

Correlating Quantitative and Genomic SARS-CoV-2 Wastewater Data with Clinical Metrics in Metropolitan Perth, Western Australia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Wastewater Sample Collection
2.2. Wastewater Concentration and Extraction
2.3. SARS-CoV-2 Real-Time PCR
2.4. Molecular Inhibition Assessment
2.5. Wastewater SARS-CoV-2 Viral Quantification
2.6. SARS-CoV-2 Genome Sequencing
2.7. Clinical Data
2.8. Data Processing, Correlation and Statistical Significance
3. Results
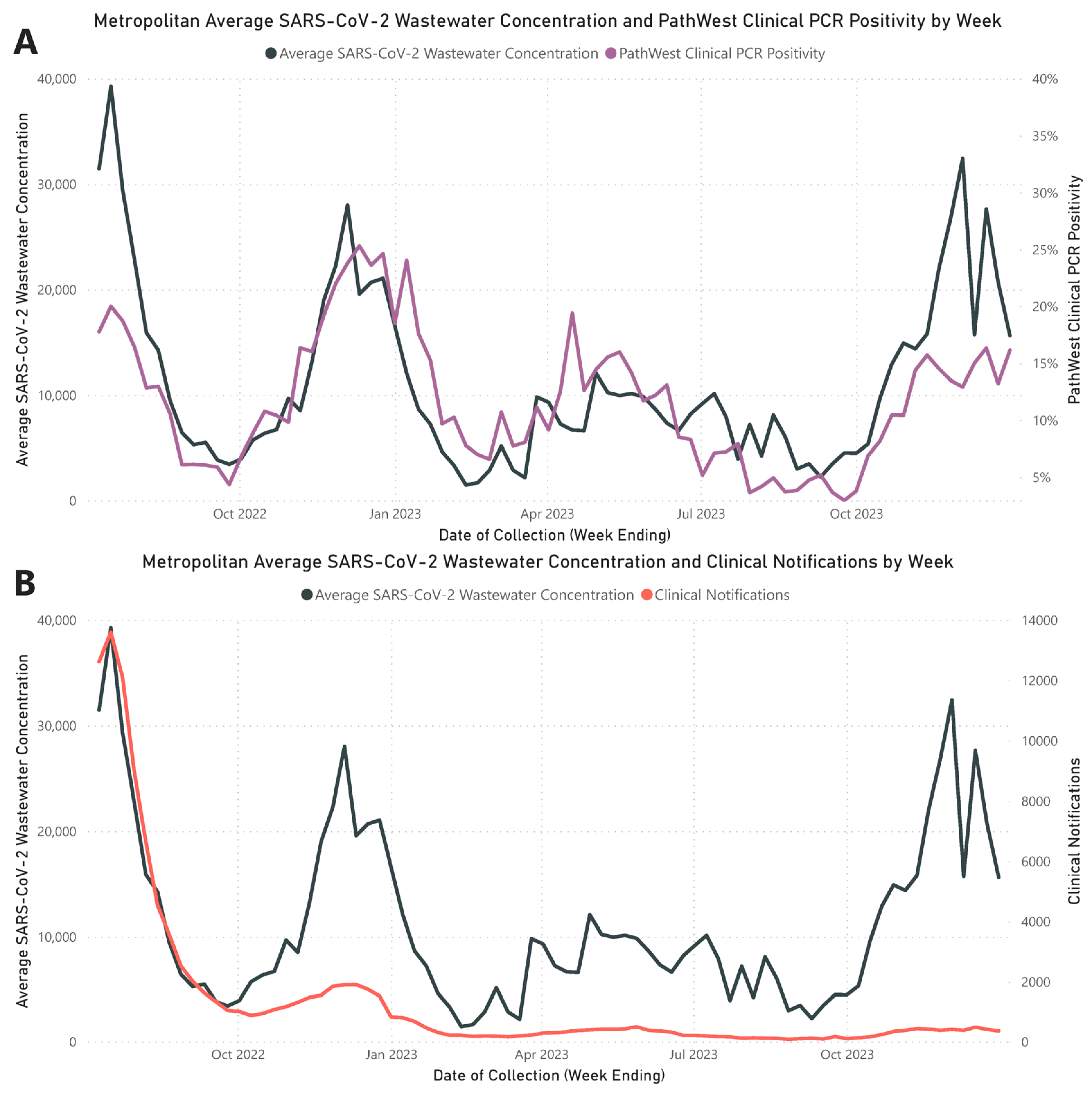
3.1. Quantitative Correlation of Respiratory Clinical Metrics to Wastewater Concentrations
3.2. SARS-CoV-2 Wastewater Genomic Coverage and Correlation to Quantitation
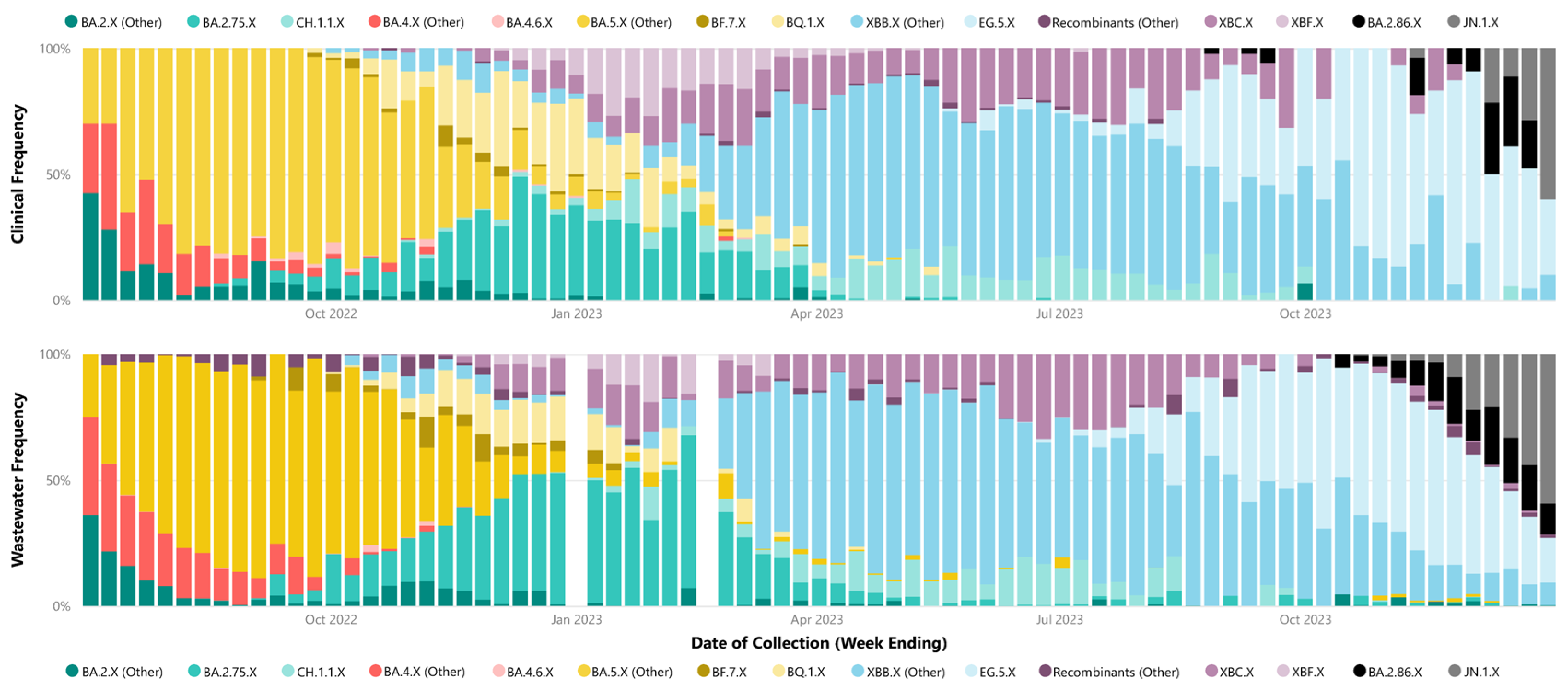
3.3. SARS-CoV-2 Relative Lineage Abundance Correlation
3.4. Initial Detection of Lineage Groups—Wastewater vs. Clinical
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Environmental Surveillance for SARS-CoV-2 to Complement Other Public Health Surveillance; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- Galanti, M.; Comito, D.; Ligon, C.; Lane, B.; Matienzo, N.; Ibrahim, S.; Shittu, A.; Tagne, E.; Birger, R.; Ud-Dean, M.; et al. Active surveillance documents rates of clinical care seeking due to respiratory illness. Influenza Other Respir. Viruses 2020, 14, 499–506. [Google Scholar] [CrossRef]
- Bonačić Marinović, A.; Swaan, C.; van Steenbergen, J.; Kretzschmar, M. Quantifying reporting timeliness to improve outbreak control. Emerg. Infect. Dis. 2015, 21, 209–216. [Google Scholar] [CrossRef]
- Kretzschmar, M.E.; Rozhnova, G.; Bootsma, M.C.J.; van Boven, M.; van de Wijgert, J.H.H.M.; Bonten, M.J.M. Impact of delays on effectiveness of contact tracing strategies for COVID-19: A modelling study. Lancet Public Health 2020, 5, e452–e459. [Google Scholar] [CrossRef] [PubMed]
- Australian Government COVID-19 Rapid Antigen Tests: Guidance on Performance Requirements and Risk Mitigation Strategies; Version 3.0; Department of Health and Aged Care—Therapeutic Goods Administration: Canberra, Australia, 2023.
- Lodder, W.; de Roda Husman, A.M. SARS-CoV-2 in wastewater: Potential health risk, but also data source. Lancet Gastroenterol. Hepatol. 2020, 5, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Roguet, A.; McClary-Gutierrez, J.S.; Newton, R.J.; Kloczko, N.; Meiman, J.G.; McLellan, S.L. Evaluation of Sampling, Analysis, and Normalization Methods for SARS-CoV-2 Concentrations in Wastewater to Assess COVID-19 Burdens in Wisconsin Communities. ACS EST Water 2021, 1, 1955–1965. [Google Scholar] [CrossRef]
- Weidhaas, J.; Aanderud, Z.T.; Roper, D.K.; VanDerslice, J.; Gaddis, E.B.; Ostermiller, J.; Hoffman, K.; Jamal, R.; Heck, P.; Zhang, Y.; et al. Correlation of SARS-CoV-2 RNA in wastewater with COVID-19 disease burden in sewersheds. Sci. Total Environ. 2021, 775, 145790. [Google Scholar] [CrossRef] [PubMed]
- Bagutti, C.; Alt Hug, M.; Heim, P.; Maurer Pekerman, L.; Ilg Hampe, E.; Hübner, P.; Fuchs, S.; Savic, M.; Stadler, T.; Topolsky, I.; et al. Wastewater monitoring of SARS-CoV-2 shows high correlation with COVID-19 case numbers and allowed early detection of the first confirmed B.1.1.529 infection in Switzerland: Results of an observational surveillance study. Swiss Med. Wkly. 2022, 152, w30202. [Google Scholar] [CrossRef]
- Boehm, A.B.; Hughes, B.; Duong, D.; Chan-Herur, V.; Buchman, A.; Wolfe, M.K.; White, B.J. Wastewater concentrations of human influenza, metapneumovirus, parainfluenza, respiratory syncytial virus, rhinovirus, and seasonal coronavirus nucleic-acids during the COVID-19 pandemic: A surveillance study. Lancet Microbe 2023, 4, e340–e348. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.; Duong, D.; White, B.J.; Wigginton, K.R.; Chan, E.M.G.; Wolfe, M.K.; Boehm, A.B. Respiratory Syncytial Virus (RSV) RNA in Wastewater Settled Solids Reflects RSV Clinical Positivity Rates. Environ. Sci. Technol. Lett. 2022, 9, 173–178. [Google Scholar] [CrossRef]
- de Melo, T.; Islam, G.; Simmons, D.B.D.; Desaulniers, J.P.; Kirkwood, A.E. An alternative method for monitoring and interpreting influenza A in communities using wastewater surveillance. Front. Public Health 2023, 11, 1141136. [Google Scholar] [CrossRef]
- Assoum, M.; Lau, C.L.; Thai, P.K.; Ahmed, W.; Mueller, J.F.; Thomas, K.V.; Choi, P.M.; Jackson, G.; Selvey, L.A. Wastewater Surveillance Can Function as an Early Warning System for COVID-19 in Low-Incidence Settings. Trop. Med. Infect. Dis. 2023, 8, 211. [Google Scholar] [CrossRef]
- Li, X.; Liu, H.; Gao, L.; Sherchan, S.P.; Zhou, T.; Khan, S.J.; van Loosdrecht, M.C.M.; Wang, Q. Wastewater-based epidemiology predicts COVID-19-induced weekly new hospital admissions in over 150 USA counties. Nat. Commun. 2023, 14, 4548. [Google Scholar] [CrossRef]
- Shaw, A.G.; Mampuela, T.K.; Lofiko, E.L.; Pratt, C.; Troman, C.; Bujaki, E.; O’Toole, Á.; Akello, J.O.; Aziza, A.A.; Lusamaki, E.K.; et al. Sensitive poliovirus detection using nested PCR and nanopore sequencing: A prospective validation study. Nat. Microbiol. 2023, 8, 1634–1640. [Google Scholar] [CrossRef]
- Karthikeyan, S.; Levy, J.I.; De Hoff, P.; Humphrey, G.; Birmingham, A.; Jepsen, K.; Farmer, S.; Tubb, H.M.; Valles, T.; Tribelhorn, C.E.; et al. Wastewater sequencing reveals early cryptic SARS-CoV-2 variant transmission. Nature 2022, 609, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Liao, S.; Ezekiel, M.; Novak, N.; Rossi, A.; LaCross, N.; Oakeson, K.; Rohrwasser, A. Wastewater Genomic Surveillance Captures Early Detection of Omicron in Utah. Microbiol. Spectr. 2023, 11, e0039123. [Google Scholar] [CrossRef] [PubMed]
- Yousif, M.; Rachida, S.; Taukobong, S.; Ndlovu, N.; Iwu-Jaja, C.; Howard, W.; Moonsamy, S.; Mhlambi, N.; Gwala, S.; Levy, J.I.; et al. SARS-CoV-2 genomic surveillance in wastewater as a model for monitoring evolution of endemic viruses. Nat. Commun. 2023, 14, 6325. [Google Scholar] [CrossRef]
- Li, L.; Uppal, T.; Hartley, P.D.; Gorzalski, A.; Pandori, M.; Picker, M.A.; Verma, S.C.; Pagilla, K. Detecting SARS-CoV-2 variants in wastewater and their correlation with circulating variants in the communities. Sci. Rep. 2022, 12, 16141. [Google Scholar] [CrossRef]
- Kaya, D.; Falender, R.; Radniecki, T.; Geniza, M.; Cieslak, P.; Kelly, C.; Lininger, N.; Sutton, M. Correlation between Clinical and Wastewater SARS-CoV-2 Genomic Surveillance, Oregon, USA. Emerg. Infect. Dis. 2022, 28, 1906–1908. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Institute of Public Health. Weekly Reports on COVID-19, Inflenza and Other Respiratory Viruses. Available online: https://www.fhi.no/publ/statusrapporter/luftveisinfeksjoner/ (accessed on 25 February 2024).
- Centre for Disease Control & Prevention USA. COVID-19 Variants in Wastewater. Available online: https://www.cdc.gov/nwss/rv/COVID19-variants.html (accessed on 26 February 2024).
- COVID-19 Wastewater Surveillance [Internet]. 2024. Available online: https://www.health.wa.gov.au/articles/a_e/coronavirus/covid19-wastewater-surveillance (accessed on 25 February 2024).
- Rajput, V.; Pramanik, R.; Malik, V.; Yadav, R.; Samson, R.; Kadam, P.; Bhalerao, U.; Tupekar, M.; Deshpande, D.; Shah, P.; et al. Genomic surveillance reveals early detection and transition of delta to omicron lineages of SARS-CoV-2 variants in wastewater treatment plants of Pune, India. Environ. Sci. Pollut. Res. 2023, 30, 118976–118988. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Greater Perth, 2021 Census All Persons QuickStats; 2021. Available online: https://abs.gov.au/census/find-census-data/quickstats/2021/5GPER (accessed on 25 February 2024).
- Levy, A.; Gazeley, J.; Lee, T.; Jardine, A.; Gordon, C.; Cooper, N.; Theobald, R.; Huppatz, C.; Sjollema, S.; Hodge, M.; et al. Whole genome sequencing of SARS-CoV-2 from wastewater links to individual cases in catchments. Sci. Total Environ. 2022, 851, 158266. [Google Scholar] [CrossRef]
- Water Research Australia. ColoSSoS|Method Evaluation and Optimisation: Investigation of PCR-Based Methods and Feasibility Study for Whole-Genome Sequencing. 2021. Available online: https://www.waterra.com.au/project/colossos-method-evaluation-and-optimisation-investigation-of-pcr-based-methods-and-feasibility-study-for-whole-genome-sequencing/ (accessed on 18 March 2024).
- Suo, T.; Liu, X.; Feng, J.; Guo, M.; Hu, W.; Guo, D.; Ullah, H.; Yang, Y.; Zhang, Q.; Wang, X.; et al. ddPCR: A more accurate tool for SARS-CoV-2 detection in low viral load specimens. Emerg. Microbes Infect. 2020, 9, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; du Plessis, L.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2020, 5, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Government of Western Australia. Public Health Act; 2016. Available online: https://www.legislation.wa.gov.au/legislation/statutes.nsf/main_mrtitle_13791_homepage.html (accessed on 25 February 2024).
- Government of Western Australia. Emergency Management Act; 2005. Available online: https://www.legislation.wa.gov.au/legislation/statutes.nsf/main_mrtitle_294_homepage.html (accessed on 25 February 2024).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Elsevier Science: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Shah, S.; Gwee, S.X.W.; Ng, J.Q.X.; Lau, N.; Koh, J.; Pang, J. Wastewater surveillance to infer COVID-19 transmission: A systematic review. Sci. Total Environ. 2022, 804, 150060. [Google Scholar] [CrossRef]
- Government of Western Australia—Department of Health. COVID-19 Weekly Surveillance Report 1–7 January 2024. Available online: https://www.health.wa.gov.au/Articles/F_I/Infectious-disease-data/COVID19-Weekly-Surveillance-Report (accessed on 25 February 2024).
- Department of Health—Government of Western Australia. Free RAT Program Ends. Available online: https://www.healthywa.wa.gov.au/News/2023/Free-RAT-program-ends (accessed on 25 February 2024).
- Government of Western Australia. Announcements—Western Australian Government News Stories, Media Releases and Community Updates. Available online: https://www.wa.gov.au/government/announcements (accessed on 25 February 2024).
- Allen, D.M.; Reyne, M.I.; Allingham, P.; Levickas, A.; Bell, S.H.; Lock, J.; Coey, J.D.; Carson, S.; Lee, A.J.; McSparron, C.; et al. Genomic Analysis and Surveillance of Respiratory Syncytial Virus (RSV) Using Wastewater-Based Epidemiology (WBE). medRxiv 2023, 2023, 23293016. [Google Scholar] [CrossRef]
- Vo, V.; Harrington, A.; Chang, C.L.; Baker, H.; Moshi, M.A.; Ghani, N.; Itorralba, J.Y.; Tillett, R.L.; Dahlmann, E.; Basazinew, N.; et al. Identification and genome sequencing of an influenza H3N2 variant in wastewater from elementary schools during a surge of influenza A cases in Las Vegas, Nevada. Sci. Total Environ. 2023, 872, 162058. [Google Scholar] [CrossRef]
- Tisza, M.; Javornik Cregeen, S.; Avadhanula, V.; Zhang, P.; Ayvaz, T.; Feliz, K.; Hoffman, K.L.; Clark, J.R.; Terwilliger, A.; Ross, M.C.; et al. Wastewater sequencing reveals community and variant dynamics of the collective human virome. Nat. Commun. 2023, 14, 6878. [Google Scholar] [CrossRef] [PubMed]
- Berno, G.; Fabeni, L.; Matusali, G.; Gruber, C.E.M.; Rueca, M.; Giombini, E.; Garbuglia, A.R. SARS-CoV-2 Variants Identification: Overview of Molecular Existing Methods. Pathogens 2022, 11, 1058. [Google Scholar] [CrossRef]
- Goswami, C.; Sheldon, M.; Bixby, C.; Keddache, M.; Bogdanowicz, A.; Wang, Y.; Schultz, J.; McDevitt, J.; LaPorta, J.; Kwon, E.; et al. Identification of SARS-CoV-2 variants using viral sequencing for the Centers for Disease Control and Prevention genomic surveillance program. BMC Infect. Dis. 2022, 22, 404. [Google Scholar] [CrossRef]
- Mao, K.; Zhang, K.; Du, W.; Ali, W.; Feng, X.; Zhang, H. The potential of wastewater-based epidemiology as surveillance and early warning of infectious disease outbreaks. Curr. Opin. Environ. Sci. Health 2020, 17, 1–7. [Google Scholar] [CrossRef]
- Kumblathan, T.; Liu, Y.; Uppal, G.K.; Hrudey, S.E.; Li, X.F. Wastewater-Based Epidemiology for Community Monitoring of SARS-CoV-2: Progress and Challenges. ACS Environ. 2021, 1, 18–31. [Google Scholar] [CrossRef]
- Government of Western Australia. Review of Western Australia’s COVID-19 Management and Response—July 2023; 2023. Available online: https://www.wa.gov.au/organisation/department-of-the-premier-and-cabinet/review-of-was-covid-19-management-and-response (accessed on 25 February 2024).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target [Fluorophore] | Type | Nucleotide Sequence (5′ to 3′) |
|---|---|---|
| Nucleocapsid [FAM] | Forward Primer | GGGGAACTTCTCCTGCTAGAAT |
| Reverse Primer | CAGACATTTTGCTCTCAAGCTG | |
| Probe | TTGCTGCTGCTTGACAGATT | |
| ORF1ab [ROX] | Forward Primer | CCCTGTGGGTTTTACACTTAA |
| Reverse Primer | ACGATTGTGCATCAGCTGA | |
| Probe | CCGTCTGCGGTATGTGGAAAGGTTATGG |
| Quarter-Year | Number of Clinical Cases Sequenced | Number of Wastewater Samples Sequenced | rs | p |
|---|---|---|---|---|
| Q3 2022 | 1411 | 43 | 0.806 | <0.001 |
| Q4 2022 | 1737 | 39 | 0.747 | <0.001 |
| Q1 2023 | 1613 | 26 | 0.773 | <0.001 |
| Q2 2023 | 1736 | 38 | 0.703 | <0.001 |
| Q3 2023 | 708 | 36 | 0.771 | <0.001 |
| Q4 2023 | 210 | 40 | 0.670 | <0.001 |
| Lineage | Pangolin Designation Date | Wastewater (Earliest Date of Collection) | Clinical (Earliest Date of Collection) | Difference (Number of Days) |
|---|---|---|---|---|
| BA.4.6.X | 03/07/2022 | 05/07/2022 | 15/08/2022 | −41 |
| BF.7.X | 16/07/2022 | 19/07/2022 | 22/09/2022 | −65 |
| BQ.1.X | 03/09/2022 | 29/09/2022 | 25/09/2022 | +4 |
| XBB.X (Other) | 18/09/2022 | 06/10/2022 | 30/09/2022 | +6 |
| XBC.X | 25/09/2022 | 13/10/2022 | 13/10/2022 | 0 |
| CH.1.1.X | 12/10/2022 | 21/12/2022 | 30/10/2022 | +52 |
| XBF.X | 04/11/2022 | 17/11/2022 | 01/12/2022 | −14 |
| JN.1.X | 13/01/2023 | 19/10/2023 | 12/11/2023 | −24 |
| EG.5.X | 23/04/2023 | 20/04/2023 | 16/05/2023 | −26 |
| BA.2.86.X | 17/08/2023 | 12/10/2023 | 22/08/2023 | +51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazeley, J.; Lee, T.; Knight, D.R.; Shivarev, A.; Gordon, C.; Speers, D.; Barth, D.D.; Maticevic, J.; Hodge, M.; Armstrong, P.; et al. Correlating Quantitative and Genomic SARS-CoV-2 Wastewater Data with Clinical Metrics in Metropolitan Perth, Western Australia. Environments 2024, 11, 62. https://doi.org/10.3390/environments11040062
Gazeley J, Lee T, Knight DR, Shivarev A, Gordon C, Speers D, Barth DD, Maticevic J, Hodge M, Armstrong P, et al. Correlating Quantitative and Genomic SARS-CoV-2 Wastewater Data with Clinical Metrics in Metropolitan Perth, Western Australia. Environments. 2024; 11(4):62. https://doi.org/10.3390/environments11040062
Chicago/Turabian StyleGazeley, Jake, Terence Lee, Daniel R. Knight, Alexander Shivarev, Cameron Gordon, David Speers, Dylan D. Barth, Jelena Maticevic, Meredith Hodge, Paul Armstrong, and et al. 2024. "Correlating Quantitative and Genomic SARS-CoV-2 Wastewater Data with Clinical Metrics in Metropolitan Perth, Western Australia" Environments 11, no. 4: 62. https://doi.org/10.3390/environments11040062