

Unlicensed Molnupiravir is an Effective Rescue Treatment Following Failure of Unlicensed GS-441524-like Therapy for Cats with Suspected Feline Infectious Peritonitis

Abstract
:1. Introduction
2. Materials and Methods
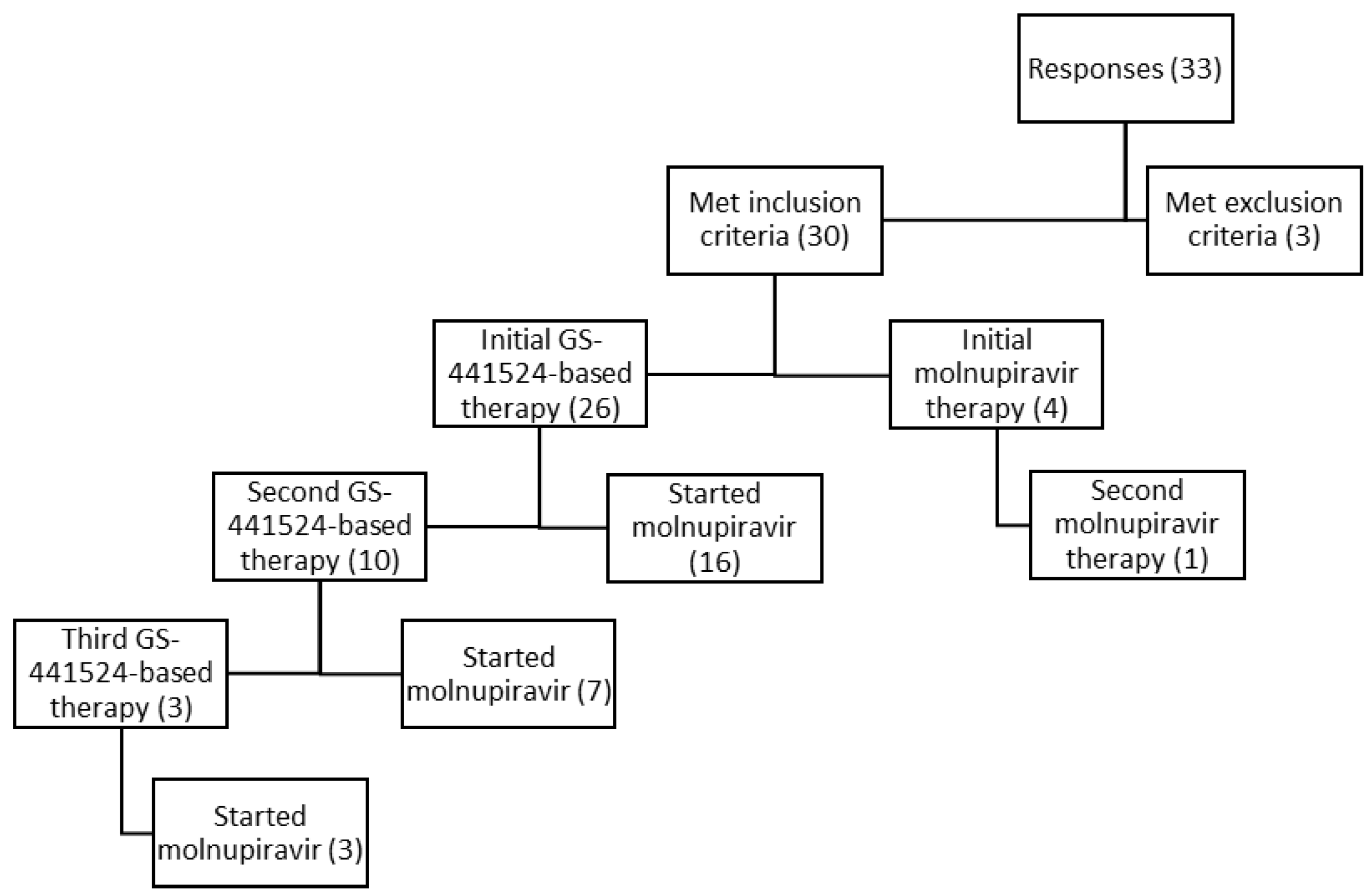
3. Results
3.1. Demographics
3.2. Initial Therapy Prior to Molnupiravir
3.3. Second Therapy Prior to Molnupiravir
3.4. Third Therapy Prior to Molnupiravir
3.5. Molnupiravir as Rescue Therapy
3.6. Molnupiravir as a First-Line Therapy
3.7. Molnupiravir Based on Type of FIP
3.8. Cost and Owner Satisfaction
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Felten, S.; Hartmann, K. Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature. Viruses 2019, 11, 1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, N.C.; Kim, Y.; Liu, H.; Kankanamalage, A.C.G.; Eckstrand, C.; Groutas, W.C.; Bannasch, M.; Meadows, J.M.; Chang, K.-O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-Like Antiviral Therapy Can Be Effective for At-Home Treatment of Feline Infectious Peritonitis. Animals 2021, 11, 2257. [Google Scholar] [CrossRef] [PubMed]
- Merck & Co., Inc. Authorized for Emergency Use in the Treatment of COVID-19. Lagevrio. 2022. Available online: https://www.lagevrio.com/patients/ (accessed on 26 August 2022).
- Gordon, C.J.; Tchesnokov, E.P.; Schinazi, R.F.; Götte, M. Molnupiravir promotes SARS-CoV-2 mutagenesis via the RNA template. J. Biol. Chem. 2021, 297, 100770. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, A.; Singh, R.; Misra, A. Molnupiravir in COVID-19: A systematic review of literature. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102329. [Google Scholar] [CrossRef] [PubMed]
- Khoo, S.H.; Fitzgerald, R.; Fletcher, T.; Ewings, S.; Jaki, T.; Lyon, R.; Downs, N.; Walker, L.; Tansley-Hancock, O.; Greenhalf, W.; et al. Optimal dose and safety of molnupiravir in patients with early SARS-CoV-2: A Phase I, open-label, dose-escalating, randomized controlled study. J. Antimicrob. Chemother. 2021, 76, 3286–3295. [Google Scholar] [CrossRef] [PubMed]
- FIP Warriors CZ/SK® (2022, May 20). Eidd-2801 (Molnupiravir). Available online: https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/ (accessed on 26 August 2022).
- Pedersen, N.C.; Jacque, N. Alternative Treatments for Cats with FIP and Natural or Acquired Resistance to GS-441524. Sock it to Fip. Available online: https://sockfip.org/https-sockfip-org-wp-content-uploads-2022-03-approaches-to-drug-resistance-in-cats-treated-with-gs-441524-for-fip-v3-pdf/ (accessed on 26 August 2022).
- Pedersen, N.C. The Long History of Beta-d-n4-Hydroxycytidine and Its Modern Application to Treatment of COVID-19 in People and FIP in Cats. Sock it to Fip. Available online: https://sockfip.org/https-sockfip-org-wp-content-uploads-2022-04-the-long-history-of-beta-d-n4-hydroxycytidine-and-its-modern-application-to-treatment-of-covid-19-in-people-and-fip-in-cats-v2-pdf/ (accessed on 8 October 2022).
- European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP) Assessment Report: Use of Mol-Nupiravir for the Treatment of COVID-19. 2022. Available online: www.ema.europa.eu/contact (accessed on 8 October 2022).
- Painter, G.R.; Bowen, R.A.; Bluemling, G.R.; DeBergh, J.; Edpuganti, V.; Gruddanti, P.R.; Guthrie, D.B.; Hager, M.; Kuiper, D.L.; Lockwood, M.A.; et al. The prophylactic and therapeutic activity of a broadly active ribonucleoside analog in a murine model of intranasal venezuelan equine encephalitis virus infection. Antivir. Res. 2019, 171, 104597. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, T.; Ah Donovan-Banneld, I.; Penrice-Randal, R.; Goldswain, H.; Rzeszutek, A.; Pilgrim, J.; Bullock, K.; Saunders, G.; Northey, J.; Dong, X.; et al. Characterisation of SARS-CoV-2 genomic variations in response to mol-nupiravir treatment in the AGILE Phase IIa clinical trial. Res. Sq. 2022. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cat | Age at Diagnosis (Months) | Sex/Neuter Status at Diagnosis | Breed | Pre-Existing Medical Condititons | Country of Origin | Form of FIP | Initial Therapy | Initial Therapy Duration (Weeks) | Disease Free Interval | Second Therapy | Second Therapy Duration (Weeks) | Disease Free Interval | Third Therapy | Third Therapy Duration (Weeks) | Disease Free Interval |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 4 | Male | European Shorthair | Parasitic infections, URI as kitten | Germany | Neurological | Injectable Oral GS-441524 | 8 | None | Injectable and Oral GS-441524 | 15 | None | |||
| 2 | 15 | Spayed Female | Burmese | None | Sweden | Effusive, non-effusive, neurological | Injectable GS-441524 | 12 | Less than 4 weeks | Injectable GS-441524 | 14 | 17 days | Oral GS-441524 | 5 weeks | None |
| 3 | 9 | Neutered Male | British Shorthair | None | Poland | Effusive, neurological, ocular | Injectable GS-441524 | 13 | Less than 2 weeks | Injectable GS-441524 | 12 | Longer than 6 months, less than 1 year | |||
| 4 | 5 | Neutered Male | Abyssinian | None | USA | Effusive | Injectable GS-441524 | 12 | Less than 2 weeks | Injectable GS-441524 | 14 | Less than 4 weeks | |||
| 5 | 4 | Spayed Female | Balinese Ragdoll mix | Calicivirus, conjunctivitis, giardiasis, ringworm, URI | USA | Non-effusive | Injectable GS-441524 | 13 | Less than 8 weeks | ||||||
| 6 | 7 | Spayed Female | Siamese | None | USA | Neurological | Injectable and oral GS-441524, injectable GC, injectable and oral molnupiravir | 12 | None | ||||||
| 7 | 7 | Neutered Male | American Shorthair | None | USA | Non-effusive | Injectable and Oral GS-441524 | 5 | None | ||||||
| 8 | 6 | Spayed Female | American Shorthair/Siamese mix | Ringworm, FCoV | USA | Effusive, neurological | Injectable and Oral GS-441524 | 5 | None | ||||||
| 9 | 4 | Spayed Female | Domestic mixed breed | History of fractured pelvis | USA | Effusive | Injectable and Oral GS-441524 | 14 | Less than 6 months | Oral GS-441524 | 13 | Less than 4 weeks | Oral GS-441524/injectable GC | 6 weeks in combination then 6 weeks of oral GS | None |
| 10 | 4 | Neutered Male | Domestic mixed breed | None | USA | Effusive | Injectable GS-441524 | 23 | Less than 4 weeks | ||||||
| 11 | 72 | Neutered Male | Domestic mixed breed | FeLV | USA | Non-effusive | Oral GS-441524 | 12 | Less than 6 months | ||||||
| 12 | 5 | Male | Domestic mixed breed | None | USA | Non-effusive, neurological, ocular | Injectable and oral GS-441524 | 17 | None | ||||||
| 13 | 1.5 | Male | Savannah | None | USA | Effusive, neurological | Injectable and oral GS-441524 | 24 | Less than 6 months | Injectable and Oral GS-441524 | 12 | Less than 4 weeks | |||
| 14 | 4 | Spayed Female | Domestic mixed breed | Skin and eye infections, fleas | poland | Non-effusive, neurological | Injectable GS-441524 | 12 | Less than 2 weeks | Injectable GS-441524 | 17 | Less than 4 weeks | |||
| 15 | 12 | Spayed Female | American Shorthair | None | USA | Effusive | Injectable GS-441524/GC | 1.5 | None | ||||||
| 16 | 5 | Spayed Female | Domestic mixed breed | None | USA | Effusive, neurological | Injectable GS-441524 | 12 | Less than 4 weeks | ||||||
| 17 | 4 | Male | American Longhair | None | USA | Ocular | Injectable and Oral GS-441524, GC376 | 13 | None | ||||||
| 18 | 6 | Neutered Male | Domestic mixed breed | None | USA | Effusive | Injectable GS-441524 | 12 | None | ||||||
| 19 | 12 | Neutered Male | Domestic mixed breed | None | USA | Non-effusive | Injectable and Oral GS-441524 | 12 | Less than 2 weeks | Injectable GS-441524 | 12 | None | |||
| 20 | 6 | Neutered Male | Unknown | None | USA | Non-effusive, neurological | Injectable GS-441524 | 4 | None | Oral GS-441524 | 3 | None | |||
| 21 | 4 | Spayed Female | Norwegian Forest Cat | None | USA | Neurological | Injectable GS-441524 | 12 | Less than 6 months | Injectable GS-441524 | 1.5 | None | Molnupiravir, GS-441524, GC | 12 weeks | None |
| 22 | 6 | Neutered Male | Domestic mixed breed | None | USA | Neurological, ocular | Oral GS-441524 | 3 | None | ||||||
| 23 | 12 | Spayed Female | Unknown breed | None | Germany | Neurological | Injectable GS-441524 | 16 | Less than 6 months | ||||||
| 24 | 3 | Male | Domestic mixed breed | None | USA | Neurological | Injectable GS-441524 | 12 | Less than 6 months | ||||||
| 25 | 6 | Neutered Male | American Shorthair | None | USA | Effusive | Oral GS-441524 | 13 | Less than 1 week | ||||||
| 26 | 1 | Male | Unknown breed | None | USA | Non-effusive | Injectable GS-441524 | 12 | Less than 1 week | ||||||
| 27 | 7 | Neutered Male | Domestic mixed breed | None | USA | Non-effusive, neurological | Molnupiravir | 12 | Less than 1 week | *Molnupiravir | |||||
| 28 | 24 | Spayed Female | Domestic mixed breed | None | USA | Effusive | Molnupiravir | ||||||||
| 29 | 12 | Spayed Female | Domestic mixed breed | None | USA | Non-effusive, ocular | Molnupiravir | ||||||||
| 30 | 24 | Neutered Male | Domestic mixed breed | None | USA | Neurological | Molnupiravir |
| Cat | Clinical Signs at Start of Treatment | Brand Name | Starting Dose and Frequency | Ending Dose and Frequency | Duration of Treatment (Weeks) | Time to Improvement | Persistent Clinical Signs | Outcome | Adverse Effects |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Diarrhea, vomiting | Aura Plus | 11 mg/kg twice a day | 11 mg/kg twice a day | 12 | Less than 1 week | None | Clinical Remission | None |
| 2 | None reported | Aura | 12 mg/kg twice a day | 12 mg/kg twice a day | 12 | Unsure | None | Clinical Remission | None |
| 3 | Anisocoria, color spots in the eye, polydypsia, pica, weight loss | Aura 2801 | 28 mg/kg twice a day | 14 mg/kg twice a day | 12 | Within 2 weeks | None | Clinical Remission | None |
| 4 | Anorexia, lethargy, weight loss | EIDD | 7 mg/kg twice a day | 7 mg/kg twice a day | 12 | Less than 1 week | None | Clinical Remission | None |
| 5 | Color spots in the eye, diarrhea, hiding and lack of socialization | Aura 2801 | 6 mg/kg once a day | 13 mg/kg once a day | 10 | Within 2 weeks | None | Clinical Remission | None |
| 6 | Anisocoria, constipation, anorexia, fecal and urinary incontinence, lethargy, paralysis, seizures, pale gums, weight loss | Aura 2801 | 20 mg/kg twice a day | 20 mg/kg twice a day | 11 | Less than 1 week | None | Clinical Remission | None |
| 7 | Anorexia, difficulty walking, hiding, lack of socialization, jaundice, lethargy | Capella EIDD | 9 mg/kg twice a day | 13 mg/kg twice a day | 10 | Less than 1 week | None | Clinical Remission | None |
| 8 | Anorexia, difficulty walking, urinary incontinence, paralysis | Aura 2801 | 17 mg/kg twice a day | 17 mg/kg twice a day | 15 | Less than 1 week | Difficulty walking persisted for 2 months, still not normal but has normal life | Clinical Remission | None |
| 9 | Cough, anorexia, hiding, lack of socialization, polydypsia, weight loss | Aura 2801 | 12 mg/kg twice a day | 16 mg/kg twice a day | 13 | Within 2 weeks | Polydypsia persisted for 1 week | Clinical Remission | None |
| 10 | Anorexia, lethargy, weight loss | Aura 2801 | 12 mg/kg twice a day | 12 mg/kg twice a day | 16 | Within 2 weeks | None | Clinical Remission | None |
| 11 | Anorexia, lethargy, URI, weight loss | Aura 1931 | 12 mg/kg twice a day | 12 mg/kg twice a day | 12 | Within 2 weeks | None | Clinical Remission | None |
| 12 | Blindness, head bobbing, difficulty walking | Aura 2801 | 10 mg/kg twice a day | 14 mg/kg twice a day | 12 | Within 3 weeks | None | Clinical Remission | None |
| 13 | Difficulty walking, hiding, lack of socialization, polyuria, lethargy, anorexia, paralysis, tremors | Aura 2801 | 12 mg/kg twice a day | 12 mg/kg twice a day | 12 | Less than 1 week | None | Clinical Remission | None |
| 14 | Anorexia, difficulty walking, hiding, lack of socialization, lethargy, unusually fearful | Aura 2801 | 11 mg/kg twice a day | 16 mg/kg twice a day | 18 | Greater than 4 weeks | Nothing physical but the MRI is still not normal | Clinical Remission | None |
| 15 | Blindness, constipation, anorexia, diarrhea, distended abdomen, hiding, lack of socialization, lethargy, pale gums, weight loss | Aura 2801 | 16 mg/kg twice a day | 16 mg/kg twice a day | 12 | Less than 1 week | None | Clinical Remission | None |
| 16 | Anorexia, difficulty walking, lethargy, seizures, tremors, weight loss | Aura 2801 | 14 mg/kg twice a day | 14 mg/kg twice a day | 12 | Less than 1 week | None | Clinical Remission | None |
| 17 | Cough, anorexia, difficulty breathing, hiding, lack of socialization, lethargy, vomiting, weight loss | Aura 2801 and Aura 1931 | 12 mg/kg twice a day | 17 mg/kg twice a day | 20 | Within 3 weeks | Anorexia | Clinical Remission | Nausea/vomiting, anorexia |
| 18 | Constipation, anorexia, difficulty walking, hiding, lack of socialization, weight loss | Aura 2801 | 12 mg/kg twice a day | 12 mg/kg twice a day | 8 | Within 2 weeks | None | Clinical Remission | None |
| 19 | Lethargy, anorexia | Aura 2801 | 12 mg/kg twice a day | 12 mg/kg twice a day | 7 | Within 2 weeks | None | Clinical Remission | None |
| 20 | Tremors/shaking | Aura 2801 | 10 mg/kg twice a day | 23 mg/kg two-three times per day | 10 | Less than 1 week | In remission for approximately 1 week before seizures started | Euthanized | Decreased appetite at three times per day dosing, severe leukopenia, losing whiskers, flaky skin on ears |
| 21 | Difficulty walking, fecal incontinence | Aura 2801 and Aura 1931 | 13 mg/kg twice a day | 30 mg/kg twice a day | 14 | Less than 1 week | Difficulty walking, difficulty jumping, fecal incontinence persisted at time of study (1 week post treatment) | Relapsed and Euthanized | Folded ear tips, muscle wasting |
| 22 | Color spots in the eye, anorexia, difficulty walking, hiding, lack of socialization, lethargy | Aura 2801 | 16 mg/kg twice a day | 19 mg/kg twice a day | 9 | Within 2 weeks | None | Clinical Remission | None |
| 23 | Difficulty walking, anorexia, loss of balance | Aura EIDD | 12 mg/kg twice a day | 15 mg/kg three times a day | 10 | Within 2 weeks | Difficulty walking | Clinical Remission | None |
| 24 | Blindness, color spots in the eyes, anorexia, difficulty breathing, difficulty walking, distended abdomen, urinary incontinence, jaundice, lethargy, paralysis, tremors | Aura 2801 | 15 mg/kg twice a day | 15 mg/kg twice a day | 16 | Less than 1 week | None | Clinical Remission | None |
| 25 | Difficulty breathing, difficulty walking, hiding, lack of socialization, lethargy, URI | Aura2801 | 7 mg/kg twice a day | 7 mg/kg twice a day | 16 | Within 2 weeks | None | Clinical Remission | None |
| 26 | Lethargy, anorexia | Aura 2801 | 14 mg/kg twice a day | 14 mg/kg twice a day | 15 | Less than 1 week | Neuological twitching, increased liver enzymes | Clinical Remission | None |
| Cat | Clinical Signs at Start of Treatment | Brand Name | Starting Dose and Frequency | Ending Dose and Frequency | Duration of Treatment (Weeks) | Time to Improvement | Persistent Clinical Signs | Outcome | Adverse Effects |
|---|---|---|---|---|---|---|---|---|---|
| * 27 | Hiding, lack of socialization, lethargy, anorexia, URI, vomiting, weight loss | Aura 2801 | 19 mg/kg twice a day | 19 mg/kg twice a day | 10 | Less than 1 week | None | Clinical Resmission | None |
| 28 | Anoreixa, difficulty walking, distended abdomen, hiding, lack of socialization, lethargy | Aura 2801 | 8 mg/kg twice a day | 8 mg/kg twice a day | 13 | Within two weeks | None | Clinical Resmission | None |
| 29 | Anisocoria, blindness, color changes in eyes, anorexia, hiding, lack of socialization, urinary incontinence, lethargy, | Aura 2801 | 10 mg/kg twice a day | 10 mg/kg twice a day | 13 | Within 2 weeks | None | Clinical Resmission | None |
| 30 | Hiding, lack of socialization, lethargy, pale gums, weight loss | Aura 2801 | 10 mg/kg twice a day | 12 mg/kg twice a day | 10 | Within two weeks | None | Clinical Resmission | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, M.; Jacque, N.; Novicoff, W.; Li, E.; Negash, R.; Evans, S.J.M. Unlicensed Molnupiravir is an Effective Rescue Treatment Following Failure of Unlicensed GS-441524-like Therapy for Cats with Suspected Feline Infectious Peritonitis. Pathogens 2022, 11, 1209. https://doi.org/10.3390/pathogens11101209
Roy M, Jacque N, Novicoff W, Li E, Negash R, Evans SJM. Unlicensed Molnupiravir is an Effective Rescue Treatment Following Failure of Unlicensed GS-441524-like Therapy for Cats with Suspected Feline Infectious Peritonitis. Pathogens. 2022; 11(10):1209. https://doi.org/10.3390/pathogens11101209
Chicago/Turabian StyleRoy, Meagan, Nicole Jacque, Wendy Novicoff, Emma Li, Rosa Negash, and Samantha J. M. Evans. 2022. "Unlicensed Molnupiravir is an Effective Rescue Treatment Following Failure of Unlicensed GS-441524-like Therapy for Cats with Suspected Feline Infectious Peritonitis" Pathogens 11, no. 10: 1209. https://doi.org/10.3390/pathogens11101209