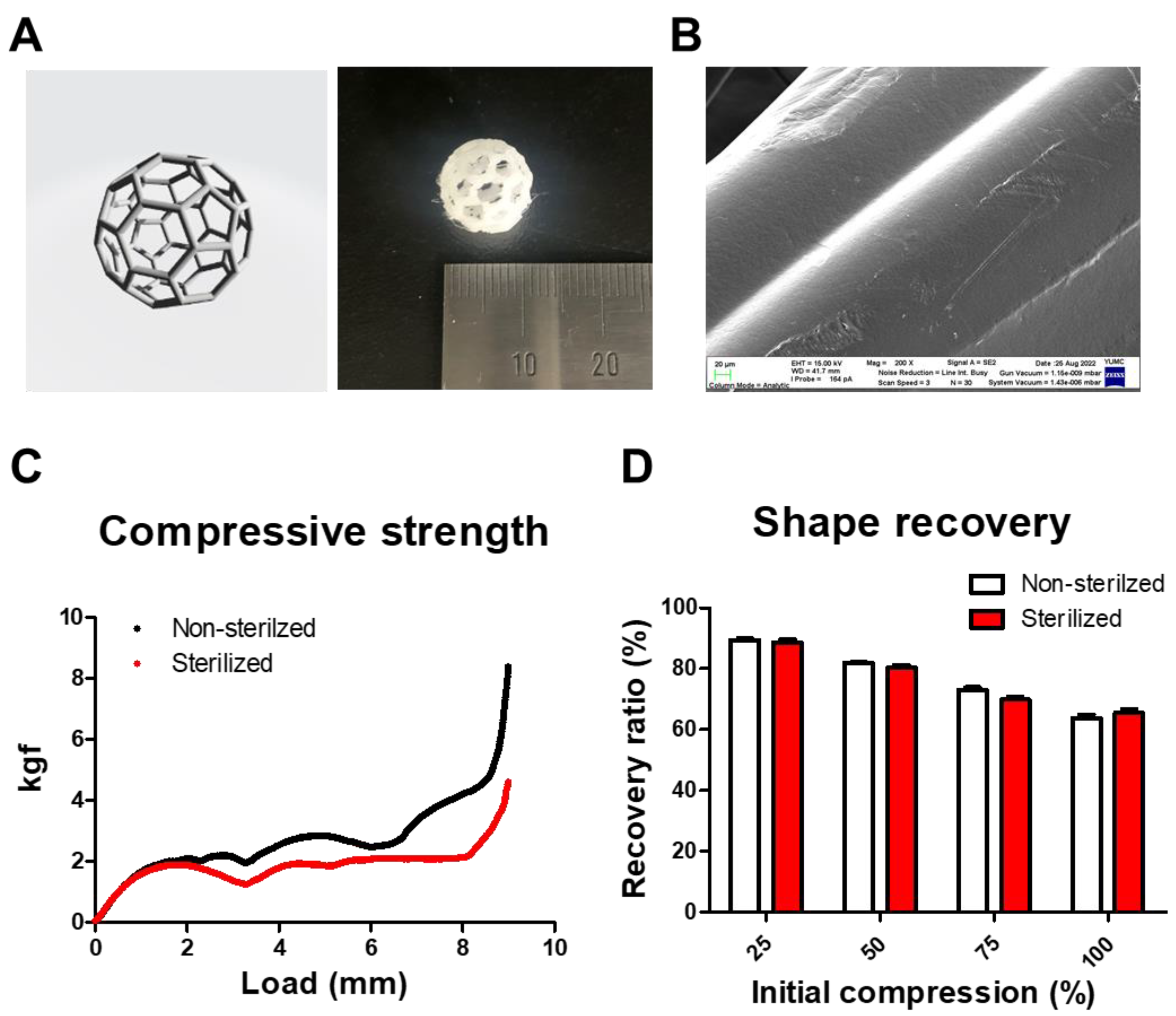
3.1. Fabrication and Mechanical Properties of PCL Scaffold
3.2. Time-Dependent Tissue Restoration after PCL Scaffold Implantation
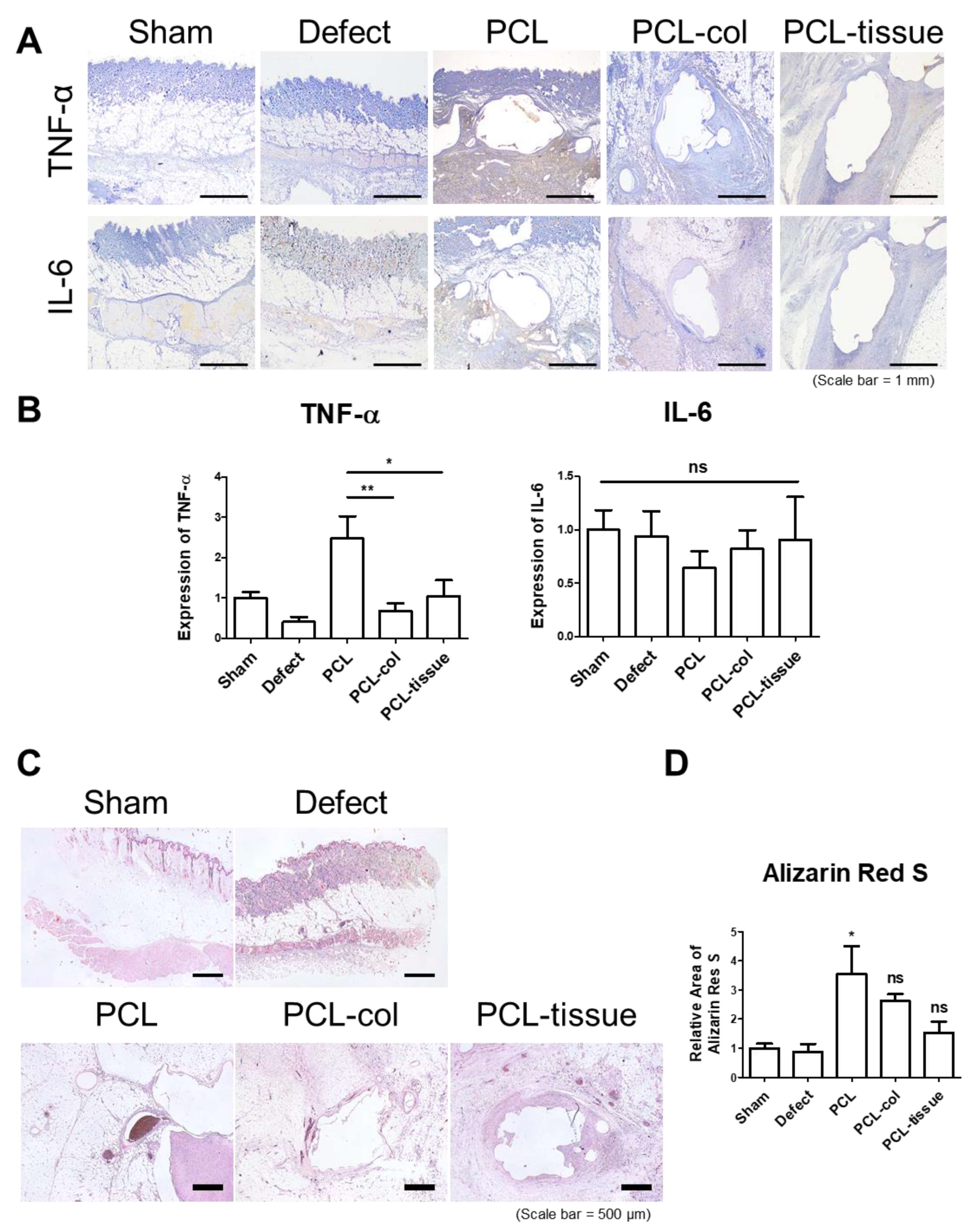
3.3. Histological Analysis after PCL Scaffold Implantation
3.4. Inflammatory Properties of PCL Scaffold
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Halsted, W.S.I. A Clinical and Histological Study of certain Adenocarcinomata of the Breast: And a Brief Consideration of the Supraclavicular Operation and of the Results of Operations for Cancer of the Breast from 1889 to 1898 at the Johns Hopkins Hospital. Ann. Surg. 1898, 28, 557–576. [Google Scholar]
- Feigenberg, Z.; Zer, M.; Dintsman, M. Comparison of postoperative complications following radical and modified radical mastectomy. World J. Surg. 1977, 2, 207–211. [Google Scholar] [CrossRef]
- Veronesi, U.; Saccozzi, R.; Del Vecchio, M.; Banfi, A.; Clemente, C.; De Lena, M.; Gallus, G.; Greco, M.; Luini, A.; Marubini, E.; et al. Comparing radical mastectomy with quadrantectomy, axillary dissection, and radiotherapy in patients with small cancers of the breast. N. Engl. J. Med. 1981, 305, 6–11. [Google Scholar] [CrossRef]
- Puls, T.J.; Fisher, C.S.; Cox, A.; Plantenga, J.M.; McBride, E.L.; Anderson, J.L.; Goergen, C.J.; Bible, M.; Moller, T.; Voytik-Harbin, S.L. Regenerative tissue filler for breast conserving surgery and other soft tissue restoration and reconstruction needs. Sci. Rep. 2021, 11, 2711. [Google Scholar] [CrossRef]
- Calabrese, C.; Casella, D.; Di Taranto, G.; Marcasciano, M.; Kothari, A.; Sordi, S.; Barellini, L.; Lo Torto, F.; Tarallo, M.; Perra, A.; et al. Oncoplastic conservative surgery for breast cancer: Long-term outcomes of our first ten years experience. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 7333–7342. [Google Scholar] [CrossRef]
- Piper, M.; Peled, A.W.; Sbitany, H. Oncoplastic breast surgery: Current strategies. Gland Surg. 2015, 4, 154–163. [Google Scholar] [CrossRef]
- Hamdi, M.; Wolfli, J.; Van Landuyt, K. Partial mastectomy reconstruction. Clin. Plast. Surg. 2007, 34, 51–62, abstract vi. [Google Scholar] [CrossRef]
- Palama, I.E.; Arcadio, V.; D’Amone, S.; Biasiucci, M.; Gigli, G.; Cortese, B. Therapeutic PCL scaffold for reparation of resected osteosarcoma defect. Sci. Rep. 2017, 7, 12672. [Google Scholar] [CrossRef]
- Esposito, A.R.; Moda, M.; Cattani, S.M.; de Santana, G.M.; Barbieri, J.A.; Munhoz, M.M.; Cardoso, T.P.; Barbo, M.L.; Russo, T.; D’Amora, U.; et al. PLDLA/PCL-T Scaffold for Meniscus Tissue Engineering. Biores. Open Access 2013, 2, 138–147. [Google Scholar] [CrossRef]
- Elamparithi, A.; Punnoose, A.M.; Kuruvilla, S.; Ravi, M.; Rao, S.; Paul, S.F. Electrospun polycaprolactone matrices with tensile properties suitable for soft tissue engineering. Artif. Cells Nanomed. Biotechnol. 2016, 44, 878–884. [Google Scholar] [CrossRef]
- Baek, W.; Kim, M.S.; Park, D.B.; Joo, O.Y.; Lee, W.J.; Roh, T.S.; Sung, H.J. Three-Dimensionally Printed Breast Reconstruction Devices Facilitate Nanostructure Surface-Guided Healthy Lipogenesis. ACS Biomater. Sci. Eng. 2019, 5, 4962–4969. [Google Scholar] [CrossRef]
- Cai, Y.; Chen, Y.; Hong, X.; Liu, Z.; Yuan, W. Porous microsphere and its applications. Int. J. Nanomed. 2013, 8, 1111. [Google Scholar]
- Jin, S.; Gao, J.; Yang, R.; Yuan, C.; Wang, R.; Zou, Q.; Zuo, Y.; Zhu, M.; Li, Y.; Man, Y. A baicalin-loaded coaxial nanofiber scaffold regulated inflammation and osteoclast differentiation for vascularized bone regeneration. Bioact. Mater. 2022, 8, 559–572. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lim, H.; Ahn, J.W.; Jang, D.; Lee, S.H.; Park, K.; Kim, S.E. Design of a 3D BMP-2-Delivering Tannylated PCL Scaffold and Its Anti-Oxidant, Anti-Inflammatory, and Osteogenic Effects In Vitro. Int. J. Mol. Sci. 2018, 19, 3602. [Google Scholar] [CrossRef]
- Rather, H.A.; Patel, R.; Yadav, U.C.; Vasita, R. Dual drug-delivering polycaprolactone-collagen scaffold to induce early osteogenic differentiation and coupled angiogenesis. Biomed. Mater. 2020, 15, 045008. [Google Scholar] [CrossRef]
- Reichert, J.; Heymer, A.; Berner, A.; Eulert, J.; Nöth, U. Fabrication of polycaprolactone collagen hydrogel constructs seeded with mesenchymal stem cells for bone regeneration. Biomed. Mater. 2009, 4, 065001. [Google Scholar] [CrossRef]
- Teoh, S.-H.; Goh, B.-T.; Lim, J. Three-dimensional printed polycaprolactone scaffolds for bone regeneration success and future perspective. Tissue Eng. Part A 2019, 25, 931–935. [Google Scholar] [CrossRef]
- Cai, Y.; Li, J.; Poh, C.K.; Tan, H.C.; San Thian, E.; Fuh, J.Y.H.; Sun, J.; Tay, B.Y.; Wang, W. Collagen grafted 3D polycaprolactone scaffolds for enhanced cartilage regeneration. J. Mater. Chem. B 2013, 1, 5971–5976. [Google Scholar] [CrossRef]
- Jia, Z.; Li, H.; Cao, R.; Xiao, K.; Lu, J.; Zhao, D.; Wang, Z.; Zhang, Y.; Chen, J.; Zhang, W. Electrospun nanofibrous membrane of fish collagen/polycaprolactone for cartilage regeneration. Am. J. Transl. Res. 2020, 12, 3754. [Google Scholar]
- Gefen, A.; Dilmoney, B. Mechanics of the normal woman’s breast. Technol. Health Care 2007, 15, 259–271. [Google Scholar] [CrossRef]
- Peled, A.W.; Sbitany, H.; Foster, R.D.; Esserman, L.J. Oncoplastic mammoplasty as a strategy for reducing reconstructive complications associated with postmastectomy radiation therapy. Breast J. 2014, 20, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Janzekovic, J.; Wagels, M.; Hutmacher, D.W. Breast reconstruction using scaffold-based tissue engineering. In Breast Reconstruction; Springer: Berlin/Heidelberg, Germany, 2020; pp. 279–290. [Google Scholar]
- Chang, J.S.; Song, S.Y.; Oh, J.H.; Lew, D.H.; Roh, T.S.; Kim, S.Y.; Keum, K.C.; Lee, D.W.; Kim, Y.B. Influence of Radiation Dose to Reconstructed Breast Following Mastectomy on Complication in Breast Cancer Patients Undergoing Two-Stage Prosthetic Breast Reconstruction. Front. Oncol. 2019, 9, 243. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.; Chim, H.; Soltanian, H.T. The effects of neoadjuvant and adjuvant chemotherapy on the surgical outcomes of breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, e267–e280. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jwa, S.-J.; Won, J.-M.; Kim, D.-H.; Kim, K.-B.; Lee, J.-B.; Heo, M.; Shim, K.-S.; Jo, H.-S.; Lee, W.-J.; Roh, T.-S.; et al. Breast Tissue Restoration after the Partial Mastectomy Using Polycaprolactone Scaffold. Polymers 2022, 14, 3817. https://doi.org/10.3390/polym14183817
Jwa S-J, Won J-M, Kim D-H, Kim K-B, Lee J-B, Heo M, Shim K-S, Jo H-S, Lee W-J, Roh T-S, et al. Breast Tissue Restoration after the Partial Mastectomy Using Polycaprolactone Scaffold. Polymers. 2022; 14(18):3817. https://doi.org/10.3390/polym14183817
Chicago/Turabian StyleJwa, Seung-Jun, Jong-Min Won, Do-Hyun Kim, Ki-Bum Kim, Jung-Bok Lee, Min Heo, Kyu-Sik Shim, Han-Saem Jo, Won-Jai Lee, Tai-Suk Roh, and et al. 2022. "Breast Tissue Restoration after the Partial Mastectomy Using Polycaprolactone Scaffold" Polymers 14, no. 18: 3817. https://doi.org/10.3390/polym14183817