Temporal Profiles and Dose-Responsiveness of Side Effects with Escitalopram and Duloxetine in Treatment-Naïve Depressed Adults


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Treatments
2.3. Assessment of Side Effects
2.4. Statistical Methods
3. Results
3.1. Participants
3.2. Side Effect Frequencies and Durations by Treatment
3.3. Time to Onset of Side Effects
3.4. Impact of Dose Changes on Side Effects
3.5. Impact of Side Effects on Treatment Outcomes
3.6. Impact of Depression Severity and Anxiety on Reported Side Effects
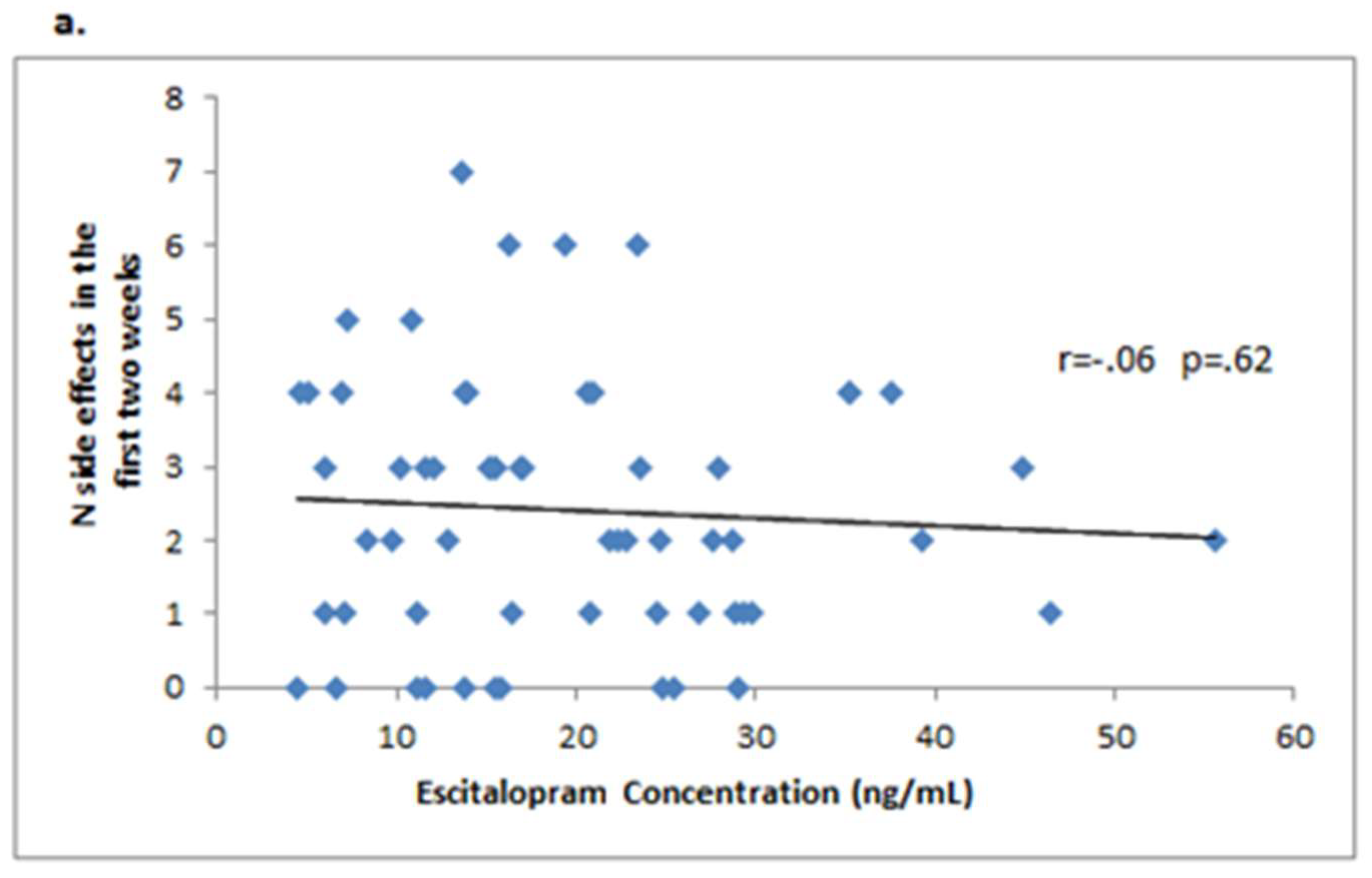
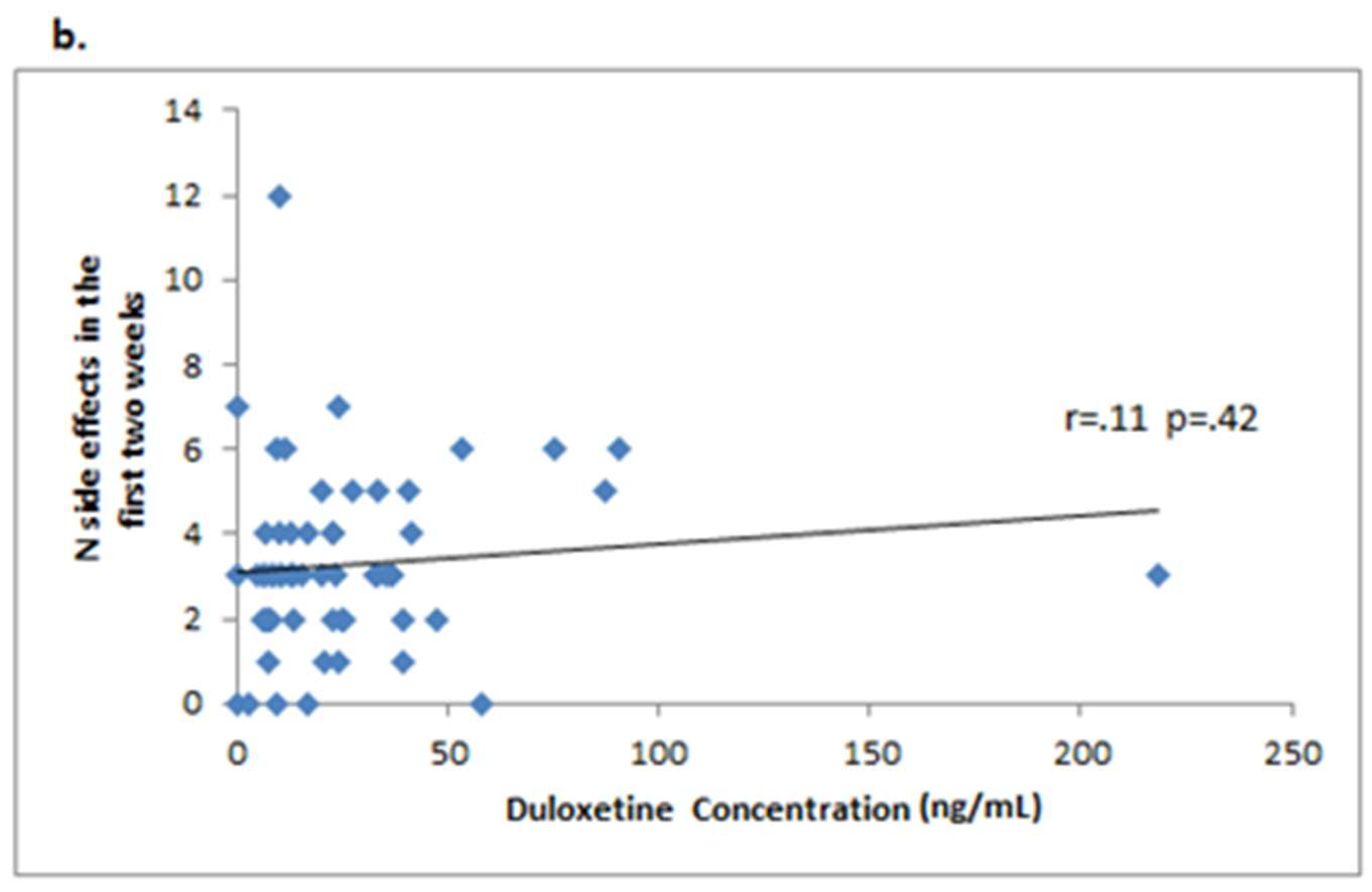
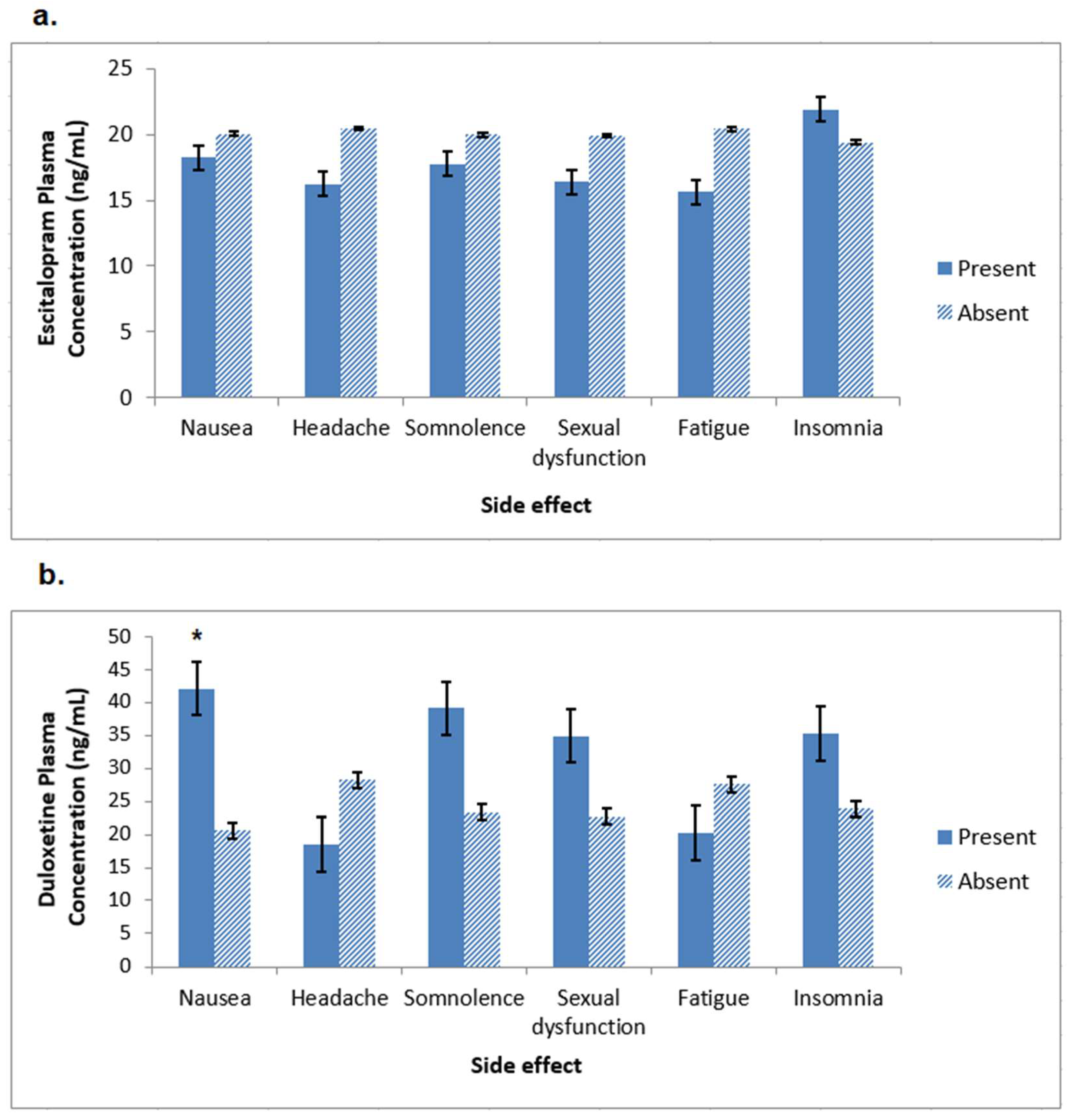
3.7. Relationship between Plasma Drug Concentration and Side Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kantor, E.D.; Rehm, C.D.; Haas, J.S.; Chan, A.T.; Giovannucci, E.L. Trends in prescription drug use among adults in the United States from 1999–2012. JAMA 2015, 314, 1818–1831. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Santilli, C.; Furukawa, T.A.; Signoretti, A.; Nakagawa, A.; McGuire, H.; Churchill, R.; Barbui, C. Escitalopram versus other antidepressive agents for depression. Cochrane Database Syst. Rev. 2009, 15, CD006532. [Google Scholar] [CrossRef] [PubMed]
- Demyttenaere, K.; Jaspers, L. Review: Bupropion and SSRI-induced side effects. J. Psychopharmacol. 2008, 22, 792–804. [Google Scholar] [CrossRef] [PubMed]
- Maddox, J.C.; Levi, M.; Thompson, C. The compliance with antidepressants in general practice. J. Psychopharmacol. 1994, 8, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Marcus, S.C.; Tedeschi, M.; Wan, G.J. Continuity of antidepressant treatment for adults with depression in the United States. Am. J. Psychiatry 2006, 163, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Moret, C.; Isaac, M.; Briley, M. Problems associated with long-term treatment with selective serotonin reuptake inhibitors. J. Psychopharmacol. 2009, 23, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Shen, Y.; Luo, J.; Li, H. Efficacy of escitalopram monotherapy in the treatment of major depressive disorder: A pooled analysis of 4 Chinese clinical trials. Medicine 2017, 96, e8142. [Google Scholar] [CrossRef] [PubMed]
- Auclair, A.L.; Martel, J.C.; Assié, M.B.; Bardin, L.; Heusler, P.; Cussac, D.; Marien, M.; Newman-Tancredi, A.; O’Connor, J.A.; Depoortère, R. Levomilnacipran (F2695), a norepinephrine-preferring SNRI: Profile in vitro and in models of depression and anxiety. Neuropharmacology 2013, 70, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Forest Laboratories, Inc. Lexapro [Package Insert]; Forest Laboratories, Inc.: St. Louis, MO, USA, 2004. [Google Scholar]
- Eli Lilly and Company. Cymbalta [Package Insert]; Eli Lilly and Company: Indianapolis, IN, UAS, 2004. [Google Scholar]
- Cipriani, A.; Koesters, M.; Furukawa, T.A.; Nosè, M.; Purgato, M.; Omori, I.M.; Trespidi, C.; Barbui, C. Duloxetine versus other anti-depressive agents for depression. Cochrane Database Syst. Rev. 2012, 17, CD006533. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Binder, E.B.; Cubells, J.F.; Goodman, M.M.; Kelley, M.E.; Kinkead, B.; Kutner, M.; Nemeroff, C.B.; Newport, D.J.; Owens, M.J.; et al. Predictors of remission in depression to individual and combined treatments (PReDICT): Study protocol for a randomized controlled trial. Trials 2012, 13, 106. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Kelley, M.E.; Aponte-Rivera, V.; Mletzko-Crowe, T.; Kinkead, B.; Ritchie, J.C.; Nemeroff, C.B.; Craighead, W.E.; Mayberg, H.S.; et al. Effects of patient preferences on outcomes in the Predictors of Remission in Depression to Individual and Combined Treatments (PReDICT) study. Am. J. Psychiatry 2017, 174, 546–556. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Edition (SCID-I/P, Version 2.0); New York State Psychiatric Institute: New York, NY, USA, 1995. [Google Scholar]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Uher, R.; Farmer, A.; Henigsberg, N.; Rietschel, M.; Mors, O.; Maier, W.; Kozel, D.; Hauser, J.; Souery, D.; Placentino, A.; et al. Adverse reactions to antidepressants. Br. J. Psychiatry 2009, 195, 202–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weitz, E.S.; Hollon, S.D.; Twisk, J.; van Straten, A.; Huibers, M.J.; David, D.; DeRubeis, R.J.; Dimidjian, S.; Dunlop, B.W.; Cristea, I.A.; et al. Baseline depression severity as moderator of depression outcomes between cognitive behavioral therapy vs pharmacotherapy: An individual patient data meta-analysis. JAMA Psychiatry 2015, 72, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Delgado, P.L. Approaches to the enhancement of patient adherence to antidepressant medication treatment. J. Clin. Psychiatry 2000, 61, 6–9. [Google Scholar] [PubMed]
- Bull, S.A.; Hu, X.H.; Hunkeler, E.M.; Lee, J.Y.; Ming, E.E.; Markson, L.E.; Fireman, B. Discontinuation of use and switching of antidepressants: Influence of patient-physician communication. JAMA 2002, 288, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, C.; Marsano, A.; Balestri, M.; De Ronchi, D.; Serretti, A. Clinical features and drug induced side effects in early versus late antidepressant responders. J. Psychiatr. Res. 2013, 47, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Brunton, S.; Wang, F.; Edwards, S.B.; Crucitti, A.S.; Ossanna, M.J.; Walker, D.J.; Robinson, M.J. Profile of adverse events with duloxetine treatment: A pooled analysis of placebo-controlled studies. Drug Saf. 2010, 33, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Bose, A.; Alexopoulos, G.S.; Gommoll, C.; Li, D.; Gandhi, C. Double-blind comparison of escitalopram and duloxetine in the acute treatment of major depressive disorder. Clin. Drug Investig. 2007, 27, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Greist, J.H.; Mallinckrodt, C.H.; Prakash, A.; Sambunaris, A.; Tollefson, G.D.; Wohlreich, M.M. Duloxetine versus escitalopram and placebo in the treatment of patients with major depressive disorder: Onset of antidepressant action, a non-inferiority study. Curr. Med. Res. Opin. 2007, 23, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.; Gembert, K.; Florea, I. A comparative study of the efficacy of acute and continuation treatment with escitalopram versus duloxetine in patients with major depressive disorder. Curr. Med. Res. Opin. 2007, 23, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Gruwez, B.; Gury, C.; Poirier, M.F.; Bouvet, O.; Gérard, A.; Bourdel, M.C.; Baylé, F.J.; Olié, J.P. Comparison of two assessment tools of antidepressant side-effects: UKU scale versus spontaneous notification. L’Encephale 2004, 30, 425–432. [Google Scholar] [CrossRef]
- Zimmerman, M.; Galione, J.N.; Attiullah, N.; Friedman, M.; Toba, C.; Boerescu, D.A.; Ragheb, M. Underrecognition of clinically significant side effects in depressed outpatients. J. Clin. Psychiatry 2010, 71, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Fava, M.; Rush, A.J.; Alpert, J.E.; Balasubramani, G.K.; Wisniewski, S.R.; Carmin, C.N.; Biggs, M.M.; Zisook, S.; Leuchter, A.; Howland, R.; et al. Difference in treatment outcome in outpatients with anxious versus nonanxious depression: A STAR*D report. Am. J. Psychiatry 2008, 165, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Gaspersz, R.; Lamers, F.; Kent, J.M.; Beekman, A.T.F.; Smit, J.H.; van Hemert, A.M.; Schoevers, R.A.; Penninx, B.W.J.H. Anxious distress predicts subsequent treatment outcome and side effects in depressed patients starting antidepressant treatment. J. Psychiatr. Res. 2017, 84, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Arias, B.; Crail-Meléndez, D.; López-Zapata, R.; Martínez-Juárez, I.E. Severity of anxiety and depression are related to a higher perception of adverse effects of antiepileptic drugs. Seizure 2012, 21, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Li, T.; Kornstein, S.G.; Friedman, E.S.; Rothschild, A.J.; Pedersen, R.; Ninan, P.; Keller, M.; Trivedi, M.H. Concordance between clinician and patient ratings as predictors of response, remission, and recurrence in major depressive disorder. J. Psychiatr. Res. 2011, 45, 96–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Linzer, M.; Hahn, S.R.; deGruy, F.V., 3rd; Brody, D. Physical symptoms in primary care: Predictors of psychiatric disorders and functional impairment. Arch. Fam. Med. 1994, 3, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Strigo, I.A.; Matthews, S.C.; Simmons, A.N. Decreased frontal regulation during pain anticipation in unmedicated subjects with major depressive disorder. Transl. Psychiatry 2013, 3, e239. [Google Scholar] [CrossRef] [PubMed]
- Ushinsky, A.; Reinhardt, L.E.; Simmons, A.N.; Strigo, I.A. Further evidence of emotional allodynia in unmedicated young adults with major depressive disorder. PLoS ONE 2013, 8, e80507. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Escitalopram (n = 105) | Duloxetine (n = 106) | F | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Age (yrs) | 41.1 | 12.1 | 38.2 | 11.4 | 3.904 | 0.049 |
| Age at first episode (yrs) | 32.8 | 15.1 | 27.7 | 13.4 | 6.850 | 0.010 |
| Current episode duration (wks) | 103.8 | 159.1 | 123.9 | 237.7 | 0.514 | 0.474 |
| HDRS | 20.0 | 3.6 | 19.4 | 3.8 | 1.766 | 0.185 |
| BDI | 23.3 | 7.2 | 23.3 | 7.3 | 0.000 | 0.998 |
| HAMA | 16.6 | 5.0 | 15.1 | 5.1 | 4.335 | 0.039 |
| N | % | N | % | X2 | P | |
| Sex | 0.379 | 0.538 | ||||
| Male | 49 | 46.7 | 45 | 42.5 | ||
| Female | 56 | 53.3 | 61 | 57.5 | ||
| Race | 1.892 | 0.864 | ||||
| White | 46 | 43.8 | 53 | 50.0 | ||
| Black | 22 | 21.0 | 20 | 18.9 | ||
| Other or Multiple | 37 | 35.2 | 33 | 31.1 | ||
| Ethnicity | 0.119 | 0.730 | ||||
| Hispanic | 33 | 31.4 | 31 | 29.2 | ||
| Non-Hispanic | 72 | 68.6 | 75 | 70.8 | ||
| Current Anxiety Disorder | 0.114 | 0.736 | ||||
| Yes | 45 | 42.9 | 43 | 40.6 | ||
| No | 60 | 57.1 | 63 | 59.4 | ||
| Previous Episodes | 2.717 | 0.257 | ||||
| 1 | 57 | 54.8 | 47 | 44.3 | ||
| 2 | 17 | 16.3 | 25 | 23.6 | ||
| ≥3 | 30 | 28.8 | 34 | 32.1 | ||
| Chronic Episode (≥2 yrs) | 29 | 28.2 | 34 | 32.4 | 0.440 | 0.507 |
| Adverse Event | Frequency | Duration | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Escitalopram | Duloxetine | p-Value | Escitalopram | Duloxetine | p-Value | ||||||
| (n = 211) | (n = 105) | (n = 106) | (n = 92) | (n = 96) | ||||||||
| n | % | n | % | n | % | Mean (Days) | SD | Mean (days) | SD | |||
| Nausea | 58 | 27.5 | 26 | 24.8 | 32 | 30.2 | 0.38 | 7.7 | 8.5 | 17.6 | 36.0 | 0.20 |
| Headache | 53 | 25.1 | 27 | 25.7 | 26 | 24.5 | 0.84 | 20.8 | 22.7 | 12.7 | 17.4 | 0.19 |
| Somnolence | 48 | 22.7 | 23 | 21.9 | 25 | 23.6 | 0.77 | 44.0 | 63.3 | 19.2 | 17.2 | 0.08 |
| Sexual dysfunction | 47 | 22.3 | 23 | 21.9 | 24 | 22.6 | 0.90 | 89.0 | 93.7 | 88.5 | 70.0 | 0.98 |
| Fatigue | 46 | 21.8 | 22 | 21 | 24 | 22.6 | 0.77 | 49.1 | 55.2 | 31.4 | 32.5 | 0.22 |
| Insomnia | 45 | 21.3 | 20 | 19 | 25 | 23.6 | 0.42 | 71.5 | 116.4 | 37.2 | 37.3 | 0.20 |
| Dry mouth | 41 | 19.4 | 16 | 15.2 | 25 | 23.6 | 0.13 | 54.4 | 62.9 | 72.3 | 73.4 | 0.43 |
| Dizziness | 33 | 15.6 | 16 | 15.2 | 17 | 16 | 0.87 | 38.9 | 78.4 | 10.3 | 11.4 | 0.19 |
| Diarrhea | 32 | 15.2 | 15 | 14.3 | 17 | 16 | 0.72 | 21.0 | 34.6 | 13.4 | 22.3 | 0.48 |
| Constipation | 20 | 9.5 | 8 | 7.6 | 12 | 11.3 | 0.36 | 24.6 | 30.0 | 27.2 | 22.6 | 0.83 |
| Anxiety | 18 | 8.5 | 8 | 7.6 | 10 | 9.4 | 0.64 | 15.8 | 18.3 | 15.4 | 16.9 | 0.97 |
| Abdominal pain | 17 | 8.1 | 6 | 5.7 | 11 | 10.4 | 0.21 | 12.6 | 15.1 | 9.6 | 9.6 | 0.64 |
| Yawning | 16 | 7.6 | 7 | 6.7 | 9 | 8.5 | 0.62 | 31.6 | 16.5 | 45.0 | 59.9 | 0.58 |
| Appetite decreased | 16 | 7.6 | 7 | 6.7 | 9 | 8.5 | 0.62 | 20.2 | 15.6 | 50.0 | 53.2 | 0.22 |
| Emotional blunting | 15 | 7.1 | 11 | 10.5 | 4 | 3.8 | 0.06 | 38.0 | 24.4 | 24.8 | 24.8 | 0.38 |
| Dyspepsia | 14 | 6.6 | 6 | 5.7 | 8 | 7.5 | 0.59 | 33.8 | 42.1 | 13.8 | 11.8 | 0.34 |
| Bruxism | 14 | 6.6 | 8 | 7.6 | 6 | 5.7 | 0.57 | 88.6 | 85.6 | 54.0 | 41.6 | 0.38 |
| Sweating increased | 13 | 6.2 | 4 | 3.8 | 9 | 8.5 | 0.16 | 41.3 | 23.4 | 41.3 | 37.1 | 0.99 |
| Jitteriness | 12 | 5.7 | 6 | 5.7 | 6 | 5.7 | 0.99 | 10.3 | 5.1 | 5.8 | 5.9 | 0.28 |
| Restlessness | 11 | 5.2 | 5 | 4.8 | 6 | 5.7 | 0.77 | 18.3 | 24.5 | 19.3 | 14.7 | 0.95 |
| Side Effect | All Patients | Escitalopram | Duloxetine | p-Value | |||
|---|---|---|---|---|---|---|---|
| (n = 793) | (n = 372) | (n = 421) | |||||
| Mean | SD | Mean | SD | Mean | SD | ||
| Dry mouth | 5.1 | 7.8 | 5.0 | 6.4 | 5.2 | 8.6 | 0.93 |
| Dyspepsia | 6.6 | 10.6 | 5.0 | 7.8 | 7.9 | 12.8 | 0.64 |
| Appetite decreased | 6.7 | 14.2 | 5.7 | 9.7 | 7.3 | 17.2 | 0.83 |
| Jitteriness | 8.6 | 13.3 | 12.0 | 15.9 | 5.1 | 10.1 | 0.36 |
| Yawning | 9.8 | 13.7 | 10.6 | 13.5 | 9.1 | 14.5 | 0.82 |
| Nausea | 10.1 | 17.6 | 10.1 | 14.7 | 10.1 | 20.0 | 0.99 |
| Restlessness | 10.8 | 14.3 | 10.8 | 14.6 | 10.7 | 15.4 | 0.99 |
| Diarrhea | 12.1 | 18.3 | 13.3 | 15.4 | 11.2 | 20.7 | 0.75 |
| Fatigue | 12.6 | 18.2 | 13.2 | 17.6 | 12.1 | 19.1 | 0.83 |
| Anxiety | 12.6 | 19.3 | 16.4 | 21.3 | 9.2 | 17.7 | 0.43 |
| Abdominal pain | 13.3 | 12.8 | 13.5 | 13.3 | 13.2 | 13.1 | 0.96 |
| Headache | 13.8 | 18.2 | 15.2 | 18.0 | 12.1 | 18.5 | 0.49 |
| Constipation | 14.3 | 14.7 | 17.3 | 17.7 | 12.3 | 12.6 | 0.43 |
| Insomnia | 14.8 | 16.8 | 15.3 | 16.3 | 14.4 | 17.6 | 0.86 |
| Dizziness | 15.6 | 19.5 | 12.6 | 15.2 | 18.6 | 23.1 | 0.35 |
| Somnolence | 15.6 | 19.2 | 19.2 | 20.4 | 12.2 | 17.7 | 0.19 |
| Sweating increased | 19.0 | 15.9 | 13.3 | 12.3 | 21.6 | 17.3 | 0.41 |
| Bruxism | 19.9 | 19.8 | 20.2 | 19.7 | 19.6 | 21.5 | 0.95 |
| Sexual dysfunction | 20.9 | 21.1 | 25.5 | 21.5 | 16.7 | 20.1 | 0.11 |
| Emotional blunting | 23.5 | 18.0 | 20.9 | 15.2 | 30.5 | 25.6 | 0.38 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polychroniou, P.E.; Mayberg, H.S.; Craighead, W.E.; Rakofsky, J.J.; Aponte Rivera, V.; Haroon, E.; Dunlop, B.W. Temporal Profiles and Dose-Responsiveness of Side Effects with Escitalopram and Duloxetine in Treatment-Naïve Depressed Adults. Behav. Sci. 2018, 8, 64. https://doi.org/10.3390/bs8070064
Polychroniou PE, Mayberg HS, Craighead WE, Rakofsky JJ, Aponte Rivera V, Haroon E, Dunlop BW. Temporal Profiles and Dose-Responsiveness of Side Effects with Escitalopram and Duloxetine in Treatment-Naïve Depressed Adults. Behavioral Sciences. 2018; 8(7):64. https://doi.org/10.3390/bs8070064
Chicago/Turabian StylePolychroniou, Philip E., Helen S. Mayberg, W. Edward Craighead, Jeffrey J. Rakofsky, Vivianne Aponte Rivera, Ebrahim Haroon, and Boadie W. Dunlop. 2018. "Temporal Profiles and Dose-Responsiveness of Side Effects with Escitalopram and Duloxetine in Treatment-Naïve Depressed Adults" Behavioral Sciences 8, no. 7: 64. https://doi.org/10.3390/bs8070064