
Immune Responses of Healthy Pregnant Women following an Elective Cesarean Section: Effects of Anesthetic Procedures
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Sample Collection
2.3. Immunological Investigations
2.4. Ethical Issue
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Investigated Patients
3.2. Group Comparisons of the Cytokines, and Catecholamines
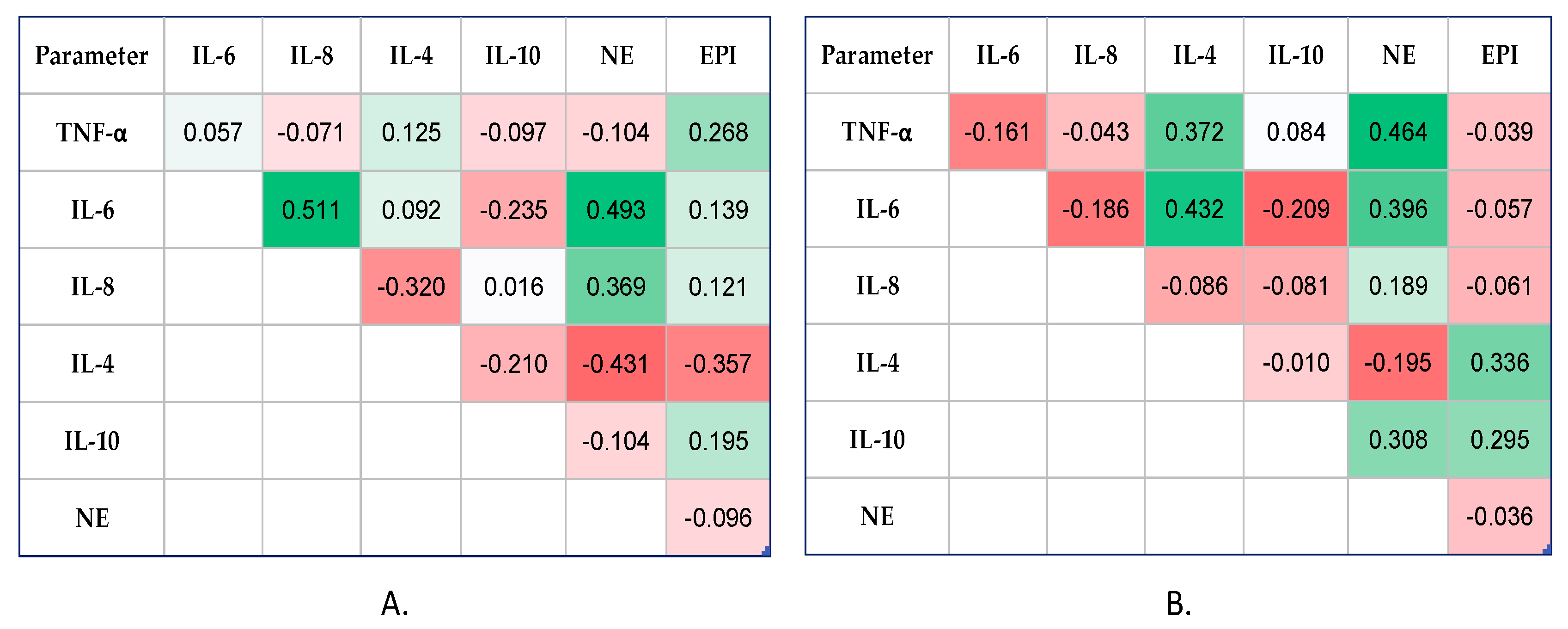
3.3. Catecholamines Serum Levels Associated Positively with Cytokines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manou-Stathopoulou, V.; Korbonits, M.; Ackland, G.L. Redefining the perioperative stress response: A narrative review. Br. J. Anaesth. 2019, 123, 570–583. [Google Scholar] [CrossRef] [PubMed]
- Cusack, B.; Buggy, D.J. Anaesthesia, analgesia, and the surgical stress response. BJA Educ. 2020, 20, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Chiasson, V.L.; Bounds, K.R.; Mitchell, B.M. Regulation of the Anti-Inflammatory Cytokines Interleukin-4 and Interleukin-10 during Pregnancy. Front. Immunol. 2014, 5, 253. [Google Scholar] [CrossRef] [PubMed]
- Pazos, M.; Sperling, R.S.; Moran, T.M.; Kraus, T.A. The influence of pregnancy on systemic immunity. Immunol. Res. 2012, 54, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Aldo, P.; Alvero, A.B. The unique immunological and microbial aspects of pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef]
- Manoharan, I.; Prasad, P.D.; Thangaraju, M.; Manicassamy, S. Lactate-Dependent Regulation of Immune Responses by Dendritic Cells and Macrophages. Front. Immunol. 2021, 12, 691134. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, P.; Chhabra, S. Physiological and anatomical changes of pregnancy: Implications for anaesthesia. Indian J. Anaesth. 2018, 62, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Rodrigues PR, S.; Zaher, S.; Davies, L.C.; Ghazal, P. Immune-metabolic adaptations in pregnancy: A potential stepping-stone to sepsis. EBioMedicine 2022, 86, 104337. [Google Scholar] [CrossRef] [PubMed]
- Racicot, K.; Kwon, J.Y.; Aldo, P.; Silasi, M.; Mor, G. Understanding the complexity of the immune system during pregnancy. Am. J. Reprod. Immunol. 2014, 72, 107–116. [Google Scholar] [CrossRef]
- O’Dwyer, M.J.; Owen, H.C.; Torrance, H.D. The perioperative immune response. Curr. Opin. Crit. Care 2015, 21, 336–342. [Google Scholar] [CrossRef]
- Kimura, F.; Shimizu, H.; Yoshidome, H.; Ohtsuka, M.; Miyazaki, M. Immunosuppression following surgical and traumatic injury. Surg. Today 2010, 40, 793–808. [Google Scholar] [CrossRef] [PubMed]
- Albertsmeier, M.; Prix, N.J.; Winter, H.; Bazhin, A.; Werner, J.; Angele, M.K. Monocyte-dependent suppression of T-cell function in postoperative patients and abdominal sepsis. Shock 2017, 48, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Ferland, C.E.; Parent, A.J.; Saran, N.; Ingelmo, P.M.; Lacasse, A.; Marchand, S.; Sarret, P.; Ouellet, J.A. Preoperative Norepinephrine Levels in Cerebrospinal Fluid and Plasma Correlate With Pain Intensity After Pediatric Spine Surgery. Spine Deform. 2017, 5, 325–333. [Google Scholar] [CrossRef]
- Tang, F.; Tie, Y.; Tu, C.; Wei, X. Surgical trauma-induced immunosuppression in cancer: Recent advances and the potential therapies. Clin. Transl. Med. 2020, 10, 199–223. [Google Scholar] [CrossRef] [PubMed]
- Novac, M.B.; Boldeanu, L.; Rotaru, L.T.; Dijmărescu, A.L.; Şerbănescu, M.S.; Radu, L.; Neamţu, S.D.; Vîlcea, A.M.; Niculescu, M.; Mirea, C.S.; et al. The perioperative effect of anesthetic drugs on the immune response in total intravenous anesthesia in patients undergoing minimally invasive gynecological surgery. Rom. J. Morphol. Embryol. 2021, 62, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Cruz, F.F.; Rocco, P.; Pelosi, P. Immunomodulators in anesthesia. Curr. Opin. Anaesthesiol. 2021, 34, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, J.; Qin, M.; Xu, M.; Luo, W.; Li, B.; Song, X.; Zhou, X. Effects of different anesthesia methods on postoperative immune function in patients undergoing gastrointestinal tumor resection. Sci. Rep. 2023, 13, 243. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Dong, T.; Zhang, J.; Li, J.; Lu, W. Effects of different methods of anesthesia and analgesia on immune function and serum tumor marker levels in critically ill patients. Exp. Ther. Med. 2017, 14, 2206–2210. [Google Scholar] [CrossRef]
- Lisowska, B.; Jakubiak, J.; Siewruk, K.; Sady, M.; Kosson, D. Which idea is better with regard to immune response? Opioid anesthesia or opioid free anesthesia. J. Inflamm. Res. 2020, 13, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Plein, L.M.; Rittner, H.L. Opioids and the immune system—Friend or foe. Br. J. Pharmacol. 2018, 175, 2717–2725. [Google Scholar] [CrossRef]
- Kalaycı, D.; Dikmen, B.; Kaçmaz, M.; Taşpınar, V.; Ornek, D.; Turan, O. Plasma levels of interleukin-10 and nitric oxide in response to two different desflurane anesthesia flow rates. Braz. J. Anesthesiol. 2014, 64, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Qin, Q.; Zhou, L.; Ouyang, W.; Li, Y.; Wu, Y.; Li, Y. Effects of fentanyl anesthesia and sufentanil anesthesia on regulatory T cells frequencies. Int. J. Clin. Exp. Pathol. 2014, 7, 7708–7716. [Google Scholar] [PubMed]
- Jafarzadeh, A.; Hadavi, M.; Hassanshahi, G.; Rezaeian, M.; Vazirinejad, R. General Anesthetics on Immune System Cytokines: A Narrative Review Article. Anesth. Pain Med. 2020, 10, e103033. [Google Scholar] [CrossRef] [PubMed]
- Simsek, E.; Karapinar, K.; Bugra, O.; Tulga Ulus, A.; Sarigul, A. Effects of albumin and synthetic polypeptide-coated oxygenators on IL-1, IL-2, IL-6, and IL-10 in open heart surgery. Asian J. Surg. 2014, 37, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.S.; Jang, J.S.; Hwang, S.M.; Tark, H.; Kim, J.H.; Lee, J.J. Effects of surgery start time on postoperative cortisol, inflammatory cytokines, and postoperative hospital day in hip surgery: Randomized controlled trial. Medicine (Baltimore) 2019, 98, e15820. [Google Scholar] [CrossRef] [PubMed]
- Vosoughian, M.; Dahi, M.; Dabir, S.; Moshari, M.; Tabashi, S.; Mosavi, Z. Effects of General Anesthesia Versus Spinal Anesthesia on Serum Cytokine Release After Cesarean Section: A Randomized Clinical Trial. Anesth. Pain Med. 2021, 11, e111272. [Google Scholar] [CrossRef] [PubMed]
- Jalal Rashid, K.; Bakir Karim, S.; Babakir-Mina, M. Effects of Anesthesia Technics on Certain Cytokines for Patients Undergoing Surgery: A Clinical Diagnostic Study. J. Coast. Life Med. 2023, 11, 383–394. [Google Scholar]
- Available online: https://www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-status-classification-system (accessed on 1 March 2024).
- Das, J.; Kumar, S.; Khanna, S.; Mehta, Y. Are we causing the recurrence-impact of perioperative period on long-term cancer prognosis: Review of current evidence and practice. J. Anaesthesiol. Clin. Pharmacol. 2014, 30, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Campos-Pérez, W.; Ramírez-Plascencia, L.; Pérez-Robles, M.; Rivera-Valdés, J.J.; Sánchez-Muñoz, P.; Pérez-Vargas, L.; González-Landeros, D.; Cuevas, J.H.M.; Martínez-López, E. A comparison of opioid-containing anesthesia versus opioid-free anesthesia using the Cortínez-Sepúlveda model on differential cytokine responses in obese patients undergoing gastric bypass surgery: A randomized controlled trial. BMC Anesthesiol. 2022, 22, 294. [Google Scholar] [CrossRef]
- Kany, S.; Vollrath, J.T.; Relja, B. Cytokines in Inflammatory Disease. Int. J. Mol. Sci. 2019, 20, 6008. [Google Scholar] [CrossRef]
- Lin, J.X.; Leonard, W.J. Fine-Tuning Cytokine Signals. Annu. Rev. Immunol. 2019, 37, 295–324. [Google Scholar] [CrossRef]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The Role of Tumor Necrosis Factor Alpha (TNF-α) in Autoimmune Disease and Current TNF-α Inhibitors in Therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef]
- Portmann, K.; Linder, A.; Oelgarth, N.; Eyer, K. Single-cell deep phenotyping of cytokine release unmasks stimulation-specific biological signatures and distinct secretion dynamics. Cell Rep. Methods 2023, 3, 100502. [Google Scholar] [CrossRef]
- Orosz, J.E.; Braz, M.G.; Golim, M.A.; Barreira, M.A.; Fecchio, D.; Braz, L.G.; Braz, J.R. Cytokine profile in patients undergoing minimally invasive surgery with balanced anesthesia. Inflammation 2012, 35, 1807–1813. [Google Scholar] [CrossRef] [PubMed]
- Ramani, T.; Auletta, C.S.; Weinstock, D.; Mounho-Zamora, B.; Ryan, P.C.; Salcedo, T.W.; Bannish, G. Cytokines: The Good, the Bad, and the Deadly. Int. J. Toxicol. 2015, 34, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, N.K.; Chadwick, A.L.; Nwaneshiudu, C.; Aggarwal, A.; Salmasi, V.; Lii, T.R.; Hah, J.M. Management of Postoperative Pain in Patients Following Spine Surgery: A Narrative Review. Int. J. Gen. Med. 2022, 15, 4535–4549. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Roychoudhury, P.; Lohia, S.; Kim, J.S.; Kim, H.T.; Ro, Y.J.; Koh, W.U. Comparison of General and Spinal Anaesthesia on Systemic Inflammatory Response in Patients Undergoing Total Knee Arthroplasty: A Propensity Score Matching Analysis. Medicina (Kaunas) 2021, 57, 1250. [Google Scholar] [CrossRef] [PubMed]
- Fekkes, D.; Hol, J.W.; Stolker, R.J. Anesthesia with propofol does not reduce interleukin-6 release in response to abdominal surgery of varying severity. J. Clin. Gynecol. Obstet. 2016, 5, 106–111. [Google Scholar] [CrossRef]
- Mohammed Ashrey, E.; Elwany Bosat, B. Impact of Two Different Anesthetic Techniques on Immune Response and Postoperative Pain for Abdominal Hysterectomy. Med. J. Cairo Univ. 2019, 87, 4363–4369. [Google Scholar] [CrossRef]
- Hassanshahi, G.; Hadavi, M.; Jafarzadeh, A.; Rezaeian, M.; Vazirinejad, R.; Sarkoohi, A.; Aminzadeh, F. Anesthesia technique and serum cytokine concentrations in the elective cesarean section. J. Res. Med. Sci. 2021, 26, 91. [Google Scholar] [CrossRef]
- Andreis, D.T.; Singer, M. Catecholamines for inflammatory shock: A Jekyll-and-Hyde conundrum. Intensive Care Med. 2016, 42, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Paravati, S.; Rosani, A.; Warrington, S.J. Physiology, Catecholamines. 2022. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Sharma, D.; Farrar, J.D. Adrenergic regulation of immune cell function and inflammation. Semin. Immunopathol. 2020, 42, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Cruz, F.F.; Rocco, P.R.; Pelosi, P. Anti-inflammatory properties of anesthetic agents. Crit. Care 2017, 21, 67. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, S.; Kato, M. Anesthetics, immune cells, and immune responses. J. Anesth. 2008, 22, 263–277. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Kaminga, A.C.; Wen, S.W.; Liu, A. Catecholamines in Post-traumatic Stress Disorder: A Systematic Review and Meta-Analysis. Front. Mol. Neurosci. 2018, 11, 450. [Google Scholar] [CrossRef] [PubMed]
- Taschner, A.; Kabon, B.; Falkner von Sonnenburg, M.; Graf, A.; Adamowitsch, N.; Fraunschiel, M.; Fleischmann, E.; Reiterer, C. Perioperative Supplemental Oxygen and Plasma Catecholamine Concentrations after Major Abdominal Surgery—Secondary Analysis of a Randomized Clinical Trial. J. Clin. Med. 2022, 11, 1767. [Google Scholar] [CrossRef] [PubMed]
- Fouladseresht, H.; Ghamar Talepoor, A.; Eskandari, N.; Norouzian, M.; Ghezelbash, B.; Beyranvand, M.R.; Nejadghaderi, S.A.; Carson-Chahhoud, K.; Kolahi, A.A.; Safiri, S. Potential Immune Indicators for Predicting the Prognosis of COVID-19 and Trauma: Similarities and Disparities. Front. Immunol. 2022, 12, 785946. [Google Scholar] [CrossRef] [PubMed]
- Restrepo-Serna, C.; Santamaría-Villegas, A. Association between stress and catecholamines with painful TMD in children. Int. J. Paediatr. Dent. 2024. [Google Scholar] [CrossRef] [PubMed]
- Corder, G.; Castro, D.C.; Bruchas, M.R.; Scherrer, G. Endogenous and exogenous opioids in pain. Annu. Rev. Neurosci. 2018, 41, 453–473. [Google Scholar] [CrossRef]
- Uribe-Rivera, A.; Rasubala, L.; Machado-Perez, A.; Ren, Y.; Malmström, H.; Carinci, A. Preliminary study of the impact of elevated circulating plasma levels of catecholamines on opioid requirements for acute surgical pain. J. Clin. Transl. Sci. 2021, 5, e114. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | GA Group (n = 15) | SA Group (n = 15) |
|---|---|---|
| Age (yrs) (mean ± SD) | 32.3 ± 4.82 | 31.2 ± 5.41 |
| BMI (Body Mass Index) (kg/m2) (mean ± SD) | 23.14 ± 3.45 | 21.68 ± 4.72 |
| Urban/rural areas | 8/7 | 7/8 |
| ASA (American Society of Anesthesiologists) grade I | 10 (66.67%) | 9 (60%) |
| ASA II | 5 (33.33%) | 6 (40%) |
| Gravidity | 2 ± 0.48 | 2 ± 0.83 |
| Parity | 2 ± 0.45 | 2 ± 0.48 |
| Gestational age at delivery (weeks) | 38.3 ± 0.62 | 38.5 ± 0.60 |
| Birth weight (g) | 3355 ± 165.19 | 3157 ± 207.10 |
| Apgar score at 1 min | 8 ± 0.63 | 9 ± 0.83 |
| Apgar score at 5 min | 9 ± 0.63 | 10 ± 0.45 |
| ICU (Intensive Care Unit) admission (n/%) | 3 (20%) | 2 (13.3%) |
| Preoperative hemoglobin (g/100 mL) | 12.2 ± 0.76 | 12.3 ± 0.45 |
| Postoperative hemoglobin (g/100 mL) | 10.8 ± 0.78 | 11.2 ± 0.44 |
| Preoperative hematocrit (%) | 34.2 ± 1.45 | 34.1 ± 1.20 |
| Postoperative hematocrit (%) | 30.1 ± 1.20 | 32.4 ± 0.73 |
| Surgical time (minutes) | 71.5 ± 10.70 | 52.7 ± 6.99 |
| Time to first mobilization (n/%) | ||
| 6 h | 2 (13.33%) | 4 (26.66%) |
| 6–12 h | 8 (53.33%) | 11 (73.33%) |
| 12–24 h | 5 (33.33%) | 0 |
| Postoperator complication | ||
| Nausea/vomiting | 2 (13.33%) | 1 (6.66%) |
| Headache | 0 | 3 (20%) |
| Cytokines (pg/mL) | Time | GA Group (n = 15) | SA Group (n = 15) | p-Value |
|---|---|---|---|---|
| TNF-α (Mean ± SD) | pre-OP | 7.11 ± 1.52 | 6.68 ± 2.05 | ns |
| 6 h post-OP | 12.00 ± 2.18 | 10.30 ± 1.08 | * | |
| 12 h post-OP | 17.50 ± 5.46 | 13.70 ± 2.21 | * | |
| IL-6 [Median (IR)] | pre-OP | 5.68 (4.98–6.21) | 3.33 (3.04–3.66) | ** |
| 6 h post-OP | 11.00 (9.21–13.00) | 6.89 (5.96–7.09) | ** | |
| 12 h post-OP | 15.40 (14.60–17.20) | 9.66 (8.74–10.20) | ** | |
| IL-8 (Mean ± SD) | pre-OP | 45.80 ± 14.15 | 43.60 ± 13.80 | ns |
| 6 h post-OP | 108.00 ± 33.00 | 62.70 ± 17.00 | ** | |
| 12 h post-OP | 162.00 ± 62.70 | 92.00 ± 27.70 | ** | |
| IL-4 (Mean ± SD) | pre-OP | 84.90 ± 11.80 | 73.80 ± 10.30 | ** |
| 6 h post-OP | 115.00 ± 16.00 | 99.70 ± 13.90 | ** | |
| 12 h post-OP | 143.00 ± 20.00 | 125.00 ± 17.40 | ** | |
| IL-10 [Median (IR)] | pre-OP | 4.14 (3.68–5.00) | 3.91 (3.76–4.54) | ns |
| 6 h post-OP | 5.62 (5.41–6.53) | 4.49 (4.33–5.22) | ** | |
| 12 h post-OP | 8.22 (7.91–9.55) | 5.67 (5.46–6.59) | ** |
| Catecholamines (Mean ± SD) | Time | GA Group (n = 15) | SA Group (n = 15) | p-Value |
|---|---|---|---|---|
| NE (ng/mL) | pre-OP | 4.85 ± 0.35 | 3.13 ± 0.23 | p < 0.0001 |
| 6 h post-OP | 6.40 ± 0.98 | 4.16 ± 0.42 | ||
| 12 h post-OP | 8.76 ± 1.13 | 5.33 ± 0.51 | ||
| EPI (pg/mL) | pre-OP | 498.00 ± 151.00 | 399.00 ± 121.00 | |
| 6 h post-OP | 598.00 ± 181.00 | 478.00 ± 145.00 | ||
| 12 h post-OP | 747.00 ± 226.00 | 598.00 ± 181.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novac, M.B.; Boldeanu, L.; Dijmărescu, A.L.; Boldeanu, M.V.; Neamțu, S.D.; Radu, L.; Manolea, M.M.; Șerbănescu, M.-S.; Stoica, M.; Rotaru, L.T.; et al. Immune Responses of Healthy Pregnant Women following an Elective Cesarean Section: Effects of Anesthetic Procedures. Diagnostics 2024, 14, 880. https://doi.org/10.3390/diagnostics14090880
Novac MB, Boldeanu L, Dijmărescu AL, Boldeanu MV, Neamțu SD, Radu L, Manolea MM, Șerbănescu M-S, Stoica M, Rotaru LT, et al. Immune Responses of Healthy Pregnant Women following an Elective Cesarean Section: Effects of Anesthetic Procedures. Diagnostics. 2024; 14(9):880. https://doi.org/10.3390/diagnostics14090880
Chicago/Turabian StyleNovac, Marius Bogdan, Lidia Boldeanu, Anda Lorena Dijmărescu, Mihail Virgil Boldeanu, Simona Daniela Neamțu, Lucreţiu Radu, Maria Magdalena Manolea, Mircea-Sebastian Șerbănescu, Maria Stoica, Luciana Teodora Rotaru, and et al. 2024. "Immune Responses of Healthy Pregnant Women following an Elective Cesarean Section: Effects of Anesthetic Procedures" Diagnostics 14, no. 9: 880. https://doi.org/10.3390/diagnostics14090880