
Comparison of Ultrasound Attenuation Imaging Using a Linear versus a Conventional Convex Probe: A Volunteer Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurement Protocol
2.2. Statistics
3. Results
3.1. Convex versus Linear Probe


3.2. Intraobserver Comparisons


Relative Intraobserver Variability
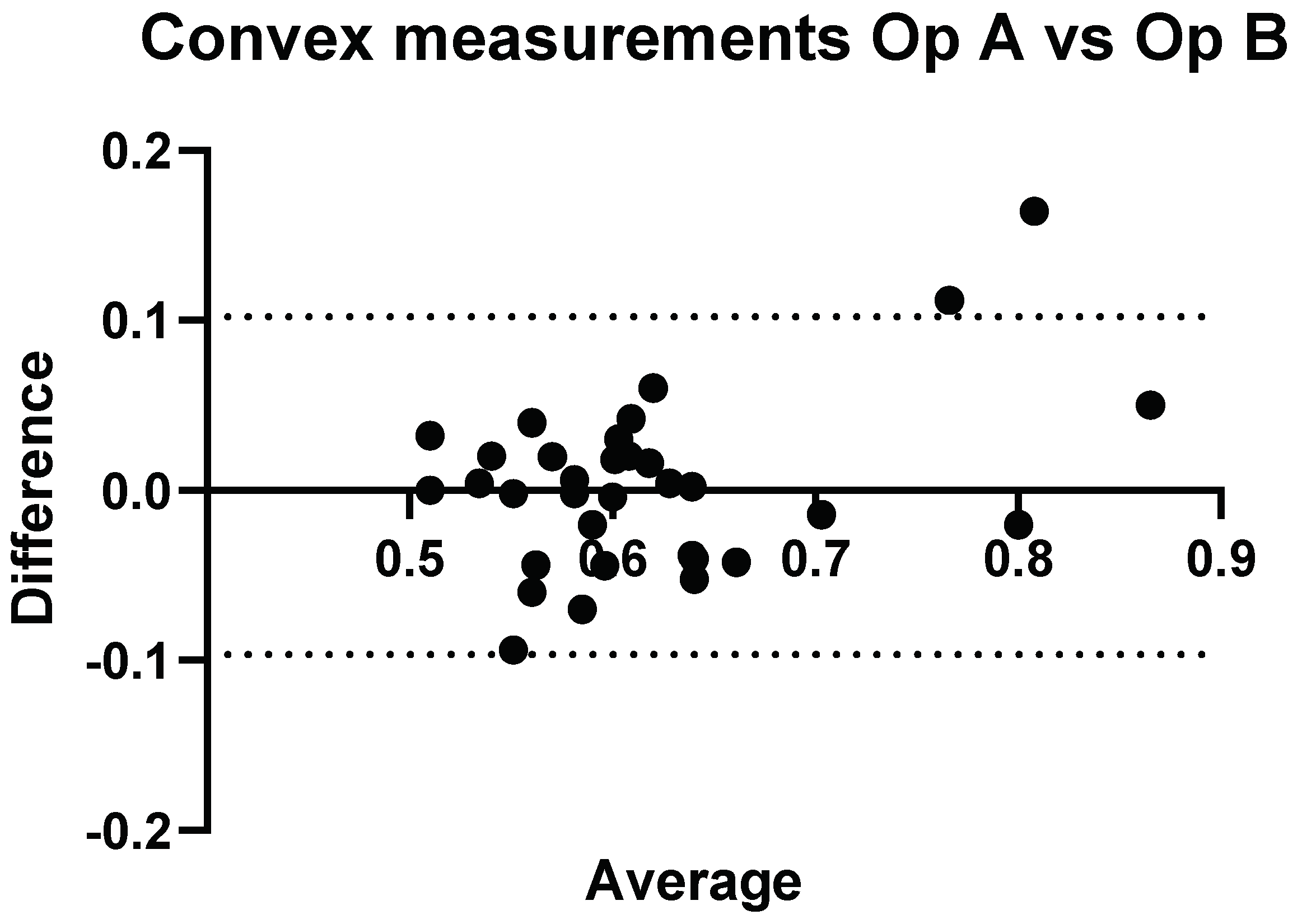
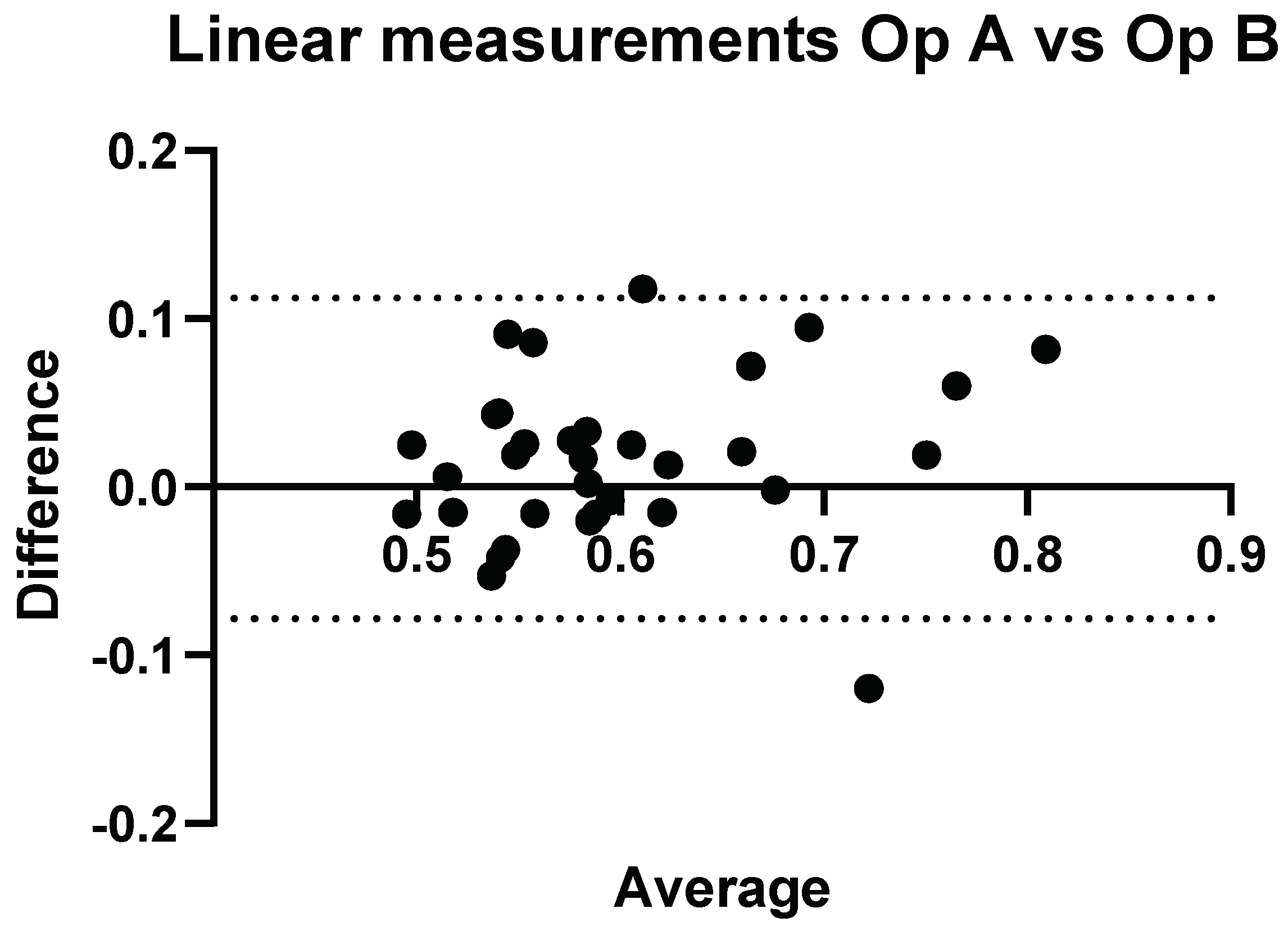
3.3. Interobserver Comparisons


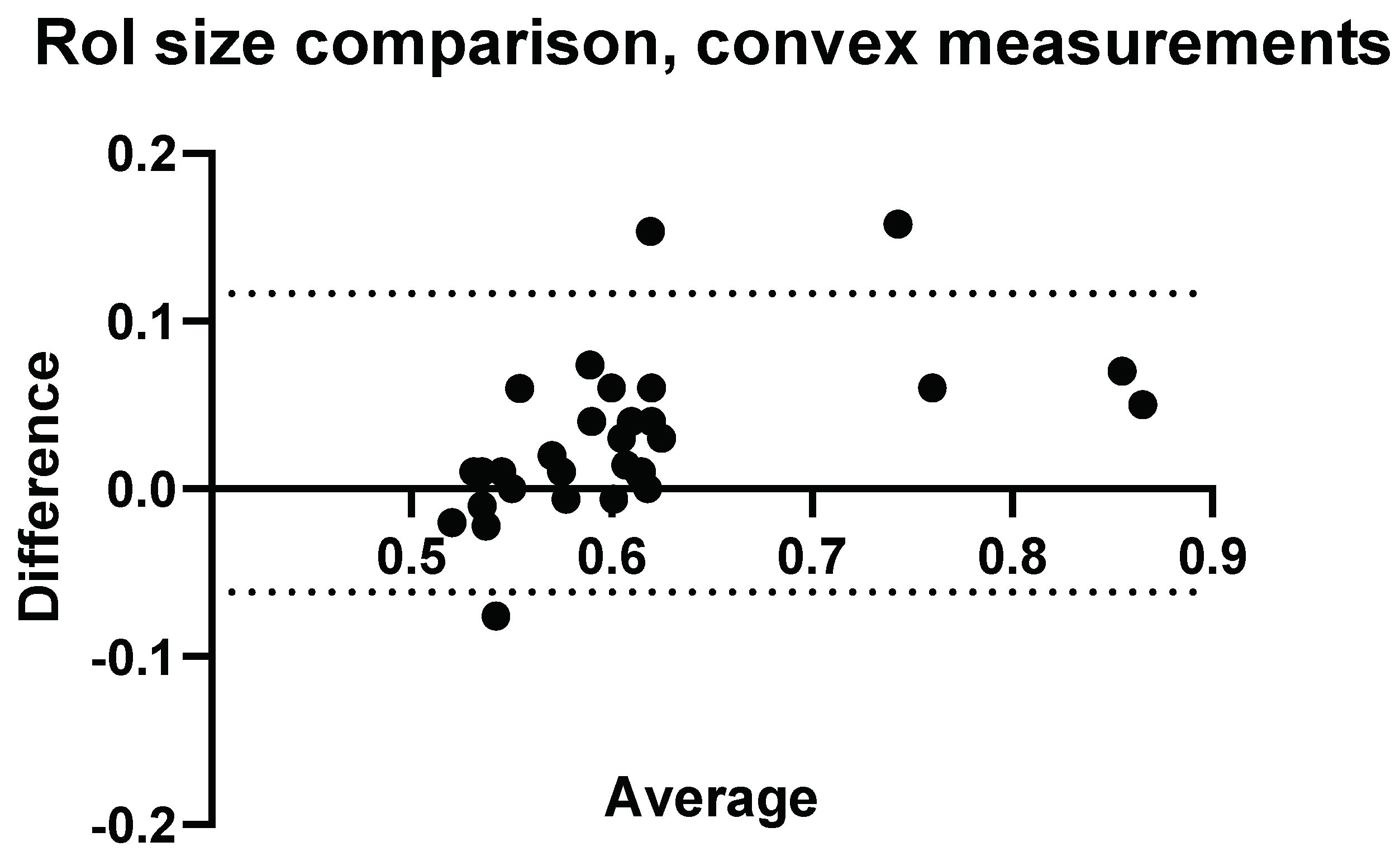
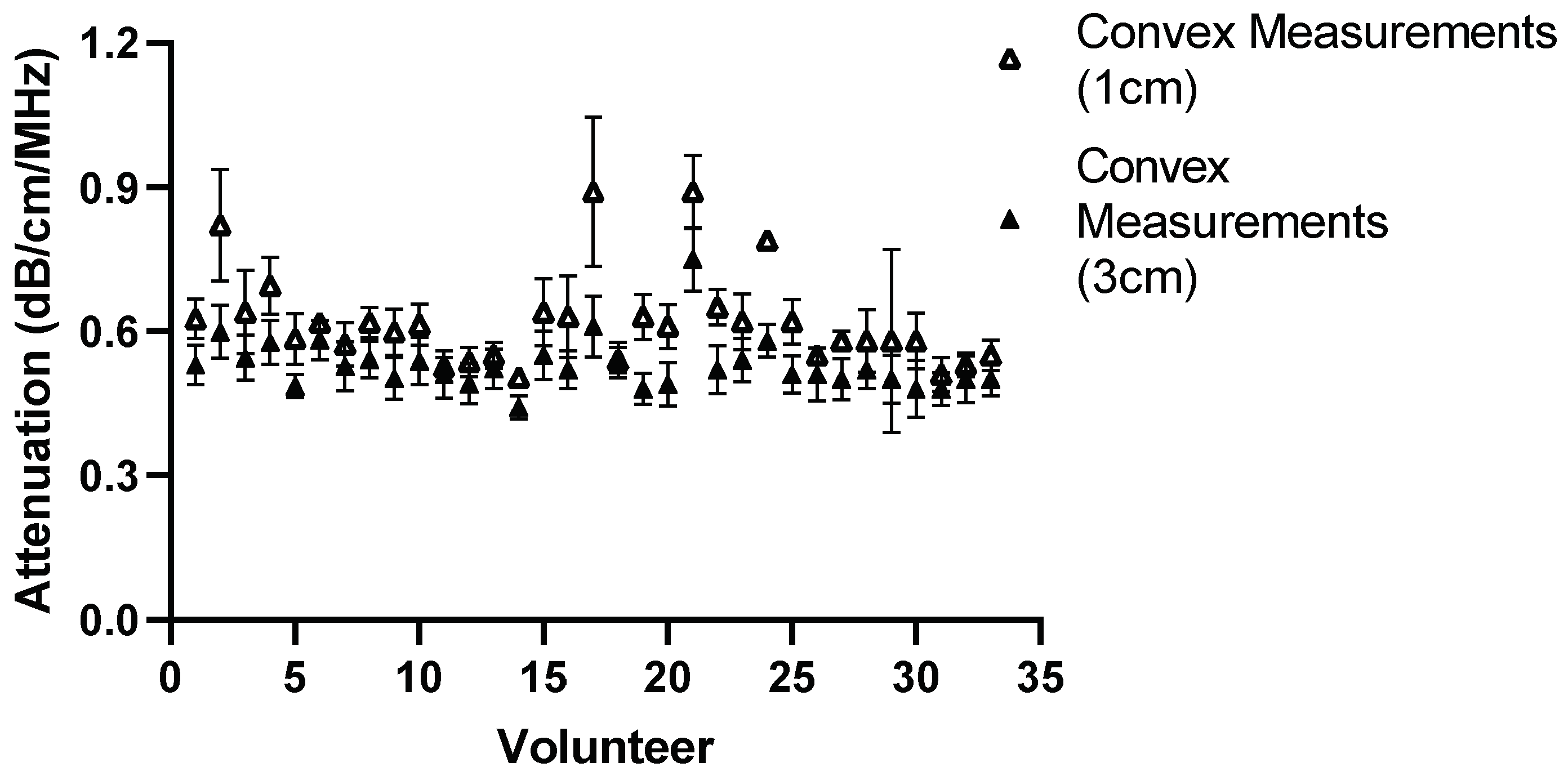
3.4. Confounders: ROI-Size and Insertion Depth








4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, K.C.; Liao, Y.Y.; Tsui, P.H.; Yeh, C.K. Ultrasound imaging in nonalcoholic liver disease: Current applications and future developments. Quant. Imaging Med. Surg. 2019, 9, 546–551. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31143646 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Bae, J.S.; Lee, D.H.; Lee, J.Y.; Kim, H.; Yu, S.J.; Lee, J.-H.; Cho, E.J.; Lee, Y.B.; Han, J.K.; Choi, B.I. Assessment of hepatic steatosis by using attenuation imaging: A quantitative, easy-to-perform ultrasound technique. Eur. Radiol. 2019, 29, 6499–6507. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31175413 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Ozturk, A.; Grajo, J.R.; Gee, M.S.; Benjamin, A.; Zubajlo, R.E.; Thomenius, K.E.; Anthony, B.W.; Samir, A.E.; Dhyani, M. Quantitative Hepatic Fat Quantification in Non-alcoholic Fatty Liver Disease Using Ultrasound-Based Techniques: A Review of Literature and Their Diagnostic Performance. Ultrasound Med. Biol. 2018, 44, 2461–2475. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30232020 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Liao, Y.Y.; Yang, K.C.; Lee, M.J.; Huang, K.C.; Chen, J.D.; Yeh, C.K. Multifeature analysis of an ultrasound quantitative diagnostic index for classifying nonalcoholic fatty liver disease. Sci. Rep. 2016, 6, 35083. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27734972 (accessed on 1 March 2024). [CrossRef]
- Hsu, P.K.; Wu, L.S.; Su, W.W.; Su, P.Y.; Chen, Y.Y.; Hsu, Y.C.; Yen, H.H.; Wu, C.L. Comparing the controlled attenuation parameter using FibroScan and attenuation imaging with ultrasound as a novel measurement for liver steatosis. PLoS ONE 2021, 16, e0254892. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34653177 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Nassir, F.; Rector, R.S.; Hammoud, G.M.; Ibdah, J.A. Pathogenesis and Prevention of Hepatic Steatosis. Gastroenterol. Hepatol. 2015, 11, 167. [Google Scholar]
- Mehta, S.R.; Thomas, E.L.; Bell, J.D.; Johnston, D.G.; Taylor-Robinson, S.D. Non-invasive means of measuring hepatic fat content. World J. Gastroenterol. 2008, 14, 3476–3483. Available online: https://pubmed.ncbi.nlm.nih.gov/18567074/ (accessed on 1 March 2024). [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. Available online: https://pubmed.ncbi.nlm.nih.gov/25920090/ (accessed on 1 March 2024). [CrossRef]
- Gatos, I.; Drazinos, P.; Yarmenitis, S.; Theotokas, I.; Koskinas, J.; Koullias, E.; Mitranou, A.; Manesis, E.; Zoumpoulis, P.S. Liver Ultrasound Attenuation: An Ultrasound Attenuation Index for Liver Steatosis Assessment. Ultrasound Q. 2022, 38, 124–132. Available online: https://pubmed.ncbi.nlm.nih.gov/35353797/ (accessed on 1 March 2024). [CrossRef]
- Alves, V.P.V.; Dillman, J.R.; Tkach, J.A.; Bennett, P.S.; Xanthakos, S.A.; Trout, A.T. Comparison of Quantitative Liver US and MRI in Patients with Liver Disease. Radiology 2022, 304, 660–669. Available online: https://pubmed.ncbi.nlm.nih.gov/35608446/ (accessed on 1 March 2024). [CrossRef]
- Ferraioli, G.; Maiocchi, L.; Savietto, G.; Tinelli, C.; Nichetti, M.; Rondanelli, M.; Calliada, F.; Preda, L.; Filice, C. Performance of the Attenuation Imaging Technology in the Detection of Liver Steatosis. J. Ultrasound Med. 2021, 40, 1325–1332. Available online: https://pubmed.ncbi.nlm.nih.gov/32960457/ (accessed on 1 March 2024). [CrossRef] [PubMed]
- Ferraioli, G.; Maiocchi, L.; Raciti, M.V.; Tinelli, C.; De Silvestri, A.; Nichetti, M.; De Cata, P.; Rondanelli, M.; Chiovato, L.; Calliada, F.; et al. Detection of Liver Steatosis with a Novel Ultrasound-Based Technique: A Pilot Study Using MRI-Derived Proton Density Fat Fraction as the Gold Standard. Clin. Transl. Gastroenterol. 2019, 10, e00081. [Google Scholar] [CrossRef] [PubMed Central]
- Jesper, D.; Klett, D.; Schellhaas, B.; Pfeifer, L.; Leppkes, M.; Waldner, M.; Neurath, M.F.; Strobel, D. Ultrasound-Based Attenuation Imaging for the Non-Invasive Quantification of Liver Fat—A Pilot Study on Feasibility and Inter-Observer Variability. IEEE J. Transl. Eng. Heal Med. 2020, 8, 1800409. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32617199 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Steyaert, L. Doppler sonography in breast pathology. JBR-BTR 2000, 83, 121–122. Available online: https://www.ncbi.nlm.nih.gov/pubmed/11025923 (accessed on 1 March 2024). [PubMed]
- Balius, R.; Pedret, C.; Iriarte, I.; Sáiz, R.; Cerezal, L. Sonographic landmarks in hamstring muscles. Skelet. Radiol. 2019, 48, 1675–1683. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30997529 (accessed on 1 March 2024). [CrossRef]
- Hegedüs, L. Thyroid ultrasound. Endocrinol. Metab. Clin. N. Am. 2001, 30, 339–360, viii–ix. Available online: https://www.ncbi.nlm.nih.gov/pubmed/11444166 (accessed on 1 March 2024). [CrossRef] [PubMed]
- Hänni, O.; Ruby, L.; Paverd, C.; Frauenfelder, T.; Rominger, M.B.; Martin, A. Confounders of Ultrasound Attenuation Imaging in a Linear Probe Using the Canon Aplio i800 System: A Phantom Study. Diagnostics 2024, 14, 271. [Google Scholar] [CrossRef] [PubMed]
- Sasso, M.; Beaugrand, M.; De Ledinghen, V.; Douvin, C.; Marcellin, P.; Poupon, R.; Sandrin, L.; Miette, V. Controlled attenuation parameter (CAP): A novel VCTETM guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: Preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med. Biol. 2010, 36, 1825–1835. Available online: https://www.ncbi.nlm.nih.gov/pubmed/20870345 (accessed on 1 March 2024). [CrossRef]
- Tada, T.; Iijima, H.; Kobayashi, N.; Yoshida, M.; Nishimura, T.; Kumada, T.; Kondo, R.; Yano, H.; Kage, M.; Nakano, C.; et al. Usefulness of Attenuation Imaging with an Ultrasound Scanner for the Evaluation of Hepatic Steatosis. Ultrasound Med. Biol. 2019, 45, 2679–2687. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31277922 (accessed on 1 March 2024). [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Ferraioli, G.; Raimondi, A.; Maiocchi, L.; De Silvestri, A.; Poma, G.; Kumar, V.; Barr, R.G. Liver Fat Quantification With Ultrasound: Depth Dependence of Attenuation Coefficient. J. Ultrasound Med. 2023, 42, 2247–2255. [Google Scholar] [CrossRef] [PubMed]
- Bruce, M.; Kolokythas, O.; Ferraioli, G.; Filice, C.; O’Donnell, M. Limitations and artifacts in shear-wave elastography of the liver. Biomed. Eng. Lett. 2017, 7, 81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rominger, M.B.; Kälin, P.; Mastalerz, M.; Martini, K.; Klingmüller, V.; Sanabria, S.; Frauenfelder, T. Influencing Factors of 2D Shear Wave Elastography of the Muscle—An Ex Vivo Animal Study. Ultrasound Int. Open 2018, 4, E54–E60. Available online: https://pubmed.ncbi.nlm.nih.gov/30250941/ (accessed on 1 March 2024). [CrossRef] [PubMed]
- Hwang, J.A.; Jeong, W.K.; Song, K.D.; Kang, K.A.; Lim, H.K. 2-D Shear Wave Elastography for Focal Lesions in Liver Phantoms: Effects of Background Stiffness, Depth and Size of Focal Lesions on Stiffness Measurement. Ultrasound Med. Biol. 2019, 45, 3261–3268. [Google Scholar] [CrossRef]
- Shin, H.J.; Kim, M.J.; Kim, H.Y.; Roh, Y.H.; Lee, M.J. Comparison of shear wave velocities on ultrasound elastography between different machines, transducers, and acquisition depths: A phantom study. Eur. Radiol. 2016, 26, 3361–3367. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, N.; Kaminuma, C.; Taketomi-Takahashi, A.; Tsushima, Y. Reliable measurement by virtual touch tissue quantification with acoustic radiation force impulse imaging: Phantom study. J. Ultrasound Med. 2012, 31, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.J.; Riely, C.A.; Hammers, L.; Flax, S.; Weltin, G.; Garcia-Tsao, G.; Conn, H.O.; Kuc, R.; Barwick, K.W. Quantitative US attenuation in normal liver and in patients with diffuse liver disease: Importance of fat. Radiology 1986, 160, 65–71. Available online: https://www.ncbi.nlm.nih.gov/pubmed/3520657 (accessed on 1 March 2024). [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (Range) | |
|---|---|
| Age (years) | 34.52 (24.5–63.3) |
| Sex | 19 (f)/14 (m) |
| Weight (kg) | 67.3 (52–86) |
| Height (m) | 1.72 (1.53–1.90) |
| BMI (kg/m2) | 22.6 (18.0–28.0) |
| Alcohol > 14 units/week | 3 yes/30 no |
| Volunteer | Convex Week 0 dB/cm/MHz | Convex Week 4 dB/cm/MHz | Relative Intraobserver Variability |
|---|---|---|---|
| 1 | 0.63 | 0.59 | 3.9% |
| 2 | 0.82 | 0.60 | 21.6% |
| 3 | 0.64 | 0.57 | 7.7% |
| 4 | 0.70 | 0.59 | 11.2% |
| 5 | 0.58 | 0.59 | 0.7% |
| 6 | 0.62 | 0.62 | 0.0% |
| 7 | 0.57 | 0.56 | 2.0% |
| 8 | 0.62 | 0.68 | 7.2% |
| 9 | 0.60 | 0.59 | 0.7% |
| 10 | 0.61 | 0.58 | 3.8% |
| 11 | 0.53 | 0.52 | 0.8% |
| 12 | 0.54 | 0.59 | 7.0% |
| 13 | 0.55 | 0.64 | 10.3% |
| 14 | 0.50 | 0.56 | 7.2% |
| 15 | 0.64 | 0.61 | 2.9% |
| 16 | 0.63 | 0.58 | 5.4% |
| 17 | 0.89 | 0.64 | 22.9% |
| 18 | 0.54 | 0.61 | 8.4% |
| 19 | 0.63 | 0.56 | 7.8% |
| 20 | 0.61 | 0.58 | 3.6% |
| 21 | 0.89 | 0.82 | 5.8% |
| 22 | 0.65 | 0.55 | 11.8% |
| 23 | 0.62 | 0.56 | 7.2% |
| 24 | 0.79 | 0.81 | 2.1% |
| 25 | 0.62 | 0.65 | 3.3% |
| 26 | 0.55 | 0.59 | 5.0% |
| 27 | 0.58 | 0.61 | 3.6% |
| 28 | 0.58 | 0.56 | 2.5% |
| 29 | 0.58 | 0.55 | 3.8% |
| 30 | 0.58 | 0.55 | 3.8% |
| 31 | 0.51 | 0.53 | 2.7% |
| 32 | 0.53 | 0.58 | 6.4% |
| 33 | 0.55 | 0.49 | 8.7% |
| Volunteer | Linear Week 0 dB/cm/MHz | Linear Week 4 dB/cm/MHz | Relative Intraobserver Variability |
|---|---|---|---|
| 1 | 0.49 | 0.57 | 11.6% |
| 2 | 0.62 | 0.71 | 9.7% |
| 3 | 0.59 | 0.55 | 5.6% |
| 4 | 0.66 | 0.64 | 2.2% |
| 5 | 0.53 | 0.58 | 6.9% |
| 6 | 0.58 | 0.59 | 1.8% |
| 7 | 0.56 | 0.51 | 6.3% |
| 8 | 0.61 | 0.60 | 1.3% |
| 9 | 0.68 | 0.66 | 1.5% |
| 10 | 0.59 | 0.55 | 4.5% |
| 11 | 0.52 | 0.56 | 5.1% |
| 12 | 0.57 | 0.49 | 10.3% |
| 13 | 0.56 | 0.58 | 2.7% |
| 14 | 0.80 | 0.71 | 8.3% |
| 15 | 0.70 | 0.69 | 1.5% |
| 16 | 0.51 | 0.57 | 8.3% |
| 17 | 0.76 | 0.82 | 5.0% |
| 18 | 0.56 | 0.51 | 6.6% |
| 19 | 0.63 | 0.61 | 1.9% |
| 20 | 0.60 | 0.57 | 3.3% |
| 21 | 0.85 | 0.91 | 4.9% |
| 22 | 0.60 | 0.56 | 4.9% |
| 23 | 0.58 | 0.61 | 3.7% |
| 24 | 0.74 | 0.72 | 1.5% |
| 25 | 0.67 | 0.71 | 4.4% |
| 26 | 0.55 | 0.58 | 4.2% |
| 27 | 0.59 | 0.59 | 0.4% |
| 28 | 0.59 | 0.58 | 1.3% |
| 29 | 0.67 | 0.54 | 15.8% |
| 30 | 0.52 | 0.50 | 2.5% |
| 31 | 0.51 | 0.49 | 2.7% |
| 32 | 0.51 | 0.55 | 5.6% |
| 33 | 0.59 | 0.53 | 7.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hänni, O.; Ruby, L.; Paverd, C.; Frauenfelder, T.; Rominger, M.B.; Martin, A. Comparison of Ultrasound Attenuation Imaging Using a Linear versus a Conventional Convex Probe: A Volunteer Study. Diagnostics 2024, 14, 886. https://doi.org/10.3390/diagnostics14090886
Hänni O, Ruby L, Paverd C, Frauenfelder T, Rominger MB, Martin A. Comparison of Ultrasound Attenuation Imaging Using a Linear versus a Conventional Convex Probe: A Volunteer Study. Diagnostics. 2024; 14(9):886. https://doi.org/10.3390/diagnostics14090886
Chicago/Turabian StyleHänni, Olivia, Lisa Ruby, Catherine Paverd, Thomas Frauenfelder, Marga B. Rominger, and Alexander Martin. 2024. "Comparison of Ultrasound Attenuation Imaging Using a Linear versus a Conventional Convex Probe: A Volunteer Study" Diagnostics 14, no. 9: 886. https://doi.org/10.3390/diagnostics14090886