Warfarin: The End or the End of One Size Fits All Therapy?


Department of Molecular and Clinical Pharmacology, Wolfson Centre for Personalised Medicine, University of Liverpool, Liverpool L69 3GL, UK
J. Pers. Med. 2018, 8(3), 22; https://doi.org/10.3390/jpm8030022
Submission received: 7 May 2018
/
Revised: 24 June 2018
/
Accepted: 25 June 2018
/
Published: 28 June 2018
(This article belongs to the Special Issue Cytochrome P450 Variation in Pharmacogenomics)
{kind=link}
Abstract
:Oral anticoagulants are required for both treatment and prophylaxis in many different diseases. Clinicians and patients now have a choice of oral anticoagulants, including the vitamin K antagonists (of which warfarin is the most widely used and is used as the exemplar in this paper), and direct oral anticoagulants (DOACs: dabigatran, apixaban, rivaroxaban, and edoxaban). This paper explores the recent advances and controversies in oral anticoagulation. While some commentators may favour a complete switchover to DOACs, this paper argues that warfarin still has a place in therapy, and a stratified approach that enables the correct choice of both drug and dose would improve both patient outcomes and affordability.
1. Introduction
Warfarin is more than 60 years old. With the advent of direct oral anticoagulants (DOACs), some commentators have suggested that the end for warfarin is nigh [1]. However, it may be premature to write an obituary for warfarin, given its widespread use worldwide and the inability to use warfarin in some patient groups, such as in children, in patients with renal impairment, and in patients with heart valves. Furthermore, given the cost of DOACs, there may still be a place in clinical practice for a stratified approach to anticoagulation. This article examines the history of warfarin use, and in particular, the role of pharmacogenetics, and looking into the future, what still needs to be done to improve the benefit–risk ratio for all oral anticoagulants.
2. Warfarin Pharmacology and Pharmacogenetics
Warfarin is a vitamin K antagonist; it inhibits vitamin K epoxide reductase complex I (VKORC1), preventing the formation of activated vitamin K-dependent coagulation factors II, VII, IX, and X [2]. The gene VKORC1 is polymorphically expressed, which leads to variable expression and activity of the enzyme; for example, the −1639A variant at rs9923231 leads to reduced mRNA levels [3]. Warfarin is administered as a racemate, with the more potent enantiomer S-wafarin being metabolised by the P450 isoform CYP2C9 [2]. CYP2C9 genetic variants show reduced activity; for example, CYP2C9*3 is associated with a 90% reduction in catalytic activity of the enzyme [4]. It is interesting to note that the frequencies of both VKORC1 and CYP2C9 genetic polymorphisms vary with ethnicity, which has an impact on dose requirement worldwide [5,6]. It is widely acknowledged that African patients generally require higher doses than Caucasians, while Chinese patients require lower doses.
There is no doubt that warfarin is an effective drug for the treatment of venous thromboembolism and for prophylaxis against strokes in patients with atrial fibrillation [7]. However, warfarin is also associated with bleeding, estimated to be about 7.2 events per 100 patient years [8]. Indeed, warfarin is amongst the top three drugs responsible for adverse drug reaction related hospital admissions [9]. The major issue with warfarin is the inability to predict inter-individual variability in daily dose requirements. Some patients require 0.5 mg per day to maintain therapeutic anticoagulation, for example—an International Normalised Ratio (INR) between 2 and 3 in the treatment of atrial fibrillation—while others may require 20 mg per day—a variability of more than 40-fold. We have known for many decades that this variability is partly dependent on clinical factors, such as age, body-mass index (BMI), drug–drug interactions, and concomitant diseases [2]. However, apart from age, none of these clinical predictors have routinely been utilised in dosing regimens.
In order to improve the predictability of daily warfarin dose requirements, many groups worldwide have evaluated the role of genetic and clinical factors. These studies have consistently shown that genetic polymorphisms in CYP2C9 and VKORC1 account for a greater degree of variance in daily dose requirement compared with clinical factors, such as age, BMI, and interactions with drugs such as amiodarone [10,11]. Indeed, the association of warfarin dose requirement with genetic factors is one of the most highly replicated genotype–phenotype associations. Another genetic factor associated with the warfarin dose requirement is the CYP4F2 genetic variant at rs2108622 (V433M) [12], the effect being due to differential vitamin K hydroxylation [13]. However, the overall effect size of CYP4F2 is much lower than that of CYP2C9 and VKORC1, accounting for about 1% of the variability in the warfarin dose requirement [14].
One of the most important developments in warfarin pharmacogenetics was the formation of the International Warfarin Pharmacogenetics Consortium (IWPC) that brought together 21 research groups from nine countries and four continents, with analysable data from about 5000 patients [15]. The IWPC developed clinical and genetic warfarin dosing algorithms. The genetic dosing algorithm was superior to the clinical dosing algorithm, with the greatest benefit being observed in about half of the patients who required either less than 21 mg of warfarin per week or more than 49 mg per week.
An important next step in the demonstration of the utility of genotype-guided dosing for warfarin was to demonstrate whether the genetic algorithm was superior to either standard care or a clinical algorithm. A number of clinical trials had already been conducted in this area with variable designs and disparate sample sizes, with inconclusive findings [16]. Because of this, two larger randomized controlled trials (RCTs) were undertaken, one in the United States (Clarification of Optimal Anticoagulation through Genetics; COAG) [17] and another in the European Union (EU Pharmacogenetics of Anticoagulant Therapy; EU-PACT) [18]. There were numerous differences in the design of the two trials [16], with COAG comparing a clinical algorithm to a genetic algorithm, while EU-PACT compared standard care in two European countries (the United Kingdom (UK) and Sweden) to the genetic algorithm. Unfortunately, but perhaps not surprisingly, given the differences in trial design, the results of the two trials were starkly different, with EU-PACT showing the superiority of the genetic algorithm over the comparator arm [19], while in COAG there was no difference between the test and control arms [20]. This led to confusion and criticisms of both trials and the conclusion that pharmacogenetic dosing of warfarin was not clinically useful [21,22]. Perhaps, this is consistent with the recent paper in Science, which highlighted that negative stories are more likely to get traction when compared with positive news [23]. Interestingly, following the publication of the trials, it was also suggested that dosing should be based on a clinical algorithm, rather than the standard dosing currently used in clinical care, despite the fact that there has been no RCT that has compared a clinical algorithm to standard of care. This is perhaps another example of genetic exceptionalism, where a lower burden of proof is considered acceptable for non-genetic interventions when compared with genetic testing. In retrospect, it would have been better to conduct three-armed trials, where genotype-guided dosing was compared simultaneously with both a clinical algorithm and standard dosing.
The reasons for the different outcomes in the two trials have been widely debated and included differences in algorithms, differences in the comparator arms, and greater ethnic heterogeneity in COAG compared with EU-PACT [16]. The design of any algorithm is, of course, crucial, and it must take into account ethnic heterogeneity (including the relevant ethnic-specific single nucleotide polymorphisms (SNPs)) and the known pharmacology of warfarin, including its long half-life. It is also fair to state that no algorithm is perfect, because not all factors that determine warfarin dosing have been identified [10]. The algorithms also predict extreme doses less efficiently (i.e., low or high daily warfarin doses) [15,24]. Algorithms designed for African-American, Indian, and Chinese patients have been developed but have not been tested in clinical trials [25,26,27].
More recently, the Genetics Informatics Trial (GIFT) has been published [28], conducted in 1650 randomised patients. This used a composite primary outcome measure comprising major bleeding, INR of four or greater, venous thromboembolism, or death. The trial found that 10.8% of the genotype-guided group met at least one of the endpoints compared with 14.7% in the clinically guided warfarin group, a 27% improvement in favour of genotype-guided dosing. The results are consistent with EU-PACT [19], but GIFT has the advantage of having included clinical outcomes as part of the primary endpoint. Indeed, EU-PACT and COAG were both criticised for having used percentage time in therapeutic range (%TTR), a surrogate measure, as the primary outcome measure [22]. Of course, a trial that used only clinical events (thromboembolic or bleeding) as the primary outcome would be preferable but would have required a sample size close to 20,000 patients. It is also important to note that an improvement in %TTR greater than 10% can lead to a 20% improvement in clinical outcomes [29].
From the EU-PACT trial data, it has been shown that genotyping prior to warfarin prescription would be cost effective in both the UK and Sweden [30]. Data on cost-effectiveness from other healthcare systems is awaited [31]. The 2017 Clinical Pharmacology Implementation Consortium (CPIC) guideline on warfarin provides detailed guidance on dosing in patients with variant alleles, including race-specific recommendations [32]. The Dutch Pharmacogenetic Working Group has also developed guidelines for the dosing of vitamin K antagonists, and there is a high overall rate of concordance between the guidelines produced by the Dutch Group and the CPIC [33].
3. Direct Oral Anticoagulants
Oral anticoagulants acting via the vitamin K-dependent pathway were the only choices available for clinicians until recently. The introduction of direct acting oral anticoagulants (DOACs) has provided greater choice for both clinicians and patients. These drugs act by inhibiting either thrombin (dabigatran) or factor Xa (apixaban, rivaroxaban, edoxaban). Large RCTs in atrial fibrillation and venous thromboembolism have shown that DOACs are either non-inferior or superior to warfarin, with a reduced risk of intracranial haemorrhage but with a possibly increased risk of gastro-intestinal bleeding [34].
DOACs have been marketed on the basis that “one-dose-fits-all” and that no monitoring is required. There has been rapid uptake of these drugs particularly in western countries, while the use of warfarin has declined [1]. This may well herald the beginning of the end for warfarin, but I feel this is premature for several reasons.
First, although the new DOACs have been shown to be cost-effective [35], there are concerns about the cost outlay given the large population that needs to be treated. It has been estimated that there are 8.8 million people with atrial fibrillation in the European Union, and this will double to 17 million in 2060 [36]. In the UK, it has been estimated that expenditure on DOACs may top £1 billion per year by 2020, about 5% of the overall spend on drugs in the National Health Services (NHS) [37]. One possible method to improve affordability and ensure that all patients have access to oral anticoagulation would be to stratify treatment according to genotypes for CYP2C9 and VKORC1. The evidence for this comes from analyses of the warfarin arm in the edoxaban ENGAGE AF-TIMI 48 trial [38]. This showed that warfarin increased the risk of bleeding in those patients who carried variant alleles for CYP2C9 and/or VKORC1, classified as sensitive or highly sensitive responders, when compared with normal responders, who represented 62% of the population. A more recent analysis of the Hokusai-venous thromboembolism trial [39] has replicated this finding, showing that sensitive and highly sensitive responders spent more time over-anticoagulated with warfarin and had a higher bleeding risk compared with normal responders (who represented 63% of the population). Thus, it may be possible to personalise the use of oral anticoagulants in the future so that patients with the low-risk genotypes (i.e., normal responders, at least 60%) would get warfarin, while those classified as sensitive or highly sensitive would get DOACs. This would lead to significant savings in expenditure [37] without any compromise in clinical outcomes.
An important issue to consider for taking forward the stratification approach is whether it is possible to implement warfarin genotyping in a clinical setting. Following the EU-PACT trial [19], and despite the conflicting results with COAG [20], we have undertaken an implementation study. The premise behind the study was to determine whether staff running anticoagulant clinics (predominantly qualified nurses) could modify the current clinical pathway so that genotyping, and subsequent genotype-guided dosing, could be incorporated. This required an improvement in the point-of-care genotyping assay. In EU-PACT, the point-of-care genotyping platform was able to provide results on three alleles (CYP2C9*2, CYP2C9*3, and VKORC1) in 2 h [19]. For the implementation study, the platform was modified to provide results within 45 min. The results of the implementation study (unpublished) were equivalent to those of the EU-PACT RCT, demonstrating that long and well-established clinical pathways could be modified using new technologies.
Second, an unintended consequence of the “no or minimal monitoring” strategy adopted for DOACs may be poor adherence. Our recent data suggest that adherence to DOACs was significantly worse when compared with warfarin [37]. Although INR monitoring is disliked by both patients and clinicians, it does act as a positive reinforcement for patients to continue taking warfarin. It is important to note that there has also been criticism of the “one-dose-fits all” strategy for DOACs, with some patients having been shown to be under-dosed, while others may be over-dosed [40]. Pharmacogenomic studies have identified some associations with plasma concentrations of these drugs, but none of the genetic variants are likely to be useful in improving the clinical use of these drugs [41,42]. Instead, it has been argued that plasma therapeutic drug monitoring should be utilised [43], especially in high-risk patients to individualise dose. High-risk groups could include patients at high risk of bleeding, those on drugs likely to interact with DOACs, and patients with borderline renal impairment, to name a few. Clearly, this would lead to a loss of the marketing advantage for DOACs, increase cost and inconvenience for patients, and may thus face an uphill battle for implementation.
Third, there are some patients where DOACs are not used because of contraindications, no marketing authorization, or unaffordability. In these situations (outlined below), warfarin remains the only alternative.
- (a)
- Patients with renal impairment: all the drug labels for DOACs have criteria, which either recommend a dose reduction or absolutely contraindicate the use of the DOAC [44]. While it may be relatively easy to avoid the use of DOACs in patients with severe forms of renal impairment, a group that may be at particular risk are patients with incipient renal impairment, where there may be asymptomatic and slow decline in renal function with age or an acute decline in an elderly patient because of a concomitant urinary tract infection. This is compounded by the fact that monitoring of renal function in patients on DOACs is poorly performed.
- (b)
- Patients on interacting drugs: Although DOACs are less likely to be involved in drug–drug interactions than warfarin, they are not immune from them. For patients on certain medications—for example, itraconazole—the use of apixaban is not recommended. A recent database study from Taiwan showed that concomitant use of drugs, such as amiodarone, fluconazole, rifampicin, and phenytoin, increased the risk of major bleeding when compared with the use of DOACs alone [45]. There is no simple biomarker that can be used to individualise dosing with DOACs, unlike warfarin, where INR monitoring provides the opportunity to change dosage to maintain the INR within a therapeutic range.
- (c)
- Use in children: DOACs are currently not licensed for use in children, but there are paediatric investigation plans in place [46]. Thus, for the time being, warfarin (or other vitamin K antagonists) remain the only alternatives. There have been numerous studies in children investigating the effects of genetic polymorphisms on warfarin dosing [47,48,49,50], but no algorithm has been tested in clinical trials.
- (d)
- Mechanical heart valves: DOACs are currently contraindicated in patients with mechanical heart valves. In the RE-ALIGN trial, after enrolment of 252 patients, an increased risk of bleeding and thrombosis was seen in patients on dabigatran, compared with warfarin, which resulted in premature discontinuation of the trial [51].
Fourth, because of the cost of DOACs, their uptake in developing countries has been low, and thus, warfarin (or other vitamin K antagonists) remains the main choice. Unfortunately, the genetic and clinical factors affecting warfarin dose variation have been poorly studied in developing countries, and, even in developed countries, in minority groups compared with Caucasian populations [6]. The frequencies of genetic variants in CYP2C9 and VKORC1 vary with ethnicity. Thus, in Chinese patents, CYP2C9*2 is less important than in Caucasians [52]. In African-Americans, both CYP2C9*2 and CYP2C9*3 have a low prevalence, with other variant alleles (*8, *11) being more important [6]. The importance of this was highlighted by the COAG trial [20], where genotype-guided dosing actually fared worse than clinical dosing in African-American patients. In Africa, where access to medicines and services is limited, warfarin remains the obvious choice for oral anticoagulation. However, dosing regimens are largely empirical and not evidence-based, which—coupled with the lack of infrastructure—leads to poor quality of anticoagulation. For example, in South Africa, a recent study showed that only 28% of patients achieved a therapeutic INR [53]. The importance of achieving better anticoagulation control in developing countries is shown by a study in South Africa, which demonstrated that haemorrhage was the fourth most common cause of hospital admission, with warfarin accounting for 68% of the bleeds [54]. We have recently embarked on a large programme of work in Uganda and South Africa (War-PATH: WARfarin anticoagulation in PATients in Sub-SaHaran Africa; http://warpath.info/), the aim of which is to identify the clinical and genetic factors determining variation in daily warfarin dose requirements and thereby, develop better clinical and genetic dosing algorithms to improve anticoagulation quality.
4. Conclusions
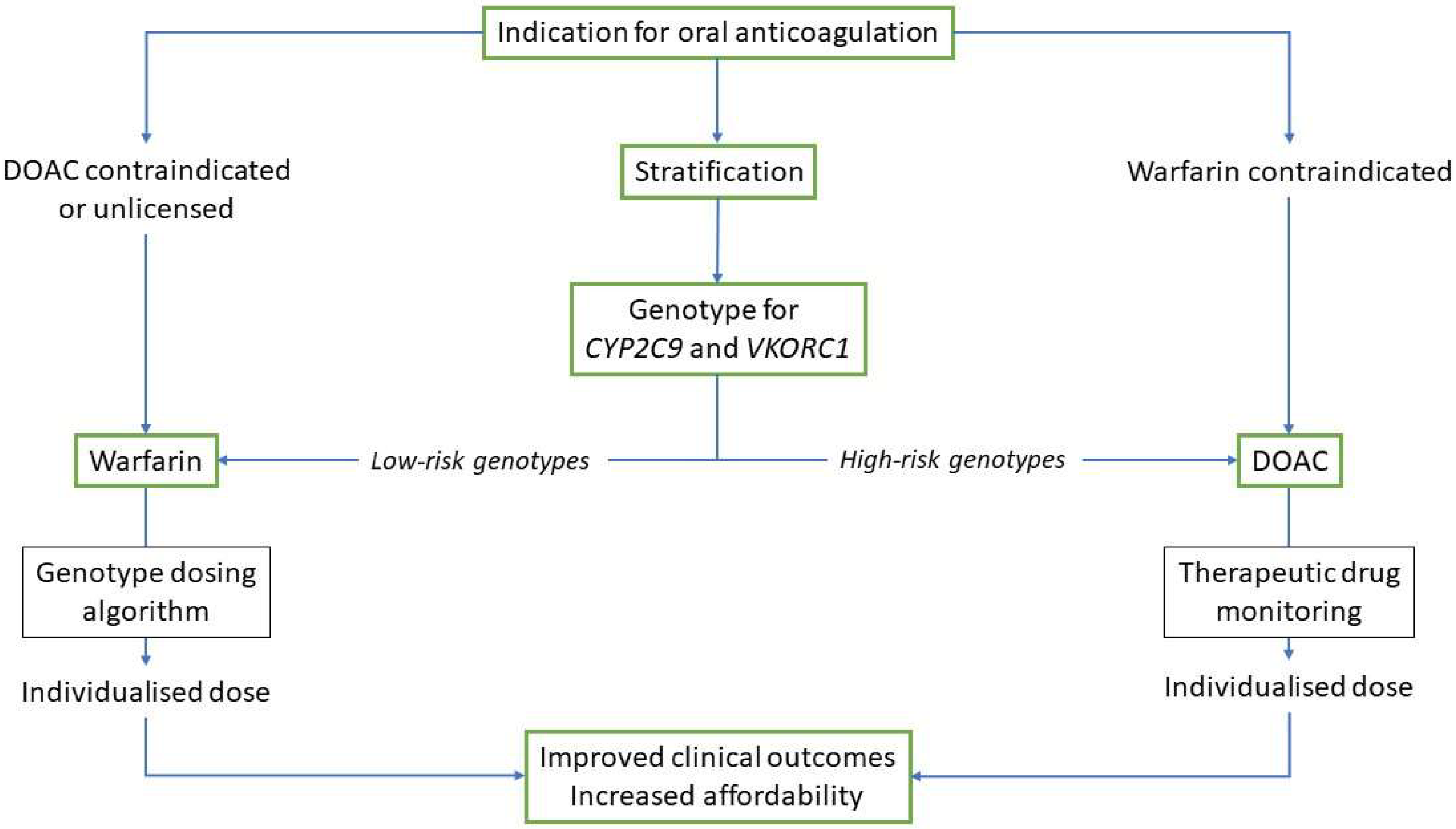
It has been estimated that the global anticoagulants market will be worth close to $30 billion by 2021 (https://www.businesswire.com/news/home/20170301005087/en/Increase-Lifestyle-Diseases-Boost-Global-Anticoagulant-Market). For both clinicians and patients, it is important to have a choice of drugs to use for either treatment or prophylaxis, and the availability of DOACs has certainly provided that choice. However, that does not mean that older drugs have no place in the therapeutic armamentarium, as I have pointed out in the case of warfarin. Undoubtedly, we can continue to improve the benefit–risk ratio of all oral anticoagulants that are available, and a stratified approach to the choice of drug, and the precise dose of that drug (Figure 1), may be an option that not only maximises the positive clinical outcomes but also improves affordability and access. Whether this would be a cost-effective approach would need further study; however, it is clear that the cost-effectiveness of DOACs is reduced or nullified when the quality of anticoagulation with warfarin improves [55], which is likely to be the consequence of a stratified approach.
Funding
The research on warfarin has been funded from a number of funding agencies, including the UK Department of Health, the UK Medical Research Council (MRC), the National Institute of Health Research (NIHR), and the EU Commission.
Acknowledgments
The author acknowledges the support of the MRC Centre for Drug Safety Science, the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) North West Coast, and the Innovation Agency and the EU FP7 Framework funding programme.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sotiriou, A.; Patel, H.C.; Tyebally, S.; Raza, S.; Qudah, T.; Malik, K.; Patel, K.; Bhattacharyya, S.; Chow, A.; Hayward, C. Is this the beginning of the end for warfarin? EP Eur. 2017, 19, i28. [Google Scholar] [CrossRef]
- Wadelius, M.; Pirmohamed, M. Pharmacogenetics of warfarin: Current status and future challenges. Pharmacogenomics J. 2007, 7, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Rieder, M.J.; Reiner, A.P.; Gage, B.F.; Nickerson, D.A.; Eby, C.S.; McLeod, H.L.; Blough, D.K.; Thummel, K.E.; Veenstra, D.L.; Rettie, A.E. Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N. Engl. J. Med. 2005, 352, 2285–2293. [Google Scholar] [CrossRef] [PubMed]
- Rettie, A.E.; Wienkers, L.C.; Gonzalez, F.J.; Trager, W.F.; Korzekwa, K.R. Impaired (S)-warfarin metabolism catalysed by the R144C allelic variant of CYP2C9. Pharmacogenetics 1994, 4, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.A.; Wadelius, M.; Cavallari, L.; Eriksson, N.; Crawford, D.C.; Lee, M.T.; Chen, C.H.; Motsinger-Reif, A.; Sagreiya, H.; Liu, N.; et al. Warfarin pharmacogenetics: A single VKORC1 polymorphism is predictive of dose across 3 racial groups. Blood 2010, 115, 3827–3834. [Google Scholar] [CrossRef] [PubMed]
- Cavallari, L.H.; Perera, M.A. The future of warfarin pharmacogenetics in under-represented minority groups. Future Cardiol. 2012, 8, 563–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar, M.I.; Hart, R.; Pearce, L.A. Oral anticoagulants versus antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no history of stroke or transient ischemic attacks. Cochrane Database Syst. Rev. 2007, CD006186. [Google Scholar] [CrossRef] [PubMed]
- Linkins, L.A.; Choi, P.T.; Douketis, J.D. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: A meta-analysis. Ann. Int. Med. 2003, 139, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18,820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, S.; Jorgensen, A.; Zhang, E.J.; Hanson, A.; Gillman, M.S.; Bumpstead, S.; Toh, C.H.; Williamson, P.; Daly, A.K.; Kamali, F.; et al. A multi-factorial analysis of response to warfarin in a UK prospective cohort. Genome Med. 2016, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Wadelius, M.; Chen, L.Y.; Lindh, J.D.; Eriksson, N.; Ghori, M.J.; Bumpstead, S.; Holm, L.; McGinnis, R.; Rane, A.; Deloukas, P. The largest prospective warfarin-treated cohort supports genetic forecasting. Blood 2009, 113, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, M.D.; Awad, T.; Johnson, J.A.; Gage, B.F.; Falkowski, M.; Gardina, P.; Hubbard, J.; Turpaz, Y.; Langaee, T.Y.; Eby, C.; et al. CYP4F2 genetic variant alters required warfarin dose. Blood 2008, 111, 4106–4112. [Google Scholar] [CrossRef] [PubMed]
- Edson, K.Z.; Prasad, B.; Unadkat, J.D.; Suhara, Y.; Okano, T.; Guengerich, F.P.; Rettie, A.E. Cytochrome P450-dependent catabolism of vitamin K: ω-hydroxylation catalyzed by human CYP4F2 and CYP4F11. Biochemistry 2013, 52, 8276–8285. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Montagnana, M.; Johnson, J.A.; Rettie, A.E.; Zambon, C.F.; Lubitz, S.A.; Suarez-Kurtz, G.; Cavallari, L.H.; Zhao, L.; Huang, M.; et al. Impact of the CYP4F2 p.V433m polymorphism on coumarin dose requirement: Systematic review and meta-analysis. Clin. Pharmacol. Ther. 2012, 92, 746–756. [Google Scholar] [CrossRef] [PubMed]
- International Warfarin Pharmacogenetics Consortium; Klein, T.E.; Altman, R.B.; Eriksson, N.; Gage, B.F.; Kimmel, S.E.; Lee, M.T.; Limdi, N.A.; Page, D.; Roden, D.M.; et al. Estimation of the warfarin dose with clinical and pharmacogenetic data. N. Engl. J. Med. 2009, 360, 753–764. [Google Scholar] [PubMed]
- Pirmohamed, M.; Kamali, F.; Daly, A.K.; Wadelius, M. Oral anticoagulation: A critique of recent advances and controversies. Trends Pharmacol. Sci. 2015, 36, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, S.E.; French, B.; Anderson, J.L.; Gage, B.F.; Johnson, J.A.; Rosenberg, Y.D.; Geller, N.L.; Kasner, S.E.; Eby, C.S.; Joo, J.; et al. Rationale and design of the clarification of optimal anticoagulation through genetics trial. Am. Heart J. 2013, 166, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Van Schie, R.M.; Wadelius, M.I.; Kamali, F.; Daly, A.K.; Manolopoulos, V.G.; de Boer, A.; Barallon, R.; Verhoef, T.I.; Kirchheiner, J.; Haschke-Becher, E.; et al. Genotype-guided dosing of coumarin derivatives: The European pharmacogenetics of anticoagulant therapy (EU-PACT) trial design. Pharmacogenomics 2009, 10, 1687–1695. [Google Scholar] [CrossRef] [PubMed]
- Pirmohamed, M.; Burnside, G.; Eriksson, N.; Jorgensen, A.L.; Toh, C.H.; Nicholson, T.; Kesteven, P.; Christersson, C.; Wahlstrom, B.; Stafberg, C.; et al. A randomized trial of genotype-guided dosing of warfarin. N. Engl. J. Med. 2013, 369, 2294–2303. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, S.E.; French, B.; Kasner, S.E.; Johnson, J.A.; Anderson, J.L.; Gage, B.F.; Rosenberg, Y.D.; Eby, C.S.; Madigan, R.A.; McBane, R.B.; et al. A pharmacogenetic versus a clinical algorithm for warfarin dosing. N. Engl. J. Med. 2013, 369, 2283–2293. [Google Scholar] [CrossRef] [PubMed]
- Zineh, I.; Pacanowski, M.; Woodcock, J. Pharmacogenetics and coumarin dosing—Recalibrating expectations. N. Engl. J. Med. 2013, 369, 2273–2275. [Google Scholar] [CrossRef] [PubMed]
- Furie, B. Do pharmacogenetics have a role in the dosing of vitamin K antagonists? N. Engl. J. Med. 2013, 369, 2345–2346. [Google Scholar] [CrossRef] [PubMed]
- Vosoughi, S.; Roy, D.; Aral, S. The spread of true and false news online. Science 2018, 359, 1146–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saffian, S.; Duffull, S.; Wright, D. Warfarin dosing algorithms underpredict dose requirements in patients requiring ≥7 mg daily: A systematic review and meta-analysis. Clin. Pharmacol. Ther. 2017, 102, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Ye, F.; Xie, D.; Zhu, Y.; Zhu, J.; Tao, Y.; Yu, F. A new algorithm to predict warfarin dose from polymorphisms of CYP4F2, CYP2C9 and VKORC1 and clinical variables: Derivation in Han Chinese patients with non valvular atrial fibrillation. Thromb. Haemost. 2012, 107, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Gaikwad, T.; Ghosh, K.; Avery, P.; Kamali, F.; Shetty, S. Warfarin dose model for the prediction of stable maintenance dose in indian patients. Clin. Appl. Thromb./Hemost. 2018, 24, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Kubo, K.; Ohara, M.; Tachikawa, M.; Cavallari, L.H.; Lee, M.T.M.; Wen, M.S.; Scordo, M.G.; Nutescu, E.A.; Perera, M.A.; Miyajima, A.; et al. Population differences in s-warfarin pharmacokinetics among African Americans, Asians and Whites: Their influence on pharmacogenetic dosing algorithms. Pharmacogenomics J. 2016, 17, 494. [Google Scholar] [CrossRef] [PubMed]
- Gage, B.F.; Bass, A.R.; Lin, H.; Woller, S.C.; Stevens, S.M.; Al-Hammadi, N.; Li, J.; Rodriguez, T., Jr.; Miller, J.P.; McMillin, G.A.; et al. Effect of genotype-guided warfarin dosing on clinical events and anticoagulation control among patients undergoing hip or knee arthroplasty: The gift randomized clinical trial. JAMA 2017, 318, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Van Spall, H.G.C.; Wallentin, L.; Yusuf, S.; Eikelboom, J.W.; Nieuwlaat, R.; Yang, S.; Kabali, C.; Reilly, P.A.; Ezekowitz, M.D.; Connolly, S.J. Variation in warfarin dose adjustment practice is responsible for differences in the quality of anticoagulation control between centers and countries. An analysis of patients receiving warfarin in the randomized evaluation of long-term anticoagulation therapy (RE-LY) trial. Circulation 2012, 126, 2309–2316. [Google Scholar] [PubMed]
- Verhoef, T.I.; Redekop, W.K.; Langenskiold, S.; Kamali, F.; Wadelius, M.; Burnside, G.; Maitland-van der Zee, A.H.; Hughes, D.A.; Pirmohamed, M. Cost-effectiveness of pharmacogenetic-guided dosing of warfarin in the United Kingdom and Sweden. Pharmacogenomics J. 2016, 16, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Plumpton, C.O.; Roberts, D.; Pirmohamed, M.; Hughes, D.A. A systematic review of economic evaluations of pharmacogenetic testing for prevention of adverse drug reactions. PharmacoEconomics 2016, 34, 771–793. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Caudle, K.E.; Gong, L.; Whirl-Carrillo, M.; Stein, C.M.; Scott, S.A.; Lee, M.T.; Gage, B.F.; Kimmel, S.E.; Perera, M.A.; et al. Clinical pharmacogenetics implementation consortium (CPIC) guideline for pharmacogenetics-guided warfarin dosing: 2017 update. Clin. Pharmacol. Ther. 2017, 102, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Bank, P.C.D.; Caudle, K.E.; Swen, J.J.; Gammal, R.S.; Whirl-Carrillo, M.; Klein, T.E.; Relling, M.V.; Guchelaar, H.J. Comparison of the guidelines of the clinical pharmacogenetics implementation consortium and the dutch pharmacogenetics working group. Clin. Pharmacol. Ther. 2018, 103, 599–618. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new Oral Anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Lopez-Lopez, J.A.; Sterne, J.A.C.; Thom, H.H.Z.; Higgins, J.P.T.; Hingorani, A.D.; Okoli, G.N.; Davies, P.A.; Bodalia, P.N.; Bryden, P.A.; Welton, N.J.; et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: Systematic review, network meta-analysis, and cost effectiveness analysis. BMJ 2017, 359, j5058. [Google Scholar] [CrossRef] [PubMed]
- Barra, S.; Fynn, S. Untreated atrial fibrillation in the United Kingdom: Understanding the barriers and treatment options. J. Saudi Heart Assoc. 2015, 27, 31–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burn, J.; Pirmohamed, M. Direct oral anticoagulants versus warfarin: Is new always better than the old? Open Heart 2018, 5, e000712. [Google Scholar] [CrossRef] [PubMed]
- Mega, J.L.; Walker, J.R.; Ruff, C.T.; Vandell, A.G.; Nordio, F.; Deenadayalu, N.; Murphy, S.A.; Lee, J.; Mercuri, M.F.; Giugliano, R.P.; et al. Genetics and the clinical response to warfarin and edoxaban: Findings from the randomised, double-blind engage Af-Timi 48 trial. Lancet 2015, 385, 2280–2287. [Google Scholar] [CrossRef]
- Vandell, A.G.; Walker, J.; Brown, K.S.; Zhang, G.; Lin, M.; Grosso, M.A.; Mercuri, M.F. Genetics and clinical response to warfarin and edoxaban in patients with venous thromboembolism. Heart 2017, 103, 1800. [Google Scholar] [CrossRef] [PubMed]
- Gulilat, M.; Tang, A.; Gryn, S.E.; Leong-Sit, P.; Skanes, A.C.; Alfonsi, J.E.; Dresser, G.K.; Henderson, S.L.; Rose, R.V.; Lizotte, D.J.; et al. Interpatient variation in rivaroxaban and apixaban plasma concentrations in routine care. Can. J. Cardiol. 2017, 33, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Asic, A.; Marjanovic, D.; Mirat, J.; Primorac, D. Pharmacogenetics of novel oral anticoagulants: A review of identified gene variants & future perspectives. Per. Med. 2018, 15, 209–221. [Google Scholar] [PubMed]
- Tseng, A.S.; Patel, R.D.; Quist, H.E.; Kekic, A.; Maddux, J.T.; Grilli, C.B.; Shamoun, F.E. Clinical review of the pharmacogenomics of direct oral anticoagulants. Cardiovasc. Drugs Ther. 2018, 32, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Powell, J. Are new oral anticoagulant dosing recommendations optimal for all patients? JAMA 2015, 313, 1013–1014. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.; Jurk, K.; Schinzel, H. Direct oral anticoagulants in patients with chronic kidney disease: Patient selection and special considerations. Int. J. Nephrol. Renovasc. Dis. 2017, 10, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Chou, I.J.; Yeh, Y.H.; Chiou, M.J.; Wen, M.S.; Kuo, C.T.; See, L.C.; Kuo, C.F. Association between use of non-vitamin K oral anticoagulants with and without concurrent medications and risk of major bleeding in nonvalvular atrial fibrillation. JAMA 2017, 318, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Newall, F.; Branchford, B.; Male, C. Anticoagulant prophylaxis and therapy in children: Current challenges and emerging issues. J. Thromb. Haemost. 2018, 16, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Biss, T.; Hamberg, A.K.; Avery, P.; Wadelius, M.; Kamali, F. Warfarin dose prediction in children using pharmacogenetics information. Br. J. Haematol. 2012, 159, 106–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vear, S.I.; Stein, C.M.; Ho, R.H. Warfarin pharmacogenomics in children. Pediatric Blood Cancer 2013, 60, 1402–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamberg, A.-K.; Wadelius, M. Pharmacogenetics-based warfarin dosing in children. Pharmacogenomics 2014, 15, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Hawcutt, D.B.; Ghani, A.A.; Sutton, L.; Jorgensen, A.; Zhang, E.; Murray, M.; Michael, H.; Peart, I.; Smyth, R.L.; Pirmohamed, M. Pharmacogenetics of warfarin in a paediatric population: Time in therapeutic range, initial and stable dosing and adverse effects. Pharmacogenomics J. 2014, 14, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus warfarin in patients with mechanical heart valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.T.; Klein, T.E. Pharmacogenetics of warfarin: Challenges and opportunities. J. Hum. Genet. 2013, 58, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Zuhlke, L.; Engel, M.E.; Karthikeyan, G.; Rangarajan, S.; Mackie, P.; Cupido, B.; Mauff, K.; Islam, S.; Joachim, A.; Daniels, R.; et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: The global rheumatic heart disease registry (the remedy study). Eur. Heart J. 2015, 36, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.P.; Njuguna, C.; Kramer, N.; Stewart, A.; Mehta, U.; Blockman, M.; Fortuin-De Smidt, M.; De Waal, R.; Parrish, A.G.; Wilson, D.P.; et al. Adverse drug reactions causing admission to medical wards: A cross-sectional survey at 4 hospitals in South Africa. Medicine 2016, 95, e3437. [Google Scholar] [CrossRef] [PubMed]
- Pink, J.; Lane, S.; Pirmohamed, M.; Hughes, D.A. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: Quantitative benefit-harm and economic analyses. BMJ 2011, 343, d6333. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical pathways for stratification in the use of oral anticoagulants. Use of either warfarin or a direct oral anticoagulant (DOAC) would require individualisation of the dose to improve time in therapeutic range and optimisation of anticoagulation, resulting in improved clinical outcomes. This would also result in improved affordability.
Figure 1.
Clinical pathways for stratification in the use of oral anticoagulants. Use of either warfarin or a direct oral anticoagulant (DOAC) would require individualisation of the dose to improve time in therapeutic range and optimisation of anticoagulation, resulting in improved clinical outcomes. This would also result in improved affordability.

© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pirmohamed, M. Warfarin: The End or the End of One Size Fits All Therapy? J. Pers. Med. 2018, 8, 22. https://doi.org/10.3390/jpm8030022
AMA Style
Pirmohamed M. Warfarin: The End or the End of One Size Fits All Therapy? Journal of Personalized Medicine. 2018; 8(3):22. https://doi.org/10.3390/jpm8030022
Chicago/Turabian StylePirmohamed, Munir. 2018. "Warfarin: The End or the End of One Size Fits All Therapy?" Journal of Personalized Medicine 8, no. 3: 22. https://doi.org/10.3390/jpm8030022
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.