

Clinical Implications of High-Sensitivity Troponin Elevation Levels in Non-ST-Segment Elevation Myocardial Infarction Patients: Beyond Diagnostics

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
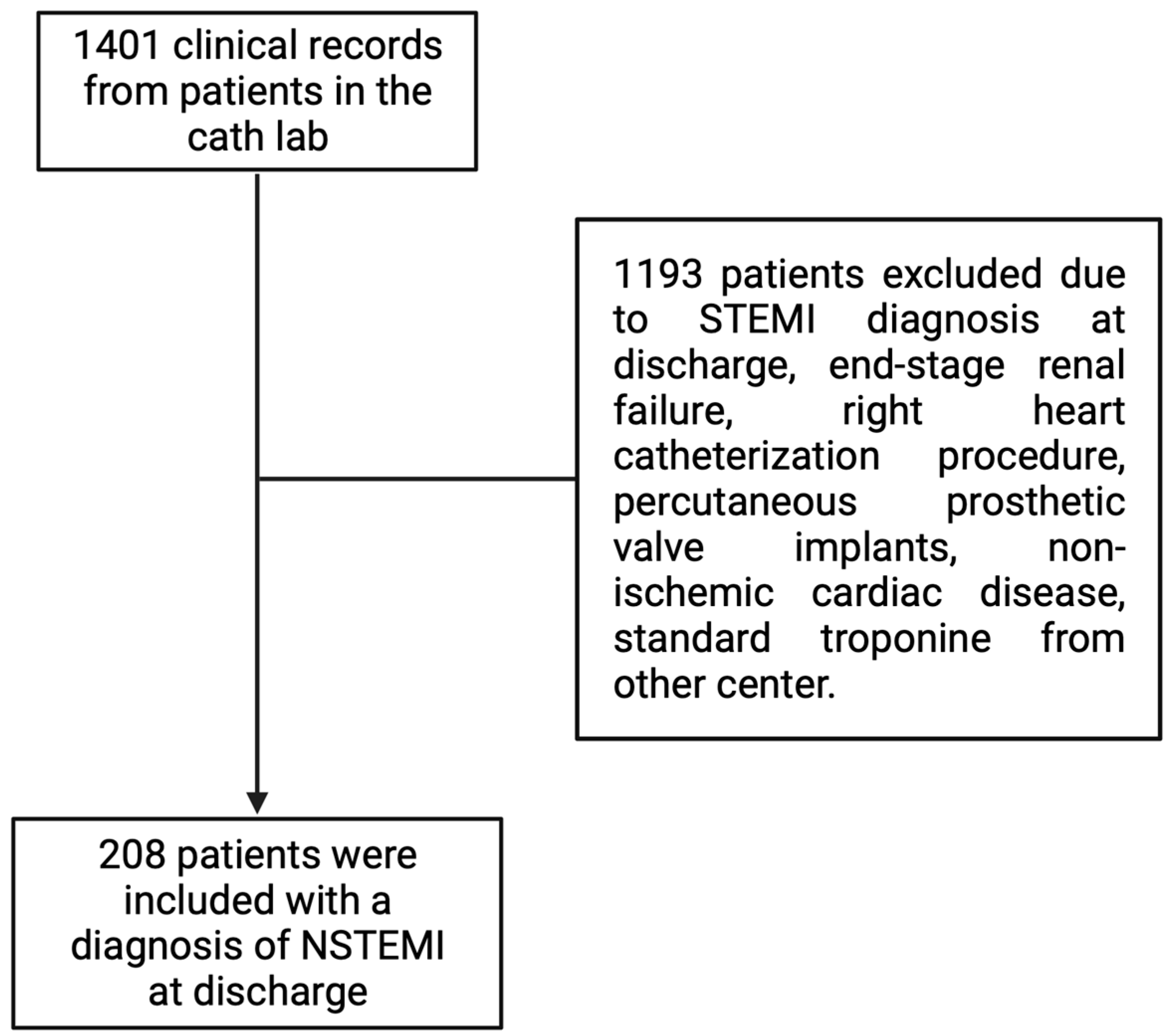
2.2. Inclusion and Exclusion Criteria
2.3. Statistical Analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Angiographic Severity of Coronary Lesion in the Culprit Artery
3.3. Validation of hs-cTnI for the Identification of Angiographically Severe Lesions
3.4. Localization of Culprit Artery Territory and Heart Failure at Admission
3.5. Performance of hs-cTnI and Characterization of Clinical Outcomes in the Obese Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garg, P.; Morris, P.; Fazlanie, A.L.; Vijayan, S.; Dancso, B.; Dastidar, A.G.; Plein, S.; Mueller, C.; Haaf, P. Cardiac biomarkers of acute coronary syndrome: From history to high-sensitivity cardiac troponin. Intern. Emerg. Med. 2017, 12, 147–155. [Google Scholar] [CrossRef]
- Arispe, I.N.S.R.; Sol, J.; Gil, A.C.; Trujillano, J.; Bravo, M.O.; Torres, O.Y. Comparison of heart, grace and TIMI scores to predict major adverse cardiac events from chest pain in a Spanish health care region. Sci. Rep. 2023, 13, 17280. [Google Scholar] [CrossRef]
- Kitamura, M.; Hata, N.; Takayama, T.; Hirayama, A.; Ogawa, M.; Yamashina, A.; Mera, H.; Yoshino, H.; Nakamura, F.; Seino, Y. Different characteristics of cardiac biomarkers to decide and predict the culprit lesions in patients with suspicious acute coronary syndrome. Heart Vessel. 2016, 31, 907–917. [Google Scholar] [CrossRef] [PubMed]
- López-Fernández, S.; Cequier, Á.; Iràculis, E.; Gómez-Hospital, J.A.; Teruel, L.; Valero, J.; Beltrán, P.; del Blanco, B.G.; Jara, F.; Esplugas, E. Elevated Troponin I Levels in Patients with Acute Coronary Syndrome Without ST Elevation Are Associated with Increased Complexity of the Culprit Lesion. Rev. Esp. Cardiol. 2004, 57, 291–298. [Google Scholar] [CrossRef]
- Damen, S.A.J.; Cramer, G.E.; Dieker, H.-J.; Gehlmann, H.; Ophuis, T.J.M.O.; Aengevaeren, W.R.M.; Fokkert, M.; Verheugt, F.W.A.; Suryapranata, H.; Wu, A.H.; et al. Cardiac Troponin Composition Characterization after Non ST-Elevation Myocardial Infarction: Relation with Culprit Artery, Ischemic Time Window, and Severity of Injury. Clin. Chem. 2021, 67, 227–236. [Google Scholar] [CrossRef]
- Benamer, H.; Steg, P.G.; Benessiano, J.; Vicaut, E.; Gaultier, C.J.; Aubry, P.; Boudvillain, O.; Sarfati, L.; Brochet, E.; Feldman, L.J.; et al. Elevated cardiac troponin I predicts a high-risk angiographic anatomy of the culprit lesion in unstable angina. Am. Heart J. 1999, 137, 815–820. [Google Scholar] [CrossRef]
- Hartman, M.H.T.; Eppinga, R.N.; Vlaar, P.J.J.; Lexis, C.P.H.; Lipsic, E.; Haeck, J.D.E.; van Veldhuisen, D.J.; van der Horst, I.C.C.; van der Harst, P. The contemporary value of peak creatine kinase-MB after ST-segment elevation myocardial infarction above other clinical and angiographic characteristics in predicting infarct size, left ventricular ejection fraction, and mortality. Clin. Cardiol. 2017, 40, 322–328. [Google Scholar] [CrossRef]
- Lazar, D.R.; Lazar, F.-L.; Homorodean, C.; Cainap, C.; Focsan, M.; Cainap, S.; Olinic, D.M. High-Sensitivity Troponin: A Review on Characteristics, Assessment, and Clinical Implications. Dis. Markers 2022, 2022, 9713326. [Google Scholar] [CrossRef]
- Sandoval, Y.; Apple, F.S.; Mahler, S.A.; Body, R.; Collinson, P.O.; Jaffe, A.S. High-Sensitivity Cardiac Troponin and the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guidelines for the Evaluation and Diagnosis of Acute Chest Pain. Circulation 2022, 146, 569–581. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Raber, I.; McCarthy, C.P.; Januzzi, J.L. A Test in Context: Interpretation of High-Sensitivity Cardiac Troponin Assays in Different Clinical Settings. J. Am. Coll. Cardiol. 2021, 77, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, M.; Padoan, A.; Mion, M.M.; Marinova, M.; Plebani, M. Short-term biological variation and diurnal rhythm of cardiac troponin I (Access hs-TnI) in healthy subjects. Clin. Chim. Acta 2020, 504, 163–167. [Google Scholar] [CrossRef]
- Parcha, V.; Patel, N.; Kalra, R.; Suri, S.S.; Arora, G.; Wang, T.J.; Arora, P. Obesity and serial nt-probnp levels in guided medical therapy for heart failure with reduced ejection fraction: Insights from the guide-it trial. J. Am. Heart Assoc. 2021, 10, e018689. [Google Scholar] [CrossRef]
- Baro, R.; Haseeb, S.; Ordoñez, S.; Costabel, J.P. High-sensitivity cardiac troponin T as a predictor of acute Total occlusion in patients with non-ST-segment elevation acute coronary syndrome. Clin. Cardiol. 2019, 42, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Aslanger, E.K.; Yıldırımtürk, Ö.; Şimşek, B.; Bozbeyoğlu, E.; Şimşek, M.A.; Karabay, C.Y.; Smith, S.W.; Değertekin, M. Diagnostic accuracy of electrocardiogram for acute coronary occlusion resulting in myocardial infarction (DIFOCCULT Study). IJC Heart Vasc. 2020, 30, 100603. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- High Sensitivity Troponin I Assay—VITROS®. Available online: https://www2.orthoclinicaldiagnostics.com/emea/diagnostics-library/solutions/high-sensitivity-troponin-assay (accessed on 20 June 2023).
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. Guía ESC 2020 sobre el diagnóstico y tratamiento del síndrome coronario agudo sin elevación del segmento ST. REC Interv. Cardiol. 2021, 74, 544.e1–544.e73. [Google Scholar] [CrossRef]
- Sanchis, J.; Alquézar-Arbé, A.; Ordóñez-Llanos, J.; Bardají, A. High-sensitivity Cardiac Troponin for the Evaluation of Patients with Suspected ACS: A True or a False Friend? Rev. Esp. Cardiol. 2019, 72, 445–448. [Google Scholar] [CrossRef]
- Tahhan, A.S.; Sandesara, P.; Hayek, S.S.; Hammadah, M.; Alkhoder, A.; Kelli, H.M.; Topel, M.; O’Neal, W.T.; Ghasemzadeh, N.; Ko, Y.; et al. High-sensitivity troponin I levels and coronary artery disease severity, progression, and long-term outcomes. J. Am. Heart Assoc. 2018, 7, e007914. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.L.; Bertazzo, B.B.; Grima, J.G.; Córdoba, A.V.F.; Konicoff, M.; Martina, L.; Rossa, V.; Amuchastegui, M.; Brenna, E.J.; Salomone, O.; et al. Validación de percentil 99 de troponina ultrasensible obtenido en la población de un hospital general. Archivos 2020, 77, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.D.; Hunter, A.; Madsen, D.M.; Shah, A.S.V.; McAllister, D.A.; Pawade, T.A.; Williams, M.C.; Berry, C.; Boon, N.A.; Flather, M.; et al. High-Sensitivity Cardiac Troponin I and the Diagnosis of Coronary Artery Disease in Patients with Suspected Angina Pectoris. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004227. [Google Scholar] [CrossRef]
- Wereski, R.; Adamson, P.; Daud, N.S.S.; McDermott, M.; Taggart, C.; Bularga, A.; Kimenai, D.M.; Lowry, M.T.; Tuck, C.; Anand, A.; et al. High-Sensitivity Cardiac Troponin for Risk Assessment in Patients with Chronic Coronary Artery Disease. J. Am. Coll. Cardiol. 2023, 82, 473–485. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Braun, S.; Schulz, S.; Mehilli, J.; Schömig, A.; Kastrati, A. High-sensitivity troponin T level and angiographic severity of coronary artery disease. Am. J. Cardiol. 2011, 108, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E.; Morrow, D.A. Unstable Angina. Circulation 2013, 127, 2452–2457. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Khanal, R.R.; Shah, S.; Gajurel, R.M.; Poudel, C.M.; Adhikari, S.; Yadav, V.; Devkota, S.; Thapa, S. Occluded Coronary Artery among Non-ST Elevation Myocardial Infarction Patients in Department of Cardiology of a Tertiary Care Centre: A Descriptive Cross-sectional Study. J. Nepal Med. Assoc. 2023, 61, 54–58. [Google Scholar] [CrossRef]
- Balbi, M.M.; Scarparo, P.; Tovar, M.N.; Masdjedi, K.; Daemen, J.; Dekker, W.D.; Ligthart, J.; Witberg, K.; Cummins, P.; Wilschut, J.; et al. Culprit Lesion Detection in Patients Presenting with Non-ST Elevation Acute Coronary Syndrome and Multivessel Disease. Cardiovasc. Revascularization Med. 2022, 35, 110–118. [Google Scholar] [CrossRef]
- Moustafa, A.; Abi-Saleh, B.; El-Baba, M.; Hamoui, O.; AlJaroudi, W. Anatomic distribution of culprit lesions in patients with non-ST-segment elevation myocardial infarction and normal ECG. Cardiovasc. Diagn. Ther. 2016, 6, 25–33. [Google Scholar] [CrossRef]
- Ekstroem, K.; Loenborg, J.; Nepper-Cristensen, L.; Holmvang, L.; Joshi, F.R.; Iversen, A.Z.; Madsen, P.L.; Olsen, N.T.; Pedersen, F.; Soerensen, R.; et al. Misclassification rate of the angiographically identified culprit lesion in NSTEMI. Eur. Heart J. 2022, 43, ehac544-1202. [Google Scholar] [CrossRef]
- Ekström, K.; Jensen, M.R.J.; Holmvang, L.; Joshi, F.R.; Iversen, A.Z.; Madsen, P.L.; Olsen, N.T.; Pedersen, F.; Sørensen, R.; Tilsted, H.-H.; et al. Organized thrombus is a frequent underlying feature in culprit lesion morphology in non-ST-elevation myocardial infarction. A study using optical coherence tomography and magnetic resonance imaging. Int. J. Cardiovasc. Imaging 2024, 40, 441–449. [Google Scholar] [CrossRef]
- Hung, C.-S.; Chen, Y.-H.; Huang, C.-C.; Lin, M.-S.; Yeh, C.-F.; Li, H.-Y.; Kao, H.-L. Prevalence and outcome of patients with non-ST segment elevation myocardial infarction with occluded “culprit” artery—A systemic review and meta-analysis. Crit. Care 2018, 22, 34. [Google Scholar] [CrossRef] [PubMed]
- Machline-Carrion, M.J.; Girotto, A.N.; Nieri, J.; Pereira, P.M.; Monfardini, F.; Forestiero, F.; Raupp, P.; Roveda, F.; Santo, K.; Berwanger, O.; et al. Assessing statins use in a real-world primary care digital strategy: A cross-sectional analysis of a population-wide digital health approach. Lancet Reg. Health Am. 2023, 23, 100534. [Google Scholar] [CrossRef]
- Tecson, K.M.; Kluger, A.Y.; Cassidy-Bushrow, A.E.; Liu, B.; Coleman, C.M.; Jones, L.K.; Jefferson, C.R.; VanWormer, J.J.; McCullough, P.A. Usefulness of Statins as Secondary Prevention Against Recurrent and Terminal Major Adverse Cardiovascular Events. Am. J. Cardiol. 2022, 176, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-F.; Lee, C.-K.; Wang, W.; Huang, Y.-C.; Lee, W.-J.; Wang, T.-D.; Chou, C.-Y. Coronary CT angiography-based estimation of myocardial perfusion territories for coronary artery FFR and wall shear stress simulation. Sci. Rep. 2021, 11, 13855. [Google Scholar] [CrossRef]
- Stelzle, D.; Shah, A.S.V.; Anand, A.; Strachan, F.E.; Chapman, A.R.; Denvir, M.A.; Mills, N.L.; McAllister, D.A. High-sensitivity cardiac troponin I and risk of heart failure in patients with suspected acute coronary syndrome: A cohort study. Eur. Heart J. Qual. Care Clin. Outcomes 2018, 4, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, A.; Amicone, S.; Armillotta, M.; Sansonetti, A.; Stefanizzi, A.; Angeli, F.; Fabrizio, M.; Bodega, F.; Canton, L.; Tattilo, F.P.; et al. Prognostic role and predictors of high Killip class in myocardial infarction with non-obstructive coronary artery. Eur. Heart J. 2022, 43, ehac544-1455. [Google Scholar] [CrossRef]
- Lyngbakken, M.N.; de Lemos, J.A.; Hveem, K.; Røsjø, H.; Omland, T. Lifetime obesity trends are associated with subclinical myocardial injury: The Trøndelag health study. J. Intern. Med. 2022, 291, 317–326. [Google Scholar] [CrossRef]
- Zhao, S.; Cao, R.; Zhang, S.; Kang, Y. Explore the Protective Role of Obesity in the Progression of Myocardial Infarction. Front. Cardiovasc. Med. 2021, 8, 629734. [Google Scholar] [CrossRef]
- Buettner, H.J.; Mueller, C.; Gick, M.; Ferenc, M.; Allgeier, J.; Comberg, T.; Werner, K.D.; Schindler, C.; Neumann, F.-J. The impact of obesity on mortality in UA/non-ST-segment elevation myocardial infarction. Eur. Heart J. 2007, 28, 1694–1701. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Patients at Baseline | |
|---|---|
| Demographic | |
| SD | 11.47 |
| Female—n (%) | 53 (25.48) |
| Comorbidities | |
| Hypertension—n (%) | 139 (66.83) |
| Diabetes—n (%) | 94 (45.19) |
| Smoking—n (%) | 68 (32.19) |
| Obesity—n (%) | 61 (29.33) |
| Coronary artery disease—n (%) | 68 (32.69) |
| Statins use—n (%) | 82 (39.42) |
| Laboratory | |
| SD [mL/min] | 8.39 |
| SD [mg/dL] | 0.5 |
| hs-TnI—median (IQR) [ng/L] | 122.75 (31.17–777.9) |
| Clinical | |
| Severe in angiography | |
| Positive—n (%) | 181 (87.02) |
| Killip-Kimbal classification | |
| Killip-Kimbal 1—n (%) | 171 (82.21) |
| Killip-Kimbal 2—n (%) | 21 (10.09) |
| Killip-Kimbal 3—n (%) | 14 (6.73) |
| Killip-Kimbal 4—n (%) | 2 (0.96) |
| Culprit coronary artery | |
| RCA—n (%) | 51 (25.25) |
| LAD—n (%) | 110 (54.46) |
| LCx—n (%) | 32 (15.84) |
| LMCA—n (%) | 9 (4.46) |
| Cut Off | Sensibility (%) | Specificity (%) | PPV (%) | NPV (%) | Precision (%) |
|---|---|---|---|---|---|
| 11 (ng/L) | 93.37% | 3.7% | 86.67% | 7.69% | 81.73% |
| 50 (ng/L) | 70.17% | 44.44% | 89.44% | 18.18% | 66.83% |
| Multivariate Analysis | ||||
|---|---|---|---|---|
| Variable | Coef. | IC 95% | p-Value | |
| Age | −44.52 | −97.948 | 8.908 | 0.102 |
| Gender | 508.62 | −717.683 | 1734.929 | 0.414 |
| Type 2 Diabetes Mellitus | 166.96 | −934.275 | 1268.203 | 0.765 |
| Arterial hypertension | 419.01 | −806.376 | 1644.399 | 0.501 |
| Smoking | 495.15 | −691.289 | 1681.598 | 0.412 |
| Obesity | 1638.36 | 438.994 | 2837.73 | 0.008 * |
| Estimated glomerular filtration rate | −9.71 | −73.096 | 53.672 | 0.763 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravo, C.; Vizcarra, G.; Sánchez, A.; Cárdenas, F.; Canales, J.P.; Ugalde, H.; Parra-Lucares, A. Clinical Implications of High-Sensitivity Troponin Elevation Levels in Non-ST-Segment Elevation Myocardial Infarction Patients: Beyond Diagnostics. Diagnostics 2024, 14, 893. https://doi.org/10.3390/diagnostics14090893
Bravo C, Vizcarra G, Sánchez A, Cárdenas F, Canales JP, Ugalde H, Parra-Lucares A. Clinical Implications of High-Sensitivity Troponin Elevation Levels in Non-ST-Segment Elevation Myocardial Infarction Patients: Beyond Diagnostics. Diagnostics. 2024; 14(9):893. https://doi.org/10.3390/diagnostics14090893
Chicago/Turabian StyleBravo, Constanza, Geovanna Vizcarra, Antonia Sánchez, Francisca Cárdenas, Juan Pablo Canales, Héctor Ugalde, and Alfredo Parra-Lucares. 2024. "Clinical Implications of High-Sensitivity Troponin Elevation Levels in Non-ST-Segment Elevation Myocardial Infarction Patients: Beyond Diagnostics" Diagnostics 14, no. 9: 893. https://doi.org/10.3390/diagnostics14090893