1. Introduction
In primary hyperparathyroidism (PHP), excessive secretion of parathyroid hormone (PTH) from one or more hyperactive parathyroid glands causes elevated levels of blood Ca2+. In approximately 90% of cases, PHP is caused by a single parathyroid adenoma. The preferred treatment is surgical removal of the diseased gland(s). As the location of the parathyroid adenoma is variable, preoperative imaging is often performed in order to permit a minimally-invasive surgical approach. Current imaging modalities include ultrasonography, parathyroid scintigraphy, contrast-enhanced CT, and magnetic resonance imaging. Recently, positron emission tomography/CT (PET/CT) using the 11C-labelled amino acid derivative [11C-l-methyl]-methionine (MET) and the 11C-labelled vitamin-like choline has shown promise. However, the availability of the 11C-based tracers is limited because the short half-life of 11C (20 min) requires an on-site cyclotron. In our department, we routinely use the 18F-based tracer O-2-(18F)fluoroethyl-l-tyrosine (FET)—another amino acid derivative—for brain glioma imaging. The 18F-based PET tracers are much easier to handle and distribute due to the longer half-life of 2 h, and they also provide better spatial resolution due to a shorter positron range, thus making them more appealing for diagnostic use. We considered it likely that FET would perform comparably to MET, as both are amino acid derivatives.
Therefore, we carried out a “proof-of-concept” study in two patients, aiming to verify or refute the feasibility of further evaluation of FET-PET in the preoperative workup in PHP.
2. Results
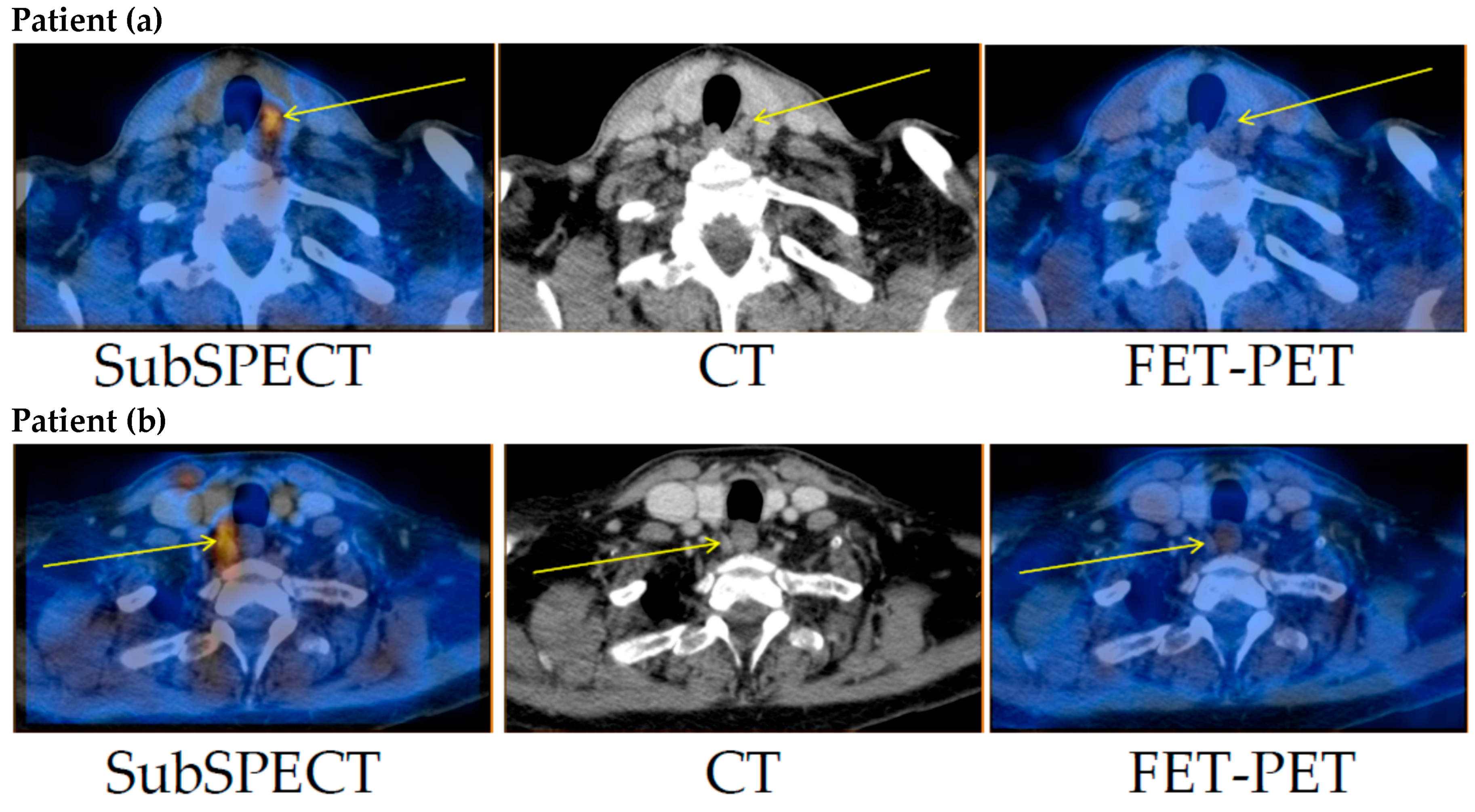
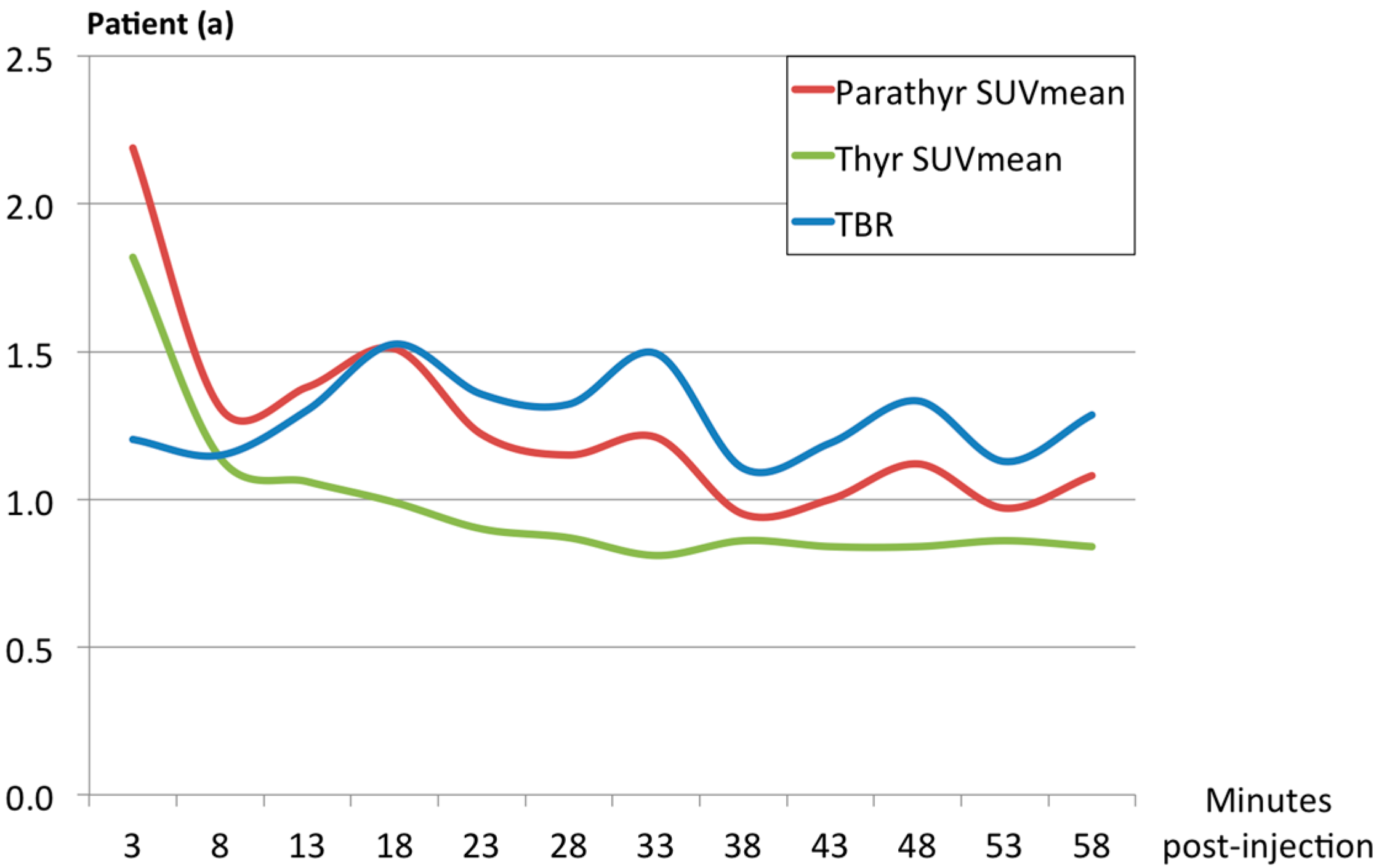
Only faint FET uptake was detected in both thyroid tissue and the parathyroid adenomas (
Figure 1). Excluding an obvious vascular phase during the first 10 min, TBR
max (for definition please refer to Materials and Methods) was reached between 30 and 35 min post-injection. TBR
max in patients (a) and (b) was 1.5 and 1.7, respectively. Thus, no clinically relevant differential uptake of FET could be detected in the parathyroid adenomas in either of the two patients (
Figure 2).
3. Discussion
This study was purely of an exploratory nature aiming to assess the differential uptake of FET in parathyroid adenomas versus thyroid tissue in vivo. We found no significant differential FET uptake in either of the two patients studied.
As MET (another amino acid-derived tracer) shows high uptake in parathyroid adenomas, we had hypothesised that this would also be the case for FET. However, the mechanisms of cellular amino acid uptake are complex, especially with regard to radiolabelled amino acid derivatives such as FET and MET. Transmembrane amino acid uptake is facilitated by an intricate system of specific transport proteins, all with different affinities for the individual amino acids. Two major subgroups are the Na
+-dependent and the Na
+-independent transport systems, the latter including the
l-type amino acid transporters (LAT1–4). The exact uptake mechanisms of FET and MET are not clear but it has been proposed that FET uptake primarily takes place via LAT2 [
1], while MET uptake is primarily mediated by LAT1 [
2]. Indeed, an antibody targeting the 4f2/SLC3A2 subunit of LAT1 has been shown to bind to and to affect parathyroid cells in culture [
3], demonstrating the presence of a functional LAT1 receptor in parathyroid tissue. Conversely, functional LAT2 cell surface expression in parathyroid cells has not been reported, to our knowledge. These findings are consistent with the fact that we found no significant uptake of FET as opposed to that reported on MET in most parathyroid adenomas [
4]. It could be argued that the two adenomas studied would also have been negative on MET. We cannot totally rule this out, as we did not perform MET-PET. However, since the sensitivity of MET-PET for surgically verified parathyroid adenomas has been found to be above 90%, we find it unlikely that both adenomas would have been negative on MET-PET.
4. Materials and Methods
This study was entirely exploratory. The primary aim was to study the in vivo uptake of FET in parathyroid adenomas.
The regional ethics committee for The Capital Region of Copenhagen approved the study (permission No. H-1-2011-101). After written and oral consent, patients were recruited from an ongoing study cohort evaluating various imaging modalities in PHP. As a tracer will only be appealing for clinical use if it provides increased sensitivity compared to the routinely used tracers, we tested the uptake of FET in two patients—(a) and (b)—with a positive sestamibi-single photon emission computed tomography/CT (SPECT/CT) performed with dual-isotope subtraction technique, which has a reported sensitivity of 93% [
5]. The location of the parathyroid adenomas was subsequently surgically and histologically confirmed. The parathyroid adenomas from patients (a) and (b) weighed 0.83 and 0.22 g, respectively. Preoperative plasma-PTH was 163 and 142 ng/L, respectively.
A dynamic PET/low dose-CT scan of the neck in a single bed-position was initiated immediately after the injection of 200 MBq FET (Philips Gemini TOF PET/CT). Acquisition continued for 60 min in list-mode, and counts were re-binned into 5–6 min bins. The exact position of the parathyroid adenoma was determined by co-registering the subtraction SPECT/CT with the FET PET/CT. A region-of-interest based target-to-background uptake value (TBR) was calculated as the mean standardize uptake value (SUVmean) in the parathyroid adenoma divided by SUVmean in the thyroid tissue in all bins. The bin with the highest TBR (TBRmax) was determined.
5. Conclusions
We found no significant differential FET uptake in parathyroid adenomas, possibly due to lack of expression of specific transmembrane transporter molecules in parathyroid tissue. 18F-FET seems therefore not to be a feasible tracer for use in preoperative localisation imaging in PHP.
Acknowledgments
No grants were received. Thanks are due to the technical staff in the department of Clinical Physiology and Nuclear Medicine, Gentofte Hospital for performing the PET and SPECT studies.
Author Contributions
Martin Krakauer and Finn N. Bennedbæk conceived and designed the study; Martin Krakauer performed the scans and analyzed the data; Andreas Kjær contributed the 18F-FET tracer; Finn N. Bennedbæk recruited the patients; Martin Krakauer wrote the paper; Finn N. Bennedbæk and Andreas Kjær contributed to the interpretation of the results and the preparation of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Langen, K.J.; Hamacher, K.; Weckesser, M.; Floeth, F.; Stoffels, G.; Bauer, D.; Coenen, H.H.; Pauleit, D. O-2-(18F)fluoroethyl-l-Tyrosine: uptake mechanisms and clinical applications. Nucl. Med. Biol. 2006, 33, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Okubo, S.; Zhen, H.N.; Kawai, N.; Nishiyama, Y.; Haba, R.; Tamiya, T. Correlation of l-methyl-11C-methionine (MET) uptake with l-type amino acid transporter 1 in human gliomas. J. Neurooncol. 2010, 99, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Posillico, J.T.; Srikanta, S.; Eisenbarth, G.; Quaranta, V.; Kajiji, S.; Brown, E.M. Binding of monoclonal antibody (4F2) to its cell surface antigen on dispersed adenomatous parathyroid cells raises cytosolic calcium and inhibits parathyroid hormone secretion. J. Clin. Endocrinol. Metab. 1987, 64, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Hayakawa, N.; Nakamoto, Y.; Kurihara, K.; Yasoda, A.; Kanamoto, N.; Miura, M.; Inagaki, N.; Togashi, K. A comparison between 11C-methionine PET/CT and MIBI SPECT/CT for localization of parathyroid adenomas/hyperplasia. Nucl. Med. Commun. 2015, 36, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, M.; Wieslander, B.; Myschetzky, P.S.; Lundstrom, A.; Bacher, T.; Sorensen, C.H.; Trolle, W.; Nygaard, B.; Bennedbaek, F.N. A prospective comparative study of parathyroid dual-phase scintigraphy, dual-isotope subtraction scintigraphy, 4D-CT, and ultrasonography in primary hyperparathyroidism. Clin. Nucl. Med. 2016, 41, 93–100. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}
{kind=link}


