
Value of SERCA2a as a Biomarker for the Identification of Patients with Heart Failure Requiring Circulatory Support

 , , ,
, , ,
Abstract
:1. Introduction and Objective
2. Material and Methods
2.1. Patients and Samples
2.2. Sample Processing
2.3. Specific Sandwich Enzyme-Linked Immunosorbent Assay
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients
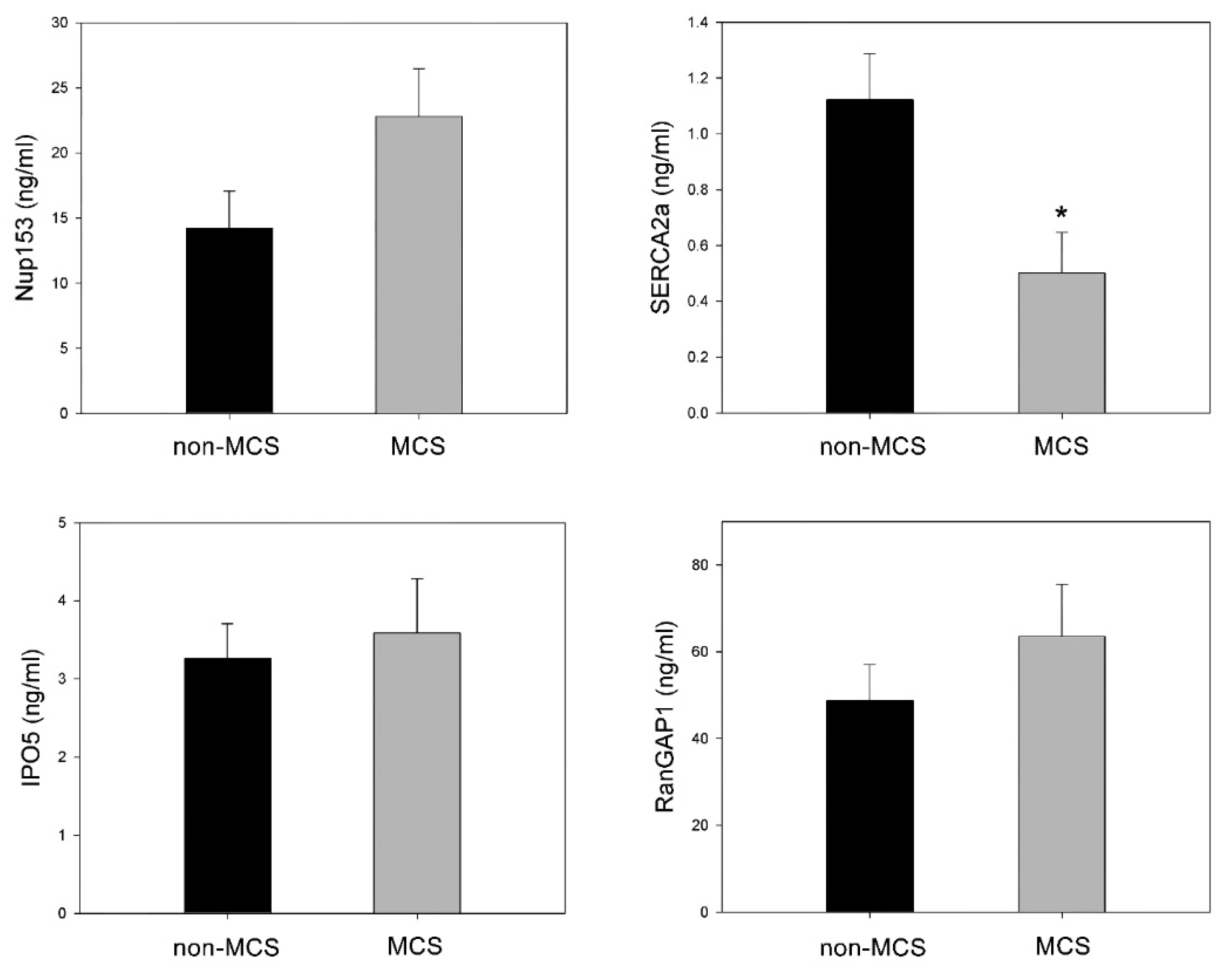
3.2. Plasma Levels of Molecules Involved in Intramyocardial Calcium Homeostasis and Nucleocytoplasmic Transport
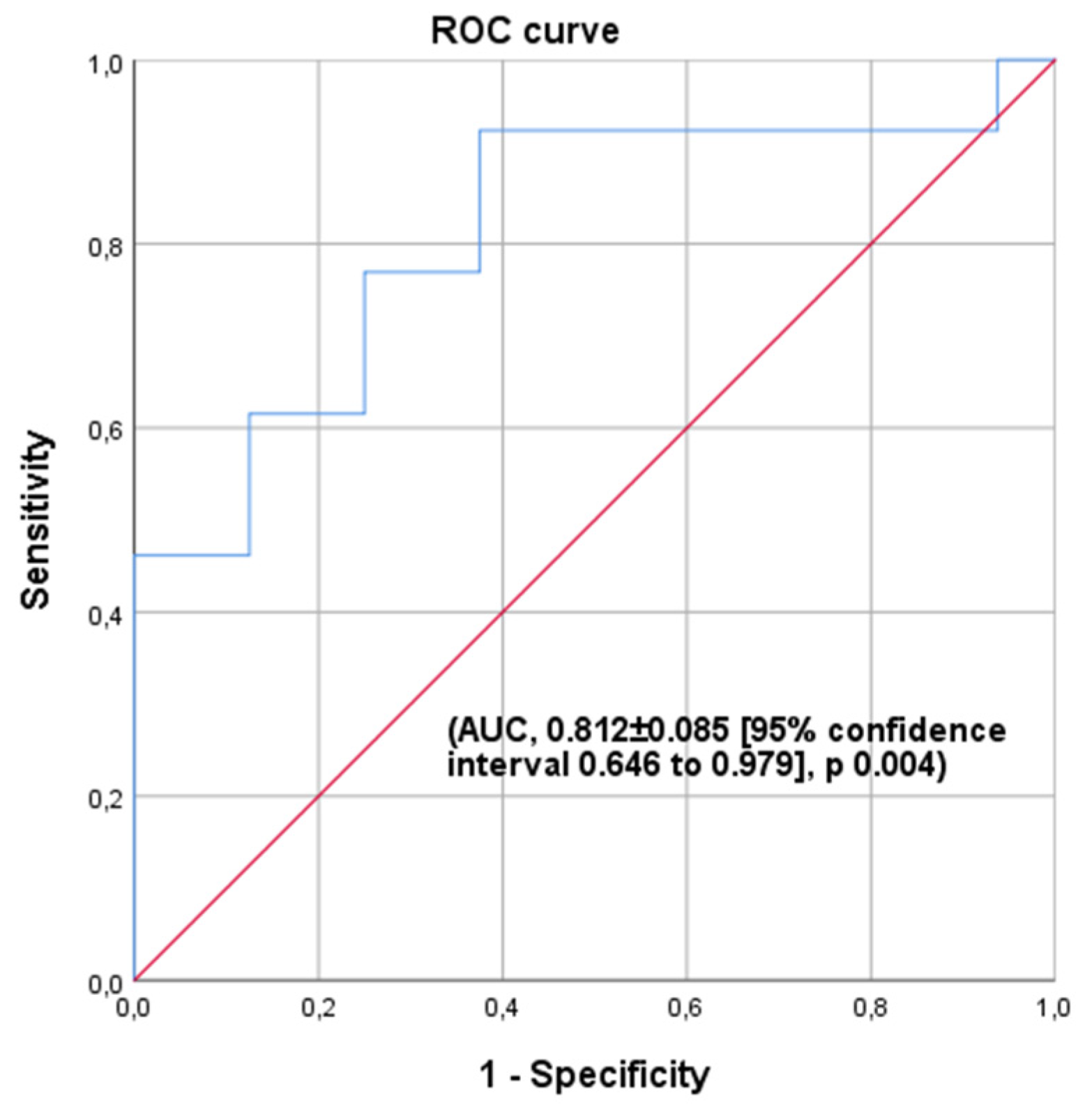
3.3. SERCA2a Capacity to Predict Advanced HF with an Unstable Clinical Outcome
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HT | Heart transplantation |
| HF | Heart Failure |
| MCS | Mechanical Circulatory Support |
| NPC | Nuclear pore complex |
| IMPs | Importins |
| EXPs | Exportins |
| SERCA2a | Sarcoplasmic reticulum Ca2+ ATPase |
| IPO5 | Importin5 |
| NUP153 | Nucleoporin153 kDa |
| RanGAP1 | RanGTPase-Activating Protein 1 |
| ECMO | Extracorporeal membrane oxygenator |
| ELISAs | Enzyme-linked immunosorbent assays |
| INTERMACS | Interagency Registry for Mechanically Assisted Circulatory Support |
References
- Salyer, J.; Flattery, M.P.; Joyner, P.L.; Elswick, R.K. Lifestyle and quality of life in long-term cardiac transplant recipients. J. Heart Lung Transplant. 2003, 22, 309–321. [Google Scholar] [CrossRef]
- Rosca, M.G.; Vazquez, E.J.; Kerner, J.; Parland, W.; Chandler, M.P.; Stanley, W.; Sabbah, H.N.; Hoppel, C.L. Cardiac mitochondria in heart failure: Decrease in respirasomes and oxidative phosphorylation. Cardiovasc. Res. 2008, 80, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Hein, S.; Kostin, S.; Heling, A.; Maeno, Y.; Schaper, J. The role of the cytoskeleton in heart failure. Cardiovasc. Res. 2000, 45, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Roselló-Lletí, E.; Rivera, M.; Cortés, R.; Azorín, I.; Sirera, R.; Martínez-Dolz, L.; Hove, L.; Cinca, J.; Lago, F.; González-Juanatey, J.R.; et al. Influence of heart failure on nucleolar organization and protein expression in human hearts. Biochem. Biophys. Res. Commun. 2012, 418, 222–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cieniewski-Bernard, C.; Mulder, P.; Henry, J.-P.; Drobecq, H.; Dubois-Deruy, E.; Pottiez, G.; Thuillez, C.; Amouyel, P.; Richard, V.; Pinet, F. Proteomic analysis of left ventricular remodelling in an experimental model of heart failure. J. Proteome Res. 2008, 7, 5004–5016. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, Y. Nucleocytoplasmic protein traffic and its significance to cell function. Genes Cells 2001, 5, 777–787. [Google Scholar] [CrossRef]
- Cook, A.; Bono, F.; Jinek, M.; Conti, E. Structural biology of nucleocytoplasmic transport. Annu. Rev. Biochem. 2007, 76, 647–671. [Google Scholar] [CrossRef]
- Perez-Terzic, C.; Gacy, A.M.; Bortolon, R.; Dzeja, P.P.; Puceat, M.; Jaconi, M.; Prendergast, F.G.; Terzic, A. Structural plasticity of the cardiac nuclear pore complex in response to regulators of nuclear import. Circ. Res. 1999, 84, 1292–1301. [Google Scholar] [CrossRef] [Green Version]
- Lidsky, P.V.; Hato, S.; Bardina, M.V.; Aminev, A.G.; Palmenberg, A.C.; Sheval, E.V.; Polyakov, V.Y.; van Kuppeveld, F.J.M.; Agol, V.I. Nucleocytoplasmic traffic disorder induced by cardioviruses. J. Virol. 2006, 80, 2705–2717. [Google Scholar] [CrossRef] [Green Version]
- Cortés, R.; Roselló-Lletí, E.; Rivera, M.; Martínez-Dolz, L.; Salvador, A.; Azorín, I.; Portolés, M. Influence of heart failure on nucleocytoplasmic transport in human cardiomyocytes. Cardiovasc. Res. 2010, 85, 464–472. [Google Scholar] [CrossRef] [Green Version]
- Tarazón, E.; Rivera, M.; Roselló-Lletí, E.; Molina-Navarro, M.M.; Sánchez-Lázaro, I.J.; España, F.; Montero, J.A.; Lago, F.; Juanatey, J.R.G.; Portolés, M. Heart failure induces significant changes in nuclear pore complex of human cardiomyocytes. PLoS ONE 2012, 7, e48957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Navarro, M.M.; Roselló-Lletí, E.; Tarazón, E.; Ortega, A.; Sánchez-Izquierdo, D.; Lago, F.; González-Juanatey, J.R.; García-Pavía, P.; Salvador, A.; Montero, J.A.; et al. Heart failure entails significant changes in human nucleocytoplasmic transport gene expression. Int. J. Cardiol. 2013, 168, 2837–2843. [Google Scholar] [CrossRef] [PubMed]
- Bers, D.M. Calcium cycling and signaling in cardiac myocytes. Annu. Rev. Physiol. 2008, 70, 23–49. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.M.; Inesi, G. Silencing calcineurin A subunit reduces SERCA2 expression in cardiac myocytes. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H173–H180. [Google Scholar] [CrossRef] [Green Version]
- Del Monte, F.; Harding, S.E.; Schmidt, U.; Matsui, T.; Kang, Z.B.; Dec, G.W.; Gwathmey, J.K.; Rosenzweig, A.; Hajjar, R.J. Restoration of contractile function in isolated cardiomyocytes from failing human hearts by gene transfer of SERCA2a. Circulation 1999, 100, 2308–2311. [Google Scholar] [CrossRef] [Green Version]
- Flesch, M.; Schwinger, R.H.; Schiffer, F.; Frank, K.; Südkamp, M.; Kuhn-Regnier, F.; Arnold, G.; Bo¨hm, M. Evidence for functional relevance of an enhanced expression of the Na+-Ca2+ exchanger in failing human myocardium. Circulation 1996, 94, 992–1002. [Google Scholar] [CrossRef]
- Tarazón, E.; Gil-Cayuela, C.; Manzanares, M.G.; Roca, M.; Lago, F.; Juanatey, J.R.G.; Sánchez-Lacuesta, E.; Martinez-Dolz, L.; Portolés, M.; Roselló-Lletí, E. Circulating Sphingosine-1-Phosphate as A Non-Invasive Biomarker of Heart Transplant Rejection. Sci. Rep. 2019, 9, 13880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarazón, E.; Ortega, A.; Gil-Cayuela, C.; Sánchez-Lacuesta, E.; Marín, P.; Lago, F.; González-Juanatey, J.R.; Martínez-Dolz, L.; Portolés, M.; Rivera, M.; et al. SERCA2a: A potential non-invasive biomarker of cardiac allograft rejection. J. Heart Lung Transplant. 2017, 36, 1322–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jessup, M.; Greenberg, B.; Mancini, D.; Cappola, T.; Pauly, D.F.; Jaski, B.; Yaroshinsky, A.; Zsebo, K.M.; Dittrich, H.; Hajjar, R.J. Calcium Upregulation by Percutaneous Administration of Gene Therapy in Cardiac Disease (CUPID): A Phase II trial of intracoronary gene therapy of sarcoplasmic reticulum Ca2+-ATPase in patients with advanced heart failure. Circulation 2011, 124, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, B.; Butler, J.; Felker, G.M.; Ponikowski, P.; Voors, A.A.; Desai, A.S.; Barnard, D.; Bouchard, A.; Jaski, B.; Lyon, A.R.; et al. Calcium up regulation by Percutaneous administration of gene therapy in patients with cardiac disease (CUPID2): A randomised, multinational, double-blind, placebo-controlled, phase IIb trial. Lancet 2016, 387, 1178–1186. [Google Scholar] [CrossRef]
- Macrae, D.J. The Council for International Organizations and Medical Sciences (CIOMS) guidelines on ethics of clinical trials. Proc. Am. Thorac. Soc. 2007, 4, 176–178. [Google Scholar] [CrossRef] [Green Version]
- González-Vílchez, F.; Almenar-Bonet, L.; Crespo-Leiro, M.G.; Segovia-Cubero, J.; González-Costello, J.; Del Prado, J.M.A.; Sousa-Casasnovas, I.; Sobrino-Márquez, J.M.; Delgado-Jiménez, J.; Pérez-Villa, F. Spanish Heart Transplant Registry: 30th official report of the Spanish Society of Cardiology Working Group on Heart Failure (1984–2018). Rev. Esp. Cardiol. 2019, 72, 954–962. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D., Jr.; Hsich, E.; Meiser, B.; Potena, L.; Robinson, A.; Rossano, J.W.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult heart transplantation report—2019; focus theme: Donor and recipient size match. J. Heart Lung Transplant. 2019, 38, 1056–1066. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.G.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Stevenson, L.W.; Pagani, F.; Young, J.B.; Jessup, M.; Miller, L.; Kormos, R.L.; Naftel, D.C.; Ulisney, K.; Desvigne-Nickens, P.; Kirklin, J.K. INTERMACS profiles of advanced heart failure: The current picture. J. Heart Lung Transplant. 2009, 28, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Barge-Caballero, E.; Segovia-Cubero, J.; Almenar-Bonet, L.; Gonzalez-Vilchez, F.; Villa-Arranz, A.; Delgado-Jimenez, J.; Lage-Galle, E.; Perez-Villa, F.; Lambert-Rodríguez, J.L.; Manito-Lorite, N.; et al. Preoperative INTERMACS Profiles Determine Postoperative Outcomes in Critically Ill Patients Undergoing Emergency Heart Transplantation Analysis of the Spanish National Heart Transplant Registry. Circ. Heart Fail. 2013, 6, 763. [Google Scholar] [CrossRef] [Green Version]
- Mercadier, J.J.; Lompré, A.M.; Duc, P.; Boheler, K.R.; Fraysse, J.B.; Wisnewsky, C.; Allen, P.D.; Komajda, M.; Schwartz, K. Altered sarcoplasmic reticulum Ca2(þ)-ATPase gene expression in the human ventricle during end-stage heart failure. J. Clin. Investig. 1990, 85, 305–309. [Google Scholar] [CrossRef] [Green Version]
- Eisner, D.; Caldwell, J.; Trafford, A. Sarcoplasmic reticulum Ca-ATPase and heart failure 20 years later. Circ. Res. 2013, 113, 958–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stüdeli, R.; Jung, S.; Mohacsi, P.; Perruchoud, S.; Castiglioni, P.; Wenaweser, P.; Heimbeck, G.; Feller, M.; Hullin, R. Diastolic dysfunction in human cardiac allografts is related with reduced SERCA2a gene expression. Am. J. Transplant. 2006, 6, 775–782. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| MCS (n = 13) | Non-MCS (n = 16) | p | |
|---|---|---|---|
| Age (years) | 52 ± 10 | 50 ± 14 | 0.60 |
| AF (%) | 54 | 50 | 1.00 |
| BMI (Kg/m2) | 26.4 ± 4 | 26.4 ± 3 | 0.90 |
| CO (L/min) | 3.3 ± 0.4 | 3.6 ± 0.8 | 0.40 |
| COPD (%) | 8 | 0 | 0.40 |
| CRT (%) | 15 | 31 | 0.40 |
| DM (%) | 15 | 12 | 1.00 |
| eGFR (ml/min/1.73 m2) | 93 ± 33 | 70 ± 24 | 0.06 |
| Gender (% Men) | 85 | 81 | 1.00 |
| HBP (%) | 23 | 37 | 0.40 |
| ICD (%) | 77 | 94 | 0.30 |
| ICM (%) | 54 | 37 | 0.50 |
| Inotropes (%) | 92% | 25% | 0.00 |
| INTERMACS (%) | I–II: 15.4 | III: 18.8 | 0.00 |
| II–III: 84.6 | IV–V: 81.3 | ||
| LVEF (%) | 20 ± 7 | 27 ± 18 | 0.20 |
| mPAP (mmHg) | 41 ± 12 | 34 ± 10 | 0.10 |
| MV (%) | 23 | 0 | 0.08 |
| PCWP (mmHg) | 28 ± 10 | 24 ± 8 | 0.40 |
| PHT (%) | 90 | 81 | 0.90 |
| Pr.CVS (%) | 8 | 12 | 0.90 |
| Pr.Infection (%) | 31 | 12 | 0.40 |
| Pr.VascD (%) | 15 | 12 | 1.00 |
| PVR (UW) | 3.7 ± 2.4 | 2.8 ± 1.1 | 0.20 |
| RI (%) | 31 | 25 | 0.90 |
| Smoking (Yes/Ex) (%) | 8/54 | 12/37 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ezzitouny, M.; Roselló-Lletí, E.; Portolés, M.; Sánchez-Lázaro, I.; Arnau-Vives, M.Á.; Tarazón, E.; Gil-Cayuela, C.; Lozano-Edo, S.; López-Vilella, R.; Almenar-Bonet, L.; et al. Value of SERCA2a as a Biomarker for the Identification of Patients with Heart Failure Requiring Circulatory Support. J. Pers. Med. 2021, 11, 1122. https://doi.org/10.3390/jpm11111122
Ezzitouny M, Roselló-Lletí E, Portolés M, Sánchez-Lázaro I, Arnau-Vives MÁ, Tarazón E, Gil-Cayuela C, Lozano-Edo S, López-Vilella R, Almenar-Bonet L, et al. Value of SERCA2a as a Biomarker for the Identification of Patients with Heart Failure Requiring Circulatory Support. Journal of Personalized Medicine. 2021; 11(11):1122. https://doi.org/10.3390/jpm11111122
Chicago/Turabian StyleEzzitouny, Meryem, Esther Roselló-Lletí, Manuel Portolés, Ignacio Sánchez-Lázaro, Miguel Ángel Arnau-Vives, Estefanía Tarazón, Carolina Gil-Cayuela, Silvia Lozano-Edo, Raquel López-Vilella, Luis Almenar-Bonet, and et al. 2021. "Value of SERCA2a as a Biomarker for the Identification of Patients with Heart Failure Requiring Circulatory Support" Journal of Personalized Medicine 11, no. 11: 1122. https://doi.org/10.3390/jpm11111122