Fluid Responsiveness Is Associated with Successful Weaning after Liver Transplant Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Bioreactance Monitoring
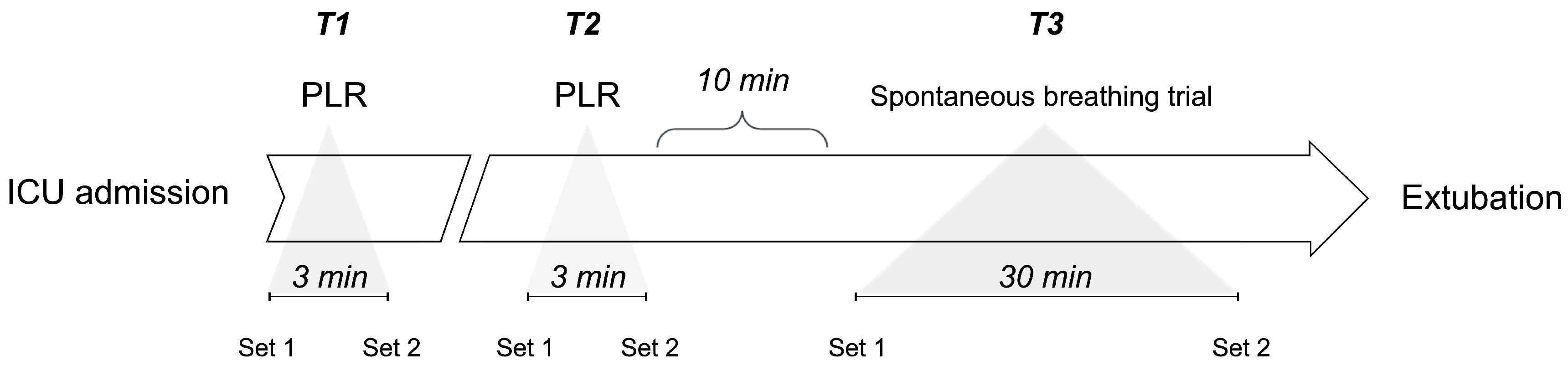
2.3. Study Procedures
2.3.1. Hemodynamic Monitoring
2.3.2. Spontaneous Breathing Trial
2.3.3. Passive Leg Raising
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silversides, J.A.; Fitzgerald, E.; Manickavasagam, U.; Lapinsky, S.E.; Nisenbaum, R.; Hemmings, N.; Nutt, C.; Trinder, T.J.; Pogson, D.; Fan, E.; et al. Deresuscitation of Patients with Iatrogenic Fluid Overload Is Associated with Reduced Mortality in Critical Illness*. Crit. Care Med. 2018, 46, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-J.; Pai, K.-C.; Huang, C.-T.; Wong, L.-T.; Wang, M.-S.; Lai, C.-M.; Chen, C.-H.; Wu, C.-L.; Chao, W.-C. A Positive Fluid Balance in the First Week Was Associated with Increased Long-Term Mortality in Critically Ill Patients: A Retrospective Cohort Study. Front. Med. 2022, 9, 727103. [Google Scholar] [CrossRef] [PubMed]
- Messmer, A.S.; Zingg, C.; Mûller, M.; Gerber, J.; Schefold, J.C.; Pfortmueller, C.A. Fluid Overload and Mortality in Adult Critical Care Patients—A Systematic Review and Meta-Analysis of Observational Studies*. Crit. Care Med. 2020, 48, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Cordemans, C.; De Laet, I.; Regenmortel, N.V.; Schoonheydt, K.; Dits, H.; Martin, G.; Huber, W.; Malbrain, M.L. Aiming for a Negative Fluid Balance in Patients with Acute Lung Injury and Increased Intra-Abdominal Pressure: A Pilot Study Looking at the Effects of PAL-Treatment. Ann. Intensive Care 2012, 2, S15. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.N.G.; Marik, P.E.; Witters, I.; Cordemans, C.; Kirkpatrick, A.W.; Roberts, D.J.; Regenmortel, N.V. Fluid Overload, de-Resuscitation, and Outcomes in Critically Ill or Injured Patients: A Systematic Review with Suggestions for Clinical Practice. Anaesthesiol. Intensive Ther. 2014, 46, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Kattan, E.; Castro, R.; Miralles-Aguiar, F.; Hernández, G.; Rola, P. The Emerging Concept of Fluid Tolerance: A Position Paper. J. Crit. Care 2022, 71, 154070. [Google Scholar] [CrossRef] [PubMed]
- Pfortmueller, C.A.; Dabrowski, W.; Malbrain, M.L.N.G. Fluid De-Resuscitation in Critical Illness—A Journey into Uncertain Territory. J. Crit. Care 2023, 76, 154249. [Google Scholar] [CrossRef] [PubMed]
- Cruz, D.N.; Ricci, Z.; Bagshaw, S.M.; Piccinni, P.; Gibney, N.; Ronco, C. Renal Replacement Therapy in Adult Critically Ill Patients: When to Begin and When to Stop. Contrib. Nephrol. 2010, 165, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Villa, G.; Katz, N.; Ronco, C. Extracorporeal Membrane Oxygenation and the Kidney. Cardiorenal Med. 2015, 6, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Granado, R.C.-D.; Mehta, R.L. Fluid Overload in the ICU: Evaluation and Management. BMC Nephrol. 2016, 17, 109. [Google Scholar] [CrossRef]
- Zeuthen, E.; Wichmann, S.; Schønemann-Lund, M.; Järvisalo, M.J.; Wahlin, R.R.; Sigurðsson, M.I.; Holen, E.; Bestle, M.H. Nordic Survey on Assessment and Treatment of Fluid Overload in Intensive Care. Front. Med. 2022, 9, 1067162. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Ronco, C.; Kazory, A. Diagnosis of Fluid Overload: From Conventional to Contemporary Concepts. Cardiorenal Med. 2022, 12, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Rienzo, M.; Osman, D.; Anguel, N.; Richard, C.; Pinsky, M.R.; Teboul, J. Passive Leg Raising Predicts Fluid Responsiveness in the Critically Ill*. Crit. Care Med. 2006, 34, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Marik, P.; Teboul, J.-L. Passive Leg Raising for Predicting Fluid Responsiveness: A Systematic Review and Meta-Analysis. Intensive Care Med. 2016, 42, 1935–1947. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Marik, P.E.; Teboul, J.-L. Prediction of Fluid Responsiveness: An Update. Ann. Intensive Care 2016, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Cipriani, F.; Camous, L.; Sentenac, P.; Dres, M.; Krastinova, E.; Anguel, N.; Richard, C.; Teboul, J.-L. The Passive Leg Raising Test to Guide Fluid Removal in Critically Ill Patients. Ann. Intensive Care 2016, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Shen, F.; Teboul, J.; Anguel, N.; Beurton, A.; Bezaz, N.; Richard, C.; Monnet, X. Cardiac Dysfunction Induced by Weaning from Mechanical Ventilation: Incidence, Risk Factors, and Effects of Fluid Removal. Crit. Care 2016, 20, 369. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Teboul, J.-L.; Anguel, N.; Guerin, L.; Richard, C.; Monnet, X. Passive Leg Raising Performed before a Spontaneous Breathing Trial Predicts Weaning-Induced Cardiac Dysfunction. Intensive Care Med. 2015, 41, 487–494. [Google Scholar] [CrossRef]
- Lemaire, F.; Teboul, J.-L.; Cinotti, L.; Giotto, G.; Abrouk, S.F.; Steg, G.; Macquin-Mavier, I.; Zapol, W.M. Acute Left Ventricular Dysfunction during Unsuccessful Weaning from Mechanical Ventilation. Anesthesiology 1988, 69, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, M.R. Breathing as Exercise: The Cardiovascular Response to Weaning from Mechanical Ventilation. Intensive Care Med. 2000, 26, 1164–1166. [Google Scholar] [CrossRef] [PubMed]
- Ferré, A.; Guillot, M.; Lichtenstein, D.; Mezière, G.; Richard, C.; Teboul, J.-L.; Monnet, X. Lung Ultrasound Allows the Diagnosis of Weaning-Induced Pulmonary Oedema. Intensive Care Med. 2019, 45, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Kashani, A.; Landaverde, C.; Medici, V.; Rossaro, L. Fluid Retention in Cirrhosis: Pathophysiology and Management. QJM Int. J. Med. 2008, 101, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Carrier, F.M.; Chassé, M.; Wang, H.T.; Aslanian, P.; Bilodeau, M.; Turgeon, A.F. Effects of Perioperative Fluid Management on Postoperative Outcomes in Liver Transplantation: A Systematic Review Protocol. Syst. Rev. 2018, 7, 180. [Google Scholar] [CrossRef] [PubMed]
- Avolio, A.W.; Gaspari, R.; Teofili, L.; Bianco, G.; Spinazzola, G.; Soave, P.M.; Paiano, G.; Francesconi, A.G.; Arcangeli, A.; Nicolotti, N.; et al. Postoperative Respiratory Failure in Liver Transplantation: Risk Factors and Effect on Prognosis. PLoS ONE 2019, 14, e0211678. [Google Scholar] [CrossRef] [PubMed]
- Suphathamwit, A.; Pongraweewan, O.; Lakkam, S.; Tovikkai, C. Predictive Score for Immediate Extubation after Liver Transplantation. Clin. Transplant. 2021, 35, e14212. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Huttin, O.; Rossignol, P.; Girerd, N. The Unit of Estimated Plasma Volume in Patients with Heart Failure Using the Strauss-Derived Duarte Formula Is Not Liter but DL/g. J. Card. Fail. 2019, 25, 140. [Google Scholar] [CrossRef] [PubMed]
- Duarte, K.; Monnez, J.M.; Albuisson, É.; Pitt, B.; Zannad, F.; Rossignol, P. Prognostic Value of Estimated Plasma Volume in Heart Failure. JACC Hear. Fail. 2015, 3, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Hakim, R.M. Plasmapheresis, 3rd ed.; Daugirdas, J.T., Blake, P.G., Ing, T.S., Eds.; Lippincott, Williams and Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Kim, K.H.; Cho, H.J.; Kim, S.C.; Lee, J. Prognostic Value of Estimated Plasma Volume Status in Patients with Sepsis. J. Korean Med. Sci. 2022, 37, e145. [Google Scholar] [CrossRef] [PubMed]
- Ahlgrim, C.; Birkner, P.; Seiler, F.; Grundmann, S.; Bode, C.; Pottgiesser, T. Estimated Plasma Volume Status Is a Modest Predictor of True Plasma Volume Excess in Compensated Chronic Heart Failure Patients. Sci. Rep. 2021, 11, 24235. [Google Scholar] [CrossRef] [PubMed]
- Keren, H.; Burkhoff, D.; Squara, P. Evaluation of a Noninvasive Continuous Cardiac Output Monitoring System Based on Thoracic Bioreactance. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H583–H589. [Google Scholar] [CrossRef] [PubMed]
- Douglas, I.S.; Alapat, P.M.; Corl, K.A.; Exline, M.C.; Forni, L.G.; Holder, A.L.; Kaufman, D.A.; Khan, A.; Levy, M.M.; Martin, G.S.; et al. Fluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical Trial. Chest 2020, 158, 1431–1445. [Google Scholar] [CrossRef] [PubMed]
- Kattan, E.; Ospina-Tascón, G.A.; Teboul, J.-L.; Castro, R.; Cecconi, M.; Ferri, G.; Bakker, J.; Hernández, G.; Hernandez, G.; Ospina-Tascón, G.; et al. Systematic Assessment of Fluid Responsiveness during Early Septic Shock Resuscitation: Secondary Analysis of the ANDROMEDA-SHOCK Trial. Crit. Care 2020, 24, 23. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Shi, R.; Teboul, J.-L. Prediction of Fluid Responsiveness. What’s New? Ann. Intensive Care 2022, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Butti, F.; Pache, B.; Winiker, M.; Grass, F.; Demartines, N.; Hübner, M. Correlation of Postoperative Fluid Balance and Weight and Their Impact on Outcomes. Langenbeck’s Arch. Surg. 2020, 405, 1191–1200. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Demographics | n = 15 |
| Age (years) | 62 {54, 65} |
| Sex (female) | 53% |
| Height (cm) | 165 {158, 173} |
| Weight (kg) | 74 {56, 75} |
| Body mass index | 25 {21, 26} |
| Clinical condition at admission | |
| APACHE II | 14 {10, 18} |
| MELD | 21 {14, 23} |
| SOFA | 6 {6, 10} |
| Norepinephrine (mcg/kg/min) (6 pts) | 0.004 {0.000, 0.220} |
| Fluid balance (m/L) | 4480 {3697, 5723} |
| Laboratory | |
| Lactate (mmol/L) | 3.2 {1.7, 5.1} |
| Hemoglobin (g/dL) | 9.7 {8.6, 10.5} |
| Albumin (g/dL) | 3.4 {2.7, 4.2} |
| Na (mEq/L) | 142 {138, 143} |
| K (mEq/L) | 4.3 {3.9, 4.4} |
| BUN (mg/dL) | 20 {13, 26} |
| Creatinine (mg/dL) | 0.9 {0.7, 1.2} |
| (a) | ||||||||||||||
| FLUID-RESPONSIVE | ||||||||||||||
| HR (lpm) | p | SAP (mmHg) | p | DAP (mmHg) | p | MAP (mmHg) | p | RR (bpm) | p | SaO2 (%) | p | pCO2 (mmHg) | p | |
| PLR start (T1) | 77 {70, 85} | 0.971 | 115 {108, 123} | 0.436 | 47 {47, 60} | 0.075 | 94 {90, 99} | 0.280 | 20 {17, 21} | 0.218 | 100 {99, 100} | 0.232 | ||
| PLR end (T1) | 77 {72, 85} | 120 {105, 152} | 65 {52, 72} | 103 {90, 128} | 20 {15, 21} | 98 {96, 100} | ||||||||
| PLR start (T2) | 79 {69, 88} | 0.887 | 112 {104, 123} | 0.551 | 55 {47, 65} | 0.054 | 92 {85, 104} | 0.514 | 22 {18, 22} | 0.143 | 100 {98, 100} | 0.912 | ||
| PLR end (T2) | 78 {67, 85} | 115 {108, 130} | 68 {57, 70} | 100 {84, 115} | 18 {16, 21} | 99 {96, 100} | ||||||||
| SBT start (T3) | 80 {69, 90} | 0.932 | 114 {104, 132} | 0.908 | 52 {49, 67} | 0.219 | 73 {68, 85} | 0.319 | 20 {19, 22} | 0.198 | 98 {96, 100} | 0.413 | 41 {37, 45} | 0.195 |
| SBT end (T3) | 75 {70, 91} | 116 {103, 130} | 62 {53, 70} | 78 {73, 88} | 18 {14, 21} | 97 {96, 98} | 37 {33, 39} | |||||||
| FLUID-UNRESPONSIVE | ||||||||||||||
| HR (lpm) | p | SAP (mmHg) | p | DAP (mmHg) | p | MAP (mmHg) | p | RR (bpm) | p | SaO2 (%) | p | pCO2 (mmHg) | p | |
| PLR start (T1) | 71 {67, 77} | 0.527 | 119 {104, 142} | 0.189 | 64 {59, 66} | 0.206 | 99 {85, 116} | 0.401 | 21 {18, 22} | 0.244 | 99 {98, 100} | 0.279 | ||
| PLR end (T1) | 73 {61, 78} | 136 {114, 151} | 68 {64, 73} | 111 {94, 127} | 16 {13, 19} | 98 {96, 99} | ||||||||
| PLR start (T2) | 76 {72, 76} | 0.268 | 120 {115, 132} | 0.050 | 62 {61, 67} | 0.127 | 105 {99, 116} | 0.127 | 16 {14, 19} | 0.658 | 100 {98, 100} | 0.609 | ||
| PLR end (T2) | 74 {67, 75} | 150 {149, 158} | 81 {74, 82} | 128 {127, 137} | 18 {17, 20} | 99 {94, 100} | ||||||||
| SBT start (T3) | 70 {67, 73} | 0.827 | 123 {119, 146} | 0.275 | 59 {57, 67} | 0.121 | 80 {80, 93} | 0.184 | 16 {14, 19} | 0.513 | 97 {96, 98} | 0.822 | 39 {38, 43} | 0.202 |
| SBT end (T3) | 71 {66, 74} | 149 {148, 165} | 77 {75, 77} | 106 {105, 112} | 15 {11, 18} | 97 {97, 98} | 37 {33, 39} | |||||||
| (b) | ||||||||||||||
| FLUID-RESPONSIVE | ||||||||||||||
| CI (L/min/m2) | p | SVI (mL/m2) | p | SVV (%) | p | CVP (mmHg) | p | SvO2 (%) | p | TFC (1/Ω) | p | |||
| PLR start (T1) | 2.8 {2.7, 3.0} | 0.003 | 37 {33, 43} | 0.005 | 21 {15, 22} | 0.035 | 9 {8, 10} | 0.529 | 74 {73, 74} | 0.971 | 110 {78, 120} | 0.912 | ||
| PLR end (T1) | 4.0 {3.6, 4.7} | 55 {49, 55} | 13 {13, 16} | 9 {8, 10} | 73 {68, 75} | 113 {75, 116} | ||||||||
| PLR start (T2) | 3.1 {2.8, 3.6} | 0.005 | 40 {38, 44} | 0.001 | 16 {14, 21} | 0.039 | 9 {8, 10} | 0.681 | 74 {70, 75} | 0.876 | 94 {72, 115} | 0.059 | ||
| PLR end (T2) | 3.9 {3.6, 4.7} | 53 {45, 55} | 13 {13, 15} | 9 {7, 9} | 71 {70, 73} | 99 {75, 113} | ||||||||
| SBT start (T3) | 3.1 {2.8, 3.7} | 0.045 | 42 {32, 48} | 0.024 | 14 {12, 18} | 0.713 | 10 {9, 12} | 0.266 | 72 {70, 75} | 0.06 | 89 {72, 116} | 0.755 | ||
| SBT end (T3) | 3.7 {3.4, 4.1} | 53 {46, 56} | 15 {12, 16} | 9 {7, 10} | 69 {66, 71} | 92 {74, 114} | ||||||||
| FLUID-UNRESPONSIVE | ||||||||||||||
| CI (L/min/m2) | p | SVI (mL/m2) | p | SVV (%) | p | CVP (mmHg) | p | SvO2 (%) | p | TFC (1/Ω) | p | |||
| PLR start (T1) | 3.5 {3.1, 4.0} | 0.878 | 47 {43, 51} | 0.574 | 14 {8, 16} | 0.721 | 9 {8, 11} | 0.645 | 71 {69, 74} | 0.628 | 66 {55, 84} | 0.994 | ||
| PLR end (T1) | 3.5 {3.1, 4.2} | 50 {46, 53} | 13 {9, 14} | 9 {5, 12} | 74 {70, 74} | 66 {56, 87} | ||||||||
| PLR start (T2) | 3.1 {2.4, 3.4} | 0.658 | 41 {35, 45} | 0.513 | 15 {15, 24} | 0.544 | 9 {8, 10} | 0.105 | 71 {70, 73} | 0.784 | 69 {60, 71} | 0.918 | ||
| PLR end (T2) | 3.2 {2.5, 3.5} | 43 {36, 47} | 13 {12, 23} | 8 {7, 9} | 70 {69, 72} | 69 {58, 72} | ||||||||
| SBT start (T3) | 3.2 {2.7, 3.2} | 0.268 | 42 {38, 44} | 0.275 | 16 {12, 19} | 0.827 | 9 {8, 11} | 0.993 | 77 {76, 78} | 0.05 | 51 {50, 58} | 0.513 | ||
| SBT end (T3) | 3.5 {2.9, 3.7} | 49 {43, 50} | 14 {12, 19} | 9 {8, 11} | 72 {72, 73} | 52 {51, 58} | ||||||||
| (a) | ||||
| Fluid balance (postoperative) (mL) | p | Fluid balance (before SBT) (mL) | p | |
| Fluid-responsive | 5230 {3698, 5723} | 0.674 | 4476 {3697, 5722} | 0.281 |
| Fluid-unresponsive | 4167 {3755, 5583} | 2997 {−146, 5747} | ||
| (b) | ||||
| Plasma volume status (postoperative) (%) | p | Plasma volume status (before SBT) (%) | p | |
| Fluid-responsive | 17 {14, 22} | 0.156 | 17 {10, 20} | 0.226 |
| Fluid-unresponsive | 9 {5, 13} | 8 {3, 14} | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro, R.; Born, P.; Muñoz, F.; Guzmán, C.; Kattan, E.; Hernandez, G.; Bakker, J. Fluid Responsiveness Is Associated with Successful Weaning after Liver Transplant Surgery. J. Pers. Med. 2024, 14, 429. https://doi.org/10.3390/jpm14040429
Castro R, Born P, Muñoz F, Guzmán C, Kattan E, Hernandez G, Bakker J. Fluid Responsiveness Is Associated with Successful Weaning after Liver Transplant Surgery. Journal of Personalized Medicine. 2024; 14(4):429. https://doi.org/10.3390/jpm14040429
Chicago/Turabian StyleCastro, Ricardo, Pablo Born, Felipe Muñoz, Camila Guzmán, Eduardo Kattan, Glenn Hernandez, and Jan Bakker. 2024. "Fluid Responsiveness Is Associated with Successful Weaning after Liver Transplant Surgery" Journal of Personalized Medicine 14, no. 4: 429. https://doi.org/10.3390/jpm14040429