
Identification of the Microbiome Associated with Prognosis in Patients with Chronic Liver Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approval, Registration, and Patient Enrollment
2.2. Sample Collection and Microbial DNA Analysis
2.3. Clinical Assessments
2.4. Statistical Analysis
2.5. Demographic and Clinical Characteristics
3. Results
3.1. Patient Background
3.2. Survival Curves and Causes of Death for All Patients
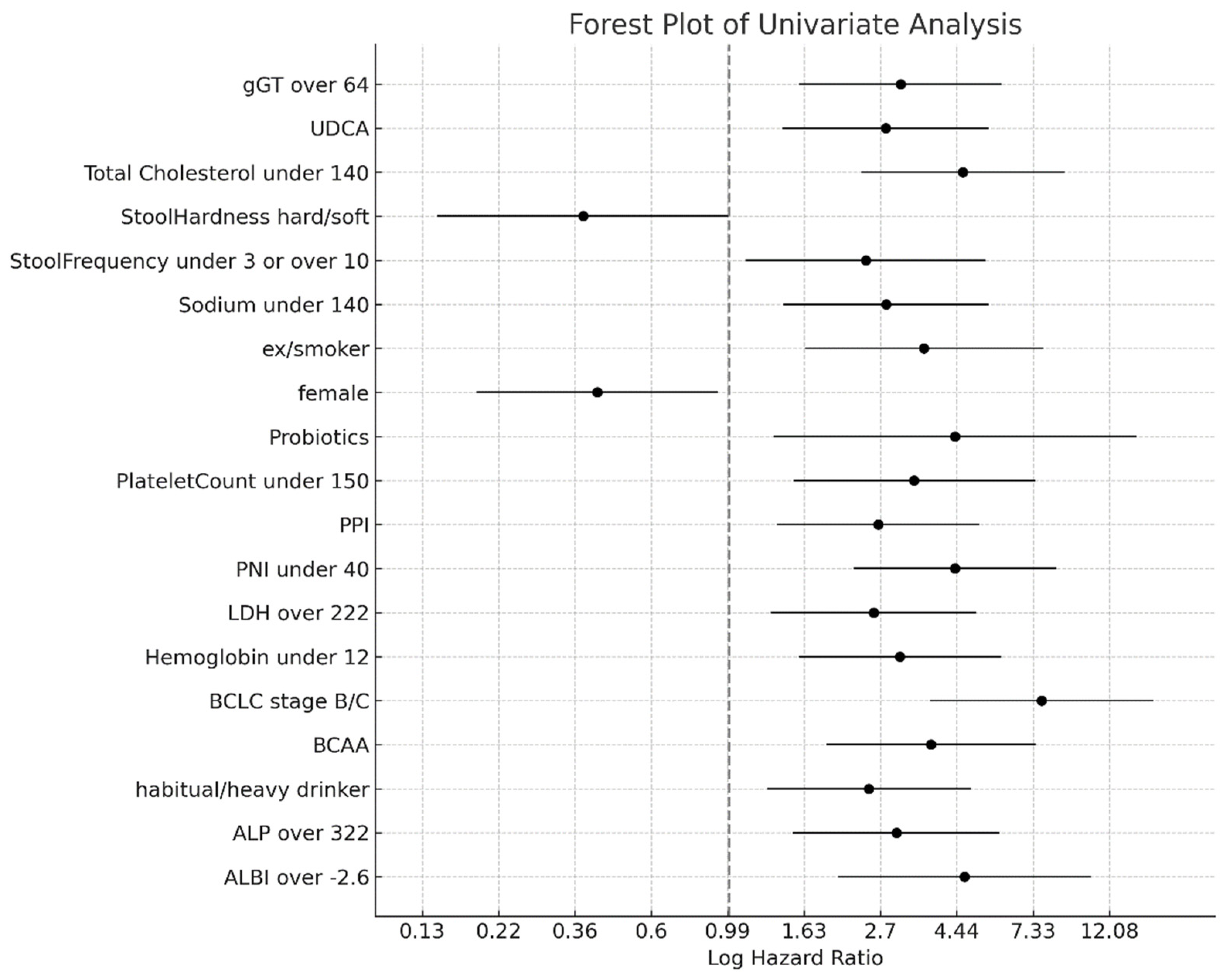
3.3. Clinical Factors Associated with Prognosis
3.4. Factors of Bacteria Associated with Prognosis
3.5. Integrated Analysis of Clinical and Microbiome Predictors of Survival
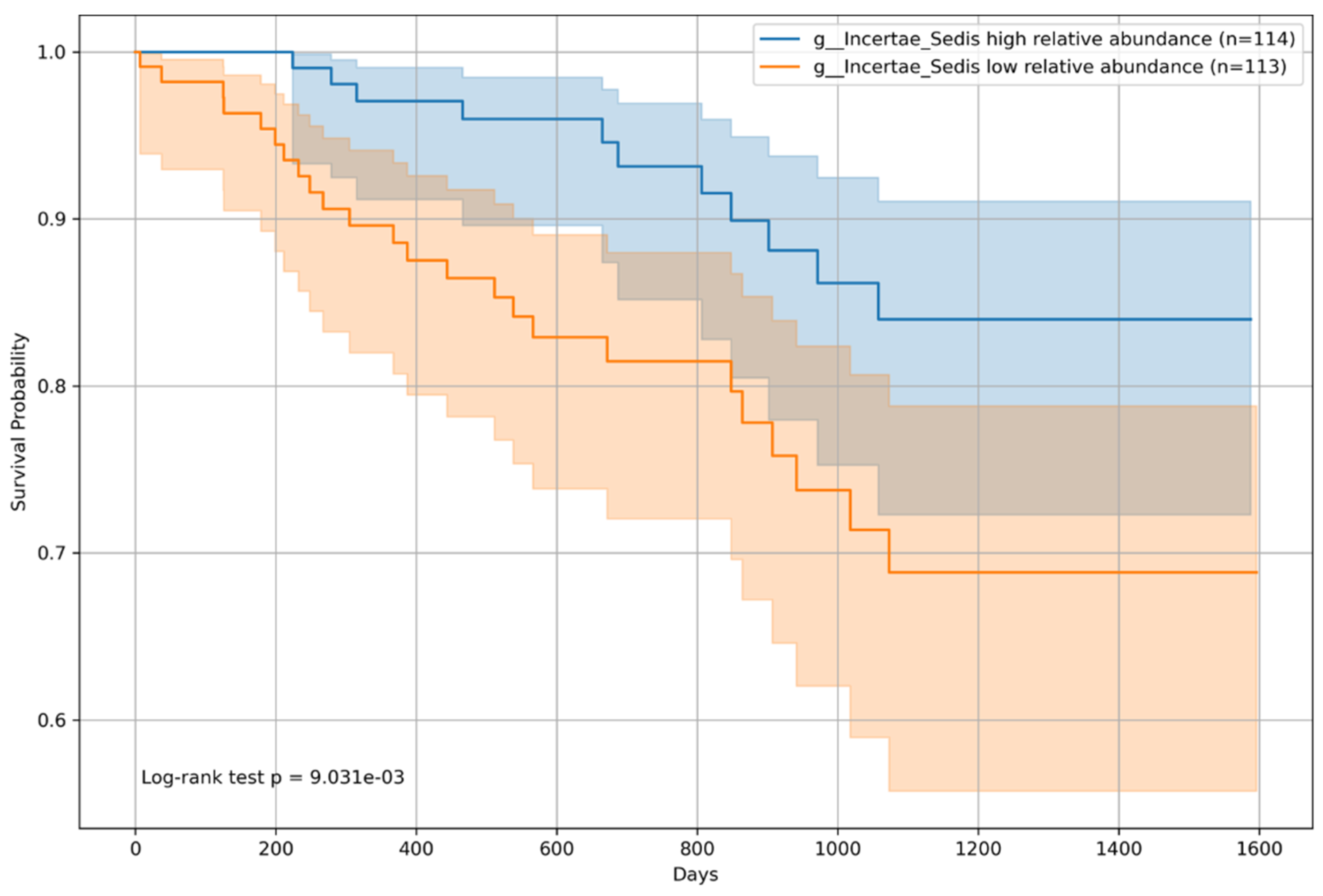
3.6. Overall Survival Analysis by Microbiome Relative Abundance
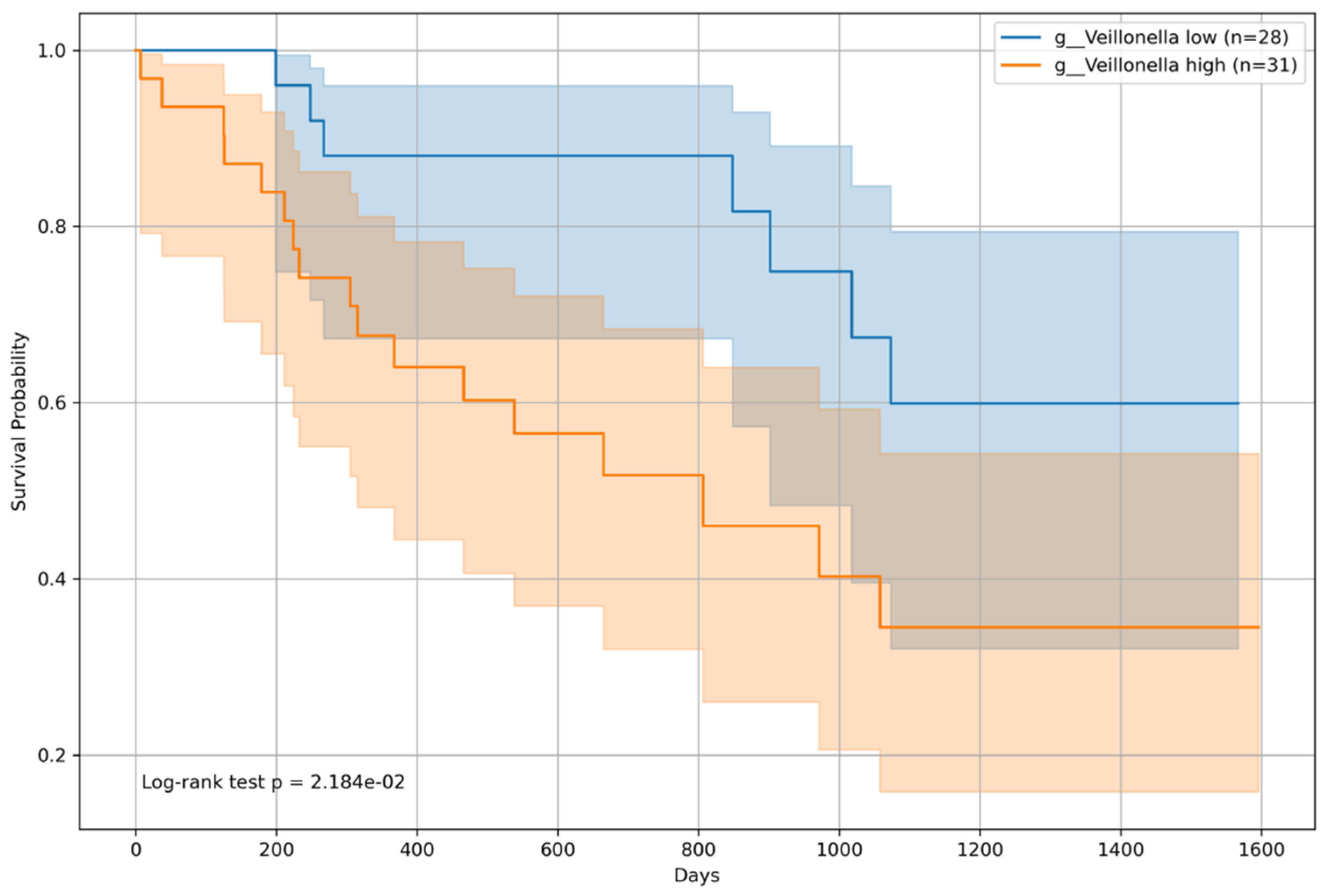
3.7. BCLC Stage-Specific Survival Impact
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 2021, 19, 55–71. [Google Scholar] [CrossRef]
- Tan, A.H.; Lim, S.Y.; Lang, A.E. The microbiome–gut–brain axis in Parkinson disease—From basic research to the clinic. Nat. Rev. Neurol. 2022, 18, 476–495. [Google Scholar] [CrossRef]
- Xu, Z.; Jiang, N.; Xiao, Y.; Yuan, K.; Wang, Z. The role of gut microbiota in liver regeneration. Front. Immunol. 2022, 13, 1003376. [Google Scholar] [CrossRef]
- Nakamoto, N.; Sasaki, N.; Aoki, R.; Miyamoto, K.; Suda, W.; Teratani, T.; Suzuki, T.; Koda, Y.; Chu, P.S.; Taniki, N.; et al. Gut pathobionts underlie intestinal barrier dysfunction and liver T helper 17 cell immune response in primary sclerosing cholangitis. Nat. Microbiol. 2019, 4, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Vargas, H.E.; Reddy, K.R.; Lai, J.C.; O’Leary, J.G.; Tandon, P.; Wong, F.; Mitrani, R.; White, M.B.; Kelly, M.; et al. Association between intestinal microbiota collected at hospital admission and outcomes of patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2019, 17, 756–765.e3. [Google Scholar] [CrossRef]
- Sung, C.M.; Lin, Y.F.; Chen, K.F.; Ke, H.M.; Huang, H.Y.; Gong, Y.N.; Tsai, W.S.; You, J.F.; Lu, M.J.; Cheng, H.T.; et al. Predicting clinical outcomes of cirrhosis patients with hepatic encephalopathy from the fecal microbiome. Cell Mol. Gastroenterol. Hepatol. 2019, 8, 301–318.e2. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Ishigami, M.; Honda, T.; Takeyama, T.; Ito, T.; Ishizu, Y.; Kuzuya, T.; Hayashi, K.; Goto, H.; Hirooka, Y. Influence of proton pump inhibitors on microbiota in chronic liver disease patients. Hepatol. Int. 2019, 13, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, Y.; Mizutani, S.; Nakajima, T.; Hosoda, F.; Watanabe, H.; Saito, Y.; Shibata, T.; Yachida, S.; Yamada, T. High stability of faecal microbiome composition in guanidine thiocyanate solution at room temperature and robustness during colonoscopy. Gut 2016, 65, 1574–1575. [Google Scholar] [CrossRef]
- Kawada, Y.; Naito, Y.; Andoh, A.; Ozeki, M.; Inoue, R. Effect of storage and DNA extraction method on 16S rRNA-profiled fecal microbiota in Japanese adults. J. Clin. Biochem. Nutr. 2019, 64, 106–111. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Kanda, T.; Goto, T.; Hirotsu, Y.; Moriyama, M.; Omata, M. Molecular mechanisms driving progression of liver cirrhosis towards hepatocellular carcinoma in chronic hepatitis B and C infections: A review. Int. J. Mol. Sci. 2019, 20, 1358. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Johnson, P.J. The ALBI score: From liver function in patients with HCC to a general measure of liver function. JHEP Rep. 2022, 4, 100557. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Feng, R.; Guo, X.; Kou, Y.; Xu, X.; Hong, C.; Zhang, W.; An, Y.; Philips, C.A.; Mancuso, A.; Qi, X. Association of lipid profile with decompensation, liver dysfunction, and mortality in patients with liver cirrhosis. Postgrad. Med. 2021, 133, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, I.; Vujovic, A.; Barac, A.; Djelic, M.; Korac, M.; Radovanovic Spurnic, A.; Gmizic, I.; Stevanovic, O.; Djordjevic, V.; Lekic, N.; et al. Gut-liver axis, gut microbiota, and its modulation in the management of liver diseases: A review of the literature. Int. J. Mol. Sci. 2019, 20, 395. [Google Scholar] [CrossRef]
- Xu, M.; Luo, K.; Li, J.; Li, Y.; Zhang, Y.; Yuan, Z.; Xu, Q.; Wu, X. Role of intestinal microbes in chronic liver diseases. Int. J. Mol. Sci. 2022, 23, 12661. [Google Scholar] [CrossRef]
- Xie, J.; Li, L.F.; Dai, T.Y.; Qi, X.; Wang, Y.; Zheng, T.Z.; Gao, X.Y.; Zhang, Y.J.; Ai, Y.; Ma, L.; et al. Short-chain fatty acids produced by Ruminococcaceae mediate α-linolenic acid promote intestinal stem cells proliferation. Mol. Nutr. Food Res. 2022, 66, e2100408. [Google Scholar] [CrossRef]
- Xie, Z.; Li, M.; Qian, M.; Yang, Z.; Han, X. Co-cultures of Lactobacillus acidophilus and Bacillus subtilis enhance mucosal barrier by modulating gut microbiota-derived short-chain fatty acids. Nutrients 2022, 14, 4475. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; White, M.B.; Monteith, P.; Noble, N.A.; Unser, A.B.; Daita, K.; Fisher, A.R.; et al. Altered profile of human gut microbiome is associated with cirrhosis and its complications. J. Hepatol. 2014, 60, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Takagi, T.; Inoue, R.; Oshima, A.; Sakazume, H.; Ogawa, K.; Tominaga, T.; Mihara, Y.; Sugaya, T.; Mizushima, K.; Uchiyama, K.; et al. Typing of the gut microbiota community in Japanese subjects. Microorganisms 2022, 10, 664. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Honda, T.; Ito, T.; Ishizu, Y.; Kuzuya, T.; Nakamura, M.; Miyahara, R.; Kawashima, H.; Ishigami, M.; Fujishiro, M. The relationship between oral-origin bacteria in the fecal microbiome and albumin–bilirubin grade in patients with hepatitis C. J. Gastroenterol. Hepatol. 2021, 36, 790–799. [Google Scholar] [CrossRef]
- Wu, Z.; Zhou, H.; Liu, D.; Deng, F. Alterations in the gut microbiota and the efficacy of adjuvant probiotic therapy in liver cirrhosis. Front. Cell Infect. Microbiol. 2023, 13, 1218552. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Years | 68 | (55–74) |
| Sex | Female | 87 | 38.30% |
| Male | 140 | 61.70% | |
| Survival Time | Days | 721 | (453–1125.5) |
| Etiology | Alcohol | 24 | 10.60% |
| HBV | 46 | 20.30% | |
| HCV | 131 | 57.70% | |
| NBNC | 26 | 11.50% | |
| Child–Pugh Class | A | 192 | 84.60% |
| B | 31 | 13.70% | |
| C | 4 | 1.80% | |
| BCLC | A | 55 | 25.20% |
| B | 43 | 19.70% | |
| C | 16 | 7.30% | |
| No HCC | 104 | 47.70% | |
| Diabetes | Yes | 68 | 30% |
| No | 159 | 70% | |
| Varices | Yes | 62 | 27.30% |
| No | 69 | 30.40% | |
| Unknown | 96 | 42.30% | |
| Lifestyle | |||
| Smoking | Ex-smoker | 43 | 26.10% |
| Nonsmoker | 98 | 59.40% | |
| Smoker | 24 | 14.50% | |
| Alcohol Consumption | Habitual | 34 | 15.20% |
| Heavy | 32 | 14.30% | |
| Non | 158 | 70.50% | |
| Exercise | Yes | 72 | 45.90% |
| No | 85 | 54.10% | |
| Main Diet | Fish | 85 | 53.80% |
| Meat | 73 | 46.20% | |
| Vegetables | Enough | 120 | 74.50% |
| Not enough | 41 | 25.50% | |
| Stool Hardness | Hard | 5 | 2.40% |
| Normal | 16 | 7.70% | |
| Soft | 188 | 90% | |
| Stool Frequency | Times/day | 7 | (5–7) |
| Medication | |||
| Proton Pump Inhibitors | Yes | 67 | 29.50% |
| No | 160 | 70.50% | |
| Probiotics | Yes | 7 | 3.10% |
| No | 220 | 96.90% | |
| Prednisolone | Yes | 4 | 1.80% |
| No | 223 | 98.20% | |
| Ursodeoxycholic acid | Yes | 77 | 33.90% |
| No | 150 | 66.10% | |
| Laxative | Yes | 31 | 13.70% |
| No | 196 | 86.30% | |
| Branched-Chain Amino Acid | Yes | 33 | 14.50% |
| No | 194 | 85.50% | |
| Blood Test | |||
| Total Protein | g/dL | 7.2 | (6.9–7.5) |
| Albumin | g/dL | 3.9 | (3.5–4.3) |
| Aspartate Aminotransferase | U/L | 32 | (22–50.5) |
| Alanine Aminotransferase | U/L | 28 | (17.5–48) |
| Alkaline Phosphatase | U/L | 271 | (221.5–377.5) |
| Gamma-Glutamyl Transferase | U/L | 36 | (23.5–73.5) |
| Cholinesterase | U/L | 270 | (188–323.5) |
| Total Bilirubin | mg/dL | 0.8 | (0.6–1.2) |
| Direct Bilirubin | mg/dL | 0.1 | (0.1–0.2) |
| Lactate Dehydrogenase | U/L | 198 | (174.5–233.5) |
| Amylase | U/L | 88 | (71.25–113) |
| Blood Urea Nitrogen | mg/dL | 14.95 | (12.6–18.1) |
| Creatinine | mg/dL | 0.76 | (0.61–0.92) |
| Estimated Glomerular Filtration Rate | mL/min/1.73 m3 | 71.8 | (61.35–86.02) |
| Uric Acid | mg/dL | 5.4 | (4.3–6.5) |
| Osmolarity | mOsm/kg | 282 | (278.25–284) |
| White Blood Cells | cells/μL | 4.8 | (3.9–5.85) |
| Red Blood Cells | cells/μL | 4.3 | (3.92–4.72) |
| Hematocrit | % | 39.7 | (36.2–42.95) |
| Hemoglobin | g/dL | 13.3 | (12.1–14.65) |
| Platelet Count | cells/μL | 155 | (106.5–207.5) |
| Sodium | mmol/L | 141 | (139–142) |
| Potassium | mmol/L | 4.2 | (4–4.4) |
| Total Calcium | mg/dL | 4.8 | (4.5–9.2) |
| Magnesium | mEq/L | 1.7 | (1.6–2) |
| Prothrombin Time | % | 95.8 | (84.05–103.45) |
| C-Reactive Protein | mg/L | 0.1 | (0.05–0.27) |
| Glucose | mg/dL | 102 | (91–123) |
| Total Cholesterol | mg/dL | 175 | (148–195.5) |
| Albumin-Bilirubin Index | −2.62 | (−2.86–2.19) | |
| Fibrosis-4 Index | 2.89 | (1.66–5.83) | |
| Prognostic Nutritional Index | 47 | (41.5–50.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, K.; Honda, T.; Inukai, Y.; Yokoyama, S.; Ito, T.; Imai, N.; Ishizu, Y.; Nakamura, M.; Kawashima, H. Identification of the Microbiome Associated with Prognosis in Patients with Chronic Liver Disease. Microorganisms 2024, 12, 610. https://doi.org/10.3390/microorganisms12030610
Yamamoto K, Honda T, Inukai Y, Yokoyama S, Ito T, Imai N, Ishizu Y, Nakamura M, Kawashima H. Identification of the Microbiome Associated with Prognosis in Patients with Chronic Liver Disease. Microorganisms. 2024; 12(3):610. https://doi.org/10.3390/microorganisms12030610
Chicago/Turabian StyleYamamoto, Kenta, Takashi Honda, Yosuke Inukai, Shinya Yokoyama, Takanori Ito, Norihiro Imai, Yoji Ishizu, Masanao Nakamura, and Hiroki Kawashima. 2024. "Identification of the Microbiome Associated with Prognosis in Patients with Chronic Liver Disease" Microorganisms 12, no. 3: 610. https://doi.org/10.3390/microorganisms12030610