1. Introduction
Multiple sclerosis (MS) is a chronic, inflammatory, demyelinating disease affecting the central nervous system (CNS) [
1,
2]. In MS, lesions occur in different focal areas of the CNS through the creation of demyelinating plaques with varying degrees of inflammation, gliosis, and neurodegeneration [
3]. These alterations are associated with axon-neuronal loss and disruptions in nerve conduction, resulting in diminished or slowed signals, giving rise to the hallmark symptoms of this disease [
4].
MS is the most common neurological condition leading to disability in young adults in Europe and North America. At present, the cause of this condition remains unknown, and it is thought to have a potential origin influenced by multiple factors [
4]. MS is distinguished by a diverse array of symptoms and progression patterns. Specifically, upper limb (UL) impairments have a high prevalence in individuals with this condition [
5]. According to Bertoni et al. [
6], these UL alterations are present in approximately 60% of patients at the time of diagnosis and occur to a greater extent early in the course of the disease. The concerns most frequently mentioned by patients in relation to their UL are alterations in sensation, strength, and fine and gross motor skills. When cerebellar involvement occurs, dysdiadochokinesia (a common disorder in MS patients) may appear, which is characterized by a limitation or inability to perform rapid and alternating movements. Consequently, this results in a number of functional impairments, which may be combined with cognitive decline, impacting the ability to perform activities of daily living, which, in turn, directly affects the quality of life of people with MS (pwMS) [
7,
8,
9].
The evaluation of the sensorimotor function of the hand has allowed the physical and cognitive assessment of numerous health conditions, as well as serving as a predictor of change and evolution [
10]. Concretely, the finger tapping test (FTT) has been used to assess motor performance of the hand and fingers in healthy subjects [
11] and a wide variety of pathologies, such as neurological disorders [
12,
13]. Further, the FTT is a tool developed as part of the Halstead Battery [
14] for the neurophysiological assessment of motor control, being used in the evaluation of motor performance and eye–hand coordination [
12,
15]. The FTT has been used in the assessment of people with MS in several studies and has been found to be a reliable and valid assessment tool in this population to evaluate motor performance, as its scores are strongly associated with the estimated clinical severity of the disease [
12,
13].
mHealth is defined as the use of mobile devices to provide healthcare and information to consumers. Mobile applications (apps) are a promising tool in healthcare, offering new perspectives to patients and healthcare professionals, as well as to the general population. Apps focused on health, help to achieve a specific goal, or perform daily activities [
16]. Since smartphones became popular, numerous health-focused apps have been developed [
10]. The development of FTT applications has provided low-cost objective tools that have solved the difficulties presented by mechanical calibrators, which have the disadvantage of having to exert a certain force as well as exert the movement on a single axis of movement, which is limiting for certain groups of patients [
10]. In recent years, an exponential increase in the use of mHealth in the development of everyday activities has been observed [
17]. The interaction of users with these applications is generally simple, and the possibility of their application to various diseases has been studied [
18]. Different mobile applications have been developed to assess UL coordination via mobile smartphones [
18,
19], as well as for self-management of pwMS [
20]. However, the everyday use of smartphones has raised the question of their usefulness as a clinical tool. Prior to their clinical use, these devices and applications should be evaluated in terms of feasibility and psychometric properties, including construct validity (the relationship between the measure of interest and other related measures) and test–retest reliability. In this sense, several FTT applications have been designed, such as the one developed by SYBU (Data Digital Finger Tapping Test (version 3.5)) [
21] or the Hand Assessment Test app [
22], which are part of motor assessment batteries. Unlike these apps, the TappingPro
® mobile app [
23] is specific in its analysis of FTT and provides specific and detailed information that can be useful in clinical and research settings. The TappingPro
® mobile app provides values that no other mobile app has presented: number of beats per unit of time, explosive speed (number of beats in the first 5 s), fatigue (comparison of beats per interval), and acceleration (time up to 60 beats).
The aim of the present study was to evaluate the intra- and inter-rater reliability of the TappingPro® mobile app and its validity with validated clinical scales for motor performance, first in healthy subjects and secondarily with a representative sample of pwMS with a mild to moderate severity of the illness. The initial hypothesis of this study was that the TappingPro® mobile app would present excellent intra- and inter-rater reliability and a correlation with other motor performance measures in pwMS.
4. Discussion
The purpose of the present study was to evaluate the intra- and inter-rater reliability of the TappingPro® mobile app and the construct validity between this app and validated clinical scales for motor performance in healthy subjects and pwMS.
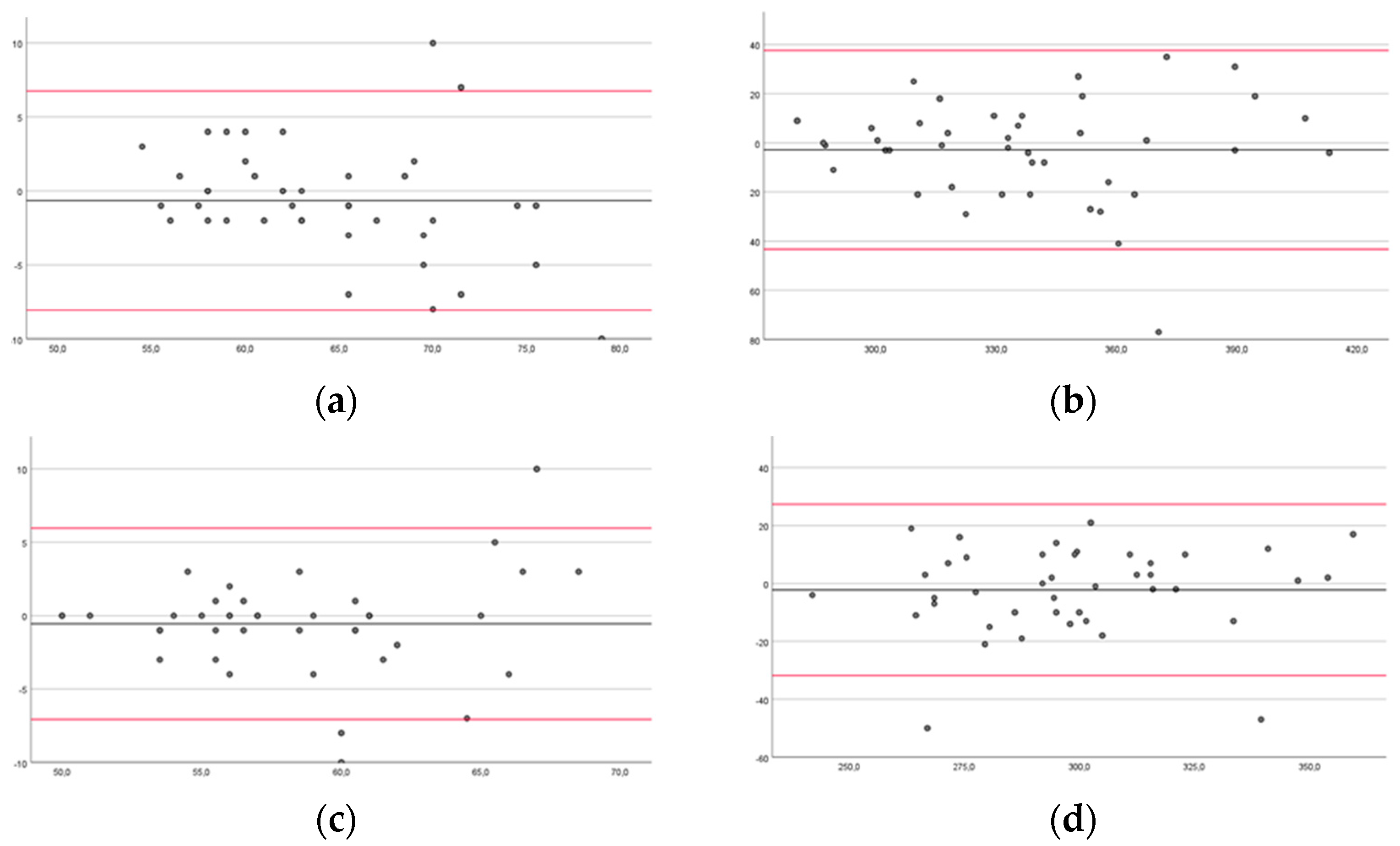
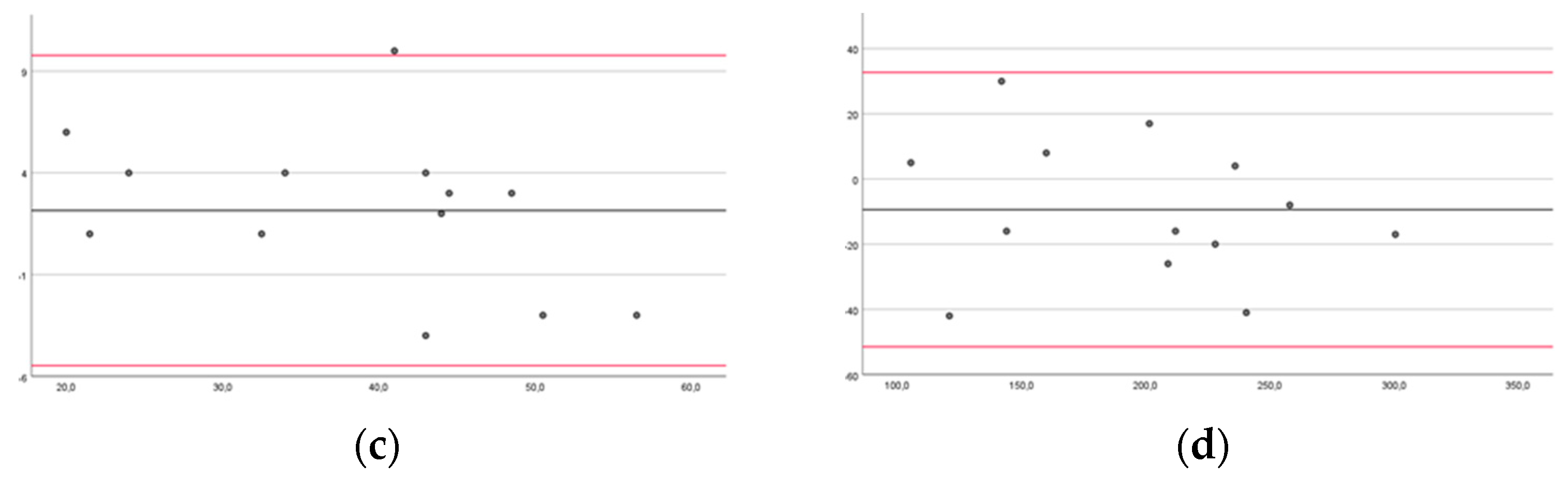
Our findings showed good intra-rater reliability in healthy subjects and excellent reliability in pwMS. The inter-rater reliability was good for the left hand in the FTT 10 s of the healthy subjects, and excellent for all the other measurements of the healthy subjects and pwMS. However, the Bland–Altman plots may be more useful than the ICC, as they can be readily and easily interpreted in a meaningful way in both clinical and research settings. Specifically, the width of the limits of agreement is useful in understanding the level of agreement or disagreement between observers, measurements, or systems [
42,
46]. In the intra-rater reliability, the range of the limits of agreement was slightly narrower for healthy subjects for NDUL in FTT 10 s (−7.59 to 8.45) and 60 s (31.5 to 38.5), and for pwMS for MAUL in FTT 10 s (−11.62 to 7.31) and 60 s (−24.3 to 39.22). There was no outlier for LAUL in FTT 10 s for pwMS, and at most three outliers for DUL in FTT 60 s for healthy subjects. In the inter-rater reliability, the range of the limits of agreement was slightly narrower for healthy subjects for NDUL in FTT 10 s (−7.07 to 5.98) and 60 s (−31.84 to 27.41), and for pwMS for MAUL in FTT 10 s (−5.47 to 9.78) and for LAUL in FTT 60 s (−27.58 to 36.96). There was no outlier for LAUL in FTT 10 s and 60 s and for MAUL in FTT 60 s for pwMS, and at most three outliers for DUL and NDUL in FTT 10 s for healthy subjects.
Regarding the construct validity of the app with validated clinical scales for motor performance in healthy subjects and pwMS, correlation analysis for healthy subjects showed poor correlations between the 10 and 60 s FTT but excellent correlations between these two tests and the manual dexterity tests (BBT and 9 HPT). The correlation analysis for pwMS showed excellent associations between BBT and all the measures of the FTT and between the NHPT and FTT 10 s for LAUL and FTT 60 s for MAUL. The correlations between NHPT and FFT 60 s for MAUL and FFT 10 s for LAUL were moderate. The correlations between hand grip strength and FFT were poor. These findings could be interpreted as the mobile application would present a construct validity with validated clinical scales for motor performance in pwMS related to coordination outcomes (BBT and NHPT), considered a convergent construct validity, but not with hand grip strength.
It is noteworthy to mention that mobile applications have become one of the most widely used tools in healthcare contexts, owing to their capacity to facilitate individual care, provide seamless access to information and communication, and enable the monitoring of health-related parameters [
16,
18]. Furthermore, numerous studies have sought to investigate and validate their use in pwMS to complement their medical and rehabilitative treatment, promote engagement in physical and mental activities, and facilitate medication monitoring [
47,
48,
49,
50]. For example, Pedullà et al. [
47], attempted to verify the effectiveness of a mobile application called COGNI-TRAcK for intensive and adaptive treatment based on memory exercises aimed at improving the cognitive state of pwMS. Golan et al. [
48] sought to assess the utility and validity of using a mobile application (MyMS&Me) based on an electronic diary to evaluate adherence and the effectiveness of pharmacological regimens in this population. Finally, Nasseri et al. [
49] and Van Geel et al. [
50] aimed to understand the effects of using two mobile applications on motivation to engage in physical activity, fatigue, and cognitive levels in pwMS. However, few studies have investigated the validity and reliability of applications designed to assess UL motor function in people with neurological disorders. As an example, the study conducted by Mollà-Casanova et al. [
51] aimed to determine the validity and reliability of a mobile application (the Hand Assessment Test) for assessing UL function in stroke individuals. The findings of this research supported the efficacy of this tool in fulfilling the required function, thus establishing it as a complementary instrument for assessing manual function in individuals with stroke.
To our best knowledge, applications related to the assessment of motor function, specifically UL motor dexterity, are scarcely explored in pwMS. In this context, the Tapping Pro
® mobile application, despite not being originally designed for the purpose of evaluating UL motor dexterity in individuals with MS, might offer the possibility of recording a set of parameters that may provide insights at the clinical level. According to the results obtained in the present study, with excellent intra- and inter-observer reliability and strong correlation with motor dexterity scales (BBT and NHPT), we could assume that the FTT within the Tapping Pro
® application emerges as a reliability tool for assessing manual dexterity and with a convergent construct validity in pwMS. Furthermore, its accessibility, ease of use, ability to gather quantitative objective data, portability, and low cost (1.99 euros) are among the inherent benefits of using this application for evaluating UL motor dexterity in pwMS [
29].
It is important to mention that the individuals with MS included in this study exhibited an average age of 51.69 (±6 years). According to Mathiowetz et al. [
34], the average scores for healthy individuals aged between 45 and 57 years on the BBT range from 73.6 to 83 points, varying depending on the limb assessed, the subject’s gender, and their age. However, the scores obtained in this study in subjects with MS were 49.62 (±18.36) and 56.46 (±17.53) in the MAUL and LAUL, respectively. Furthermore, the average values of the NHPT test for healthy subjects show a range from 17.3 to 21.0 s [
52], whereas individuals with MS included in our study exhibited results ranging from 33.63 (±22.31) to 56.01 (±49) seconds. Comparing the standardized average data of healthy subjects [
34,
52] to those with MS included in this study, it is readily apparent that the disease has a significant impact on both gross and fine motor skills in pwMS, as well as on UL coordination. Additionally, it is well known that loss of manual dexterity is associated with a decrease in independence to perform activities of daily living and, consequently, a decline in quality of life in pwMS [
5,
6,
9]. Therefore, the use of valid, reliable, user-friendly, and cost-effective tools, such as the FTT within the Tapping Pro
®, could become an interesting technological tool for monitoring manual dexterity and coordination to detect and/or treat their early deterioration in pwMS, owing to its close correlation (convergent construct validity) with outcomes, such as the BBT and the NHPT. So, future studies could be conducted in this line to corroborate these hypotheses.
There are several limitations to this study that warrant attention. Firstly, it is important to note that the findings may not be applicable to the broader population of individuals with MS or other neurological disorders, given that the study focused exclusively on patients scoring between 3.0 and 7.5 on the EDSS scale. Secondly, the sampling technique utilized might have introduced selection bias, considering that participants were sourced solely from a single MS association in a particular geographical area. Third, the Tapping Pro® app is only available for the iOS operating system, which may restrict its usage in situations where such devices are not available. Fourth, the Tapping Pro® app costs less than USD 2, but having a device with an iOS operating system, such as the one used in this study, costs more than USD 400/370 Euros, which could be socioeconomically challenging and most likely unavailable in some areas of the world.
Future studies could use our protocol to monitor disease progression, therapeutic effects, and/or for the early detection of motor symptoms in pwMS.

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}