Nucleus Accumbens Volume Is Associated with Frequency of Alcohol Use among Juvenile Justice-Involved Adolescents

Abstract
:1. Introduction
2. Results and Discussion

{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Accumbens | - | |||||
| 2. OFC | 0.42 ** | - | ||||
| 3. Accumbens by OFC | 0.31 ** | 0.29 ** | - | |||
| 4. Past 3-month Frequency | 0.13 | −0.11 | 0.09 | - | ||
| 5. Past 3-month Quantity | 0.01 | −0.09 | −0.04 | 0.55 ** | - | |
| 6. Years of Alcohol Use | 0.05 | −0.02 | 0.04 | 0.36 ** | 0.42 ** | - |
2.1. Regression Models
2.1.1. Quantity of Alcohol Use
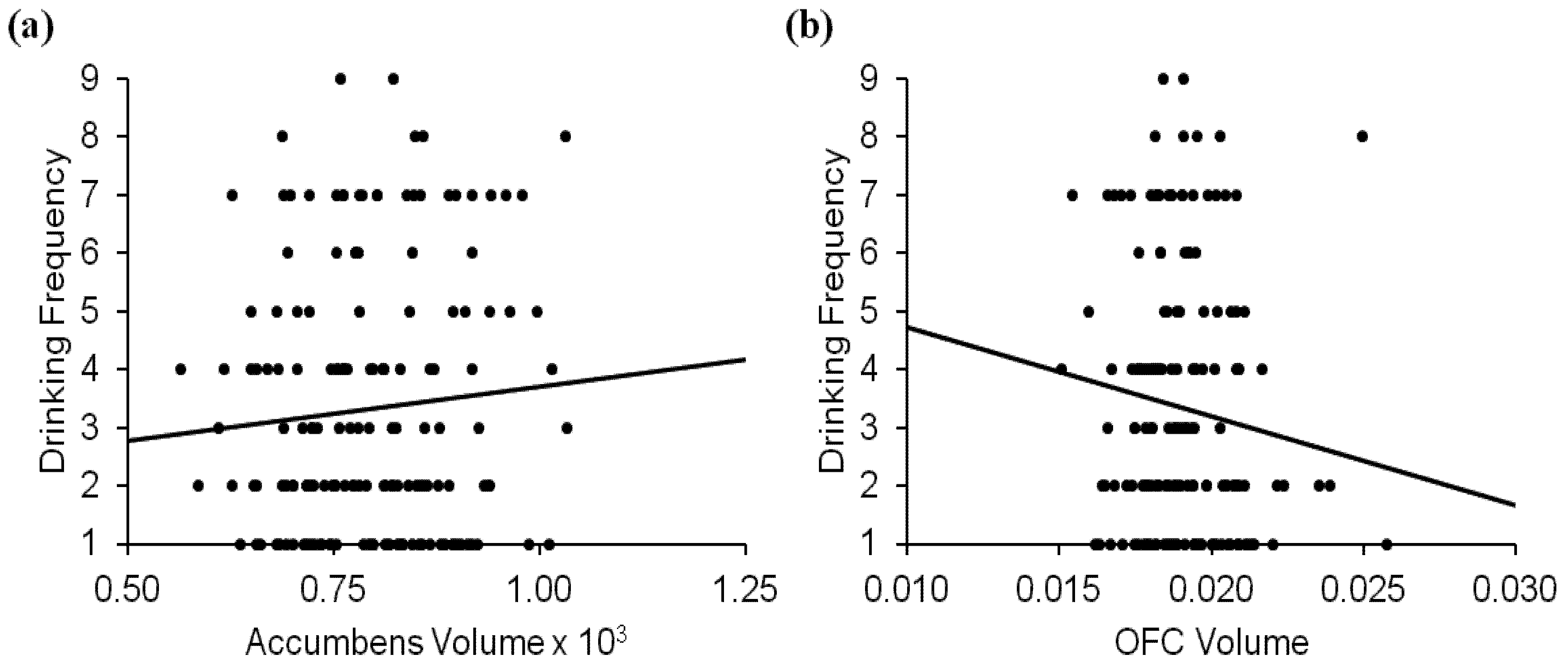
2.1.2. Frequency of Alcohol Use
| Standardized b † | p | R2 | Δ R2 | Δ F | |
|---|---|---|---|---|---|
| Quantity | |||||
| Step 1 | <0.001 | 0.21 | 0.21 | 8.75 | |
| Age | 0.06 | 0.45 | |||
| Years Alcohol | 0.38 | <0.001 | |||
| Years Tobacco | −0.16 | 0.06 | |||
| Years Marijuana | 0.23 | 0.02 | |||
| Years Other Drugs | −0.05 | 0.59 | |||
| Step 2 | 0.74 ‡ | 0.22 | 0.01 | 0.42 | |
| Accumbens | 0.03 | 0.71 | |||
| OFC | −0.07 | 0.38 | |||
| Accumbens × OFC | −0.04 | 0.64 | |||
| Frequency | |||||
| Step 1 | <0.001 | 0.15 | 0.15 | 5.83 | |
| Age | −0.06 | 0.42 | |||
| Years Alcohol | 0.31 | <0.001 | |||
| Years Tobacco | −0.10 | 0.25 | |||
| Years Marijuana | 0.16 | 0.10 | |||
| Years Other Drugs | 0.02 | 0.88 | |||
| Step 2 | 0.03 ‡ | 0.20 | 0.05 | 2.96 | |
| Accumbens | 0.18 | 0.03 | |||
| OFC | −0.20 | 0.02 | |||
| Accumbens × OFC | 0.09 | 0.25 | |||

2.1.3. Possible Moderators of Volumetric Effects on Frequency of Alcohol Use
| Standardized b | p | R2 | Δ R2 ‡ | Δ F ‡ | |
|---|---|---|---|---|---|
| Total Scale Scores | <0.01 ‡ | 0.26 | 0.06 | 4.42 | |
| Age | −0.02 | 0.77 | |||
| Years Alcohol | 0.32 | <0.001 | |||
| Years Tobacco | −0.09 | 0.29 | |||
| Years Marijuana | 0.13 | 0.17 | |||
| Years Other Drugs | −0.05 | 0.59 | |||
| Accumbens | 0.17 | 0.03 | |||
| OFC | −0.21 | <0.01 | |||
| Accumbens × OFC | 0.11 | 0.16 | |||
| CDI | −0.23 | <0.01 | |||
| CASS | 0.19 | 0.04 | |||
| CBCL | 0.11 | 0.24 | |||
| Moderation by Sex | 0.47 ‡ | 0.22 | 0.02 | 0.90 | |
| Age | −0.07 | 0.34 | |||
| Years Alcohol | 0.28 | 0.001 | |||
| Years Tobacco | −0.09 | 0.28 | |||
| Years Marijuana | 0.16 | 0.12 | |||
| Years Other Drugs | 0.04 | 0.73 | |||
| Accumbens | 0.08 | 0.70 | |||
| OFC | −0.19 | 0.26 | |||
| Accumbens × OFC | 0.22 | 0.10 | |||
| Gender | 0.05 | 0.54 | |||
| Accumbens × Gender | 0.06 | 0.74 | |||
| OFC × Gender | −0.01 | 0.98 | |||
| Accumbens × OFC × Gender | −0.18 | 0.08 | |||
| Moderation by Age | 0.16 ‡ | 0.22 | 0.03 | 1.77 | |
| Age | −0.09 | 0.23 | |||
| Years Alcohol | 0.29 | 0.001 | |||
| Years Tobacco | −0.12 | 0.18 | |||
| Years Marijuana | 0.17 | 0.09 | |||
| Years Other Drugs | 0.02 | 0.82 | |||
| Accumbens | 0.15 | 0.08 | |||
| OFC | −0.20 | 0.02 | |||
| Accumbens × OFC | <0.01 | 0.93 | |||
| Accumbens × Age | 0.10 | 0.29 | |||
| OFC × Age | −0.16 | 0.07 | |||
| Accumbens × OFC × Age | 0.17 | 0.13 |
2.2. Key Findings and Limitations
3. Experimental Section
3.1. Participants
3.2. Measures
3.2.1. Sample Characteristics
3.2.2. Substance Use Quantity and Frequency
| Measures | Mean (SD; Range) |
|---|---|
| Total Scale Scores | |
| Pubertal Development Scale (PDS) † | 3.20 (0.39; 1.60–4.00) |
| Children’s Depression Index (CDI-S) | 2.85 (3.17; 0.00–19.00) |
| Connors-Wells Self-Report Scale (CASS-S) ‡ | 26.99 (13.77; 0.00–74.00) |
| Child Behavior Checklist (CBCL) Externalizing ‡ | 20.88 (12.78; 0.00–64.00) |
| Rutgers Alcohol Problems Index (RAPI) | 11.66 (13.24; 0.00–92.00) |
| Alcohol Use Disorders Identification Test (AUDIT) | 7.11 (6.93; 0.00–32.00) |
| Substance Use | |
| Alcohol use frequency (past 3 months) | 3.35 (2.25; 1.00–9.00) |
| Alcohol use quantity (past 3 months) | 3.34 (2.22; 1.00–10.00) |
| Alcohol use (years) | 2.69 (2.19; 0.00–11.00) |
| Tobacco use (years) | 1.99 (2.24; 0.00–10.00) |
| Marijuana use (years) | 3.24 (2.49; 0.00–11.00) |
| Other use (years) | 1.16 (1.42; 0.00–6.00) |
3.3. Volumetric Data
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Durazzo, T.C.; Tosun, D.; Buckley, S.; Gazdzinski, S.; Mon, A.; Fryer, S.L.; Meyerhoff, D.J. Cortical thickness, surface area, and volume of the brain reward system in alcohol dependence: Relationships to relapse and extended abstinence. Alcohol. Clin. Exp. Res. 2011, 35, 1187–1200. [Google Scholar] [CrossRef]
- Van Holst, R.J.; van Holstein, M.; van den Brink, W.; Veltman, D.J.; Goudriaan, A.E. Response inhibition during cue reactivity in problem gamblers: An fMRI study. PLoS One 2012, 7. [Google Scholar] [CrossRef]
- Casey, B.J.; Getz, S.; Galvan, A. The adolescent brain. Dev. Rev. 2008, 28, 62–77. [Google Scholar] [CrossRef]
- Gogtay, N.; Giedd, J.N.; Lusk, L.; Hayashi, K.M.; Greenstein, D.; Vaituzis, A.C.; Nugent, T.F., III; Herman, D.H.; Clasen, L.S.; Toga, A.W.; et al. Dynamic mapping of human cortical development during childhood through early adulthood. Proc. Natl. Acad. Sci. USA 2004, 101, 8174–8179. [Google Scholar]
- Casey, B.J.; Jones, R.M.; Hare, T.A. The adolescent brain. Ann. N. Y. Acad. Sci. 2008, 1124, 111–126. [Google Scholar]
- Casey, B.J.; Somerville, L.H.; Gotlib, I.H.; Ayduk, O.; Franklin, N.T.; Askren, M.K.; Jonides, J.; Berman, M.G.; Wilson, N.L.; Teslovich, T.; et al. Behavioral and neural correlates of delay of gratification 40 years later. Proc. Natl. Acad. Sci. USA 2011, 108, 14998–15003. [Google Scholar]
- Galvan, A.; Hare, T.A.; Parra, C.E.; Penn, J.; Voss, H.; Glover, G.; Casey, B.J. Earlier development of the accumbens relative to orbitofrontal cortex might underlie risk-taking behavior in adolescents. J. Neurosci. 2006, 26, 6885–6892. [Google Scholar] [CrossRef]
- Hare, T.A.; O’Doherty, J.; Camerer, C.F.; Schultz, W.; Rangel, A. Dissociating the role of the orbitofrontal cortex and the striatum in the computation of goal values and prediction errors. J. Neurosci. 2008, 28, 5623–5630. [Google Scholar] [CrossRef]
- Yau, W.Y.; Zubieta, J.K.; Weiland, B.J.; Samudra, P.G.; Zucker, R.A.; Heitzeg, M.M. Nucleus accumbens response to incentive stimuli anticipation in children of alcoholics: Relationships with precursive behavioral risk and lifetime alcohol use. J. Neurosci. 2012, 32, 2544–2551. [Google Scholar]
- Ernst, M.; Nelson, E.E.; Jazbec, S.; McClure, E.B.; Monk, C.S.; Leibenluft, E.; Blair, J.; Pine, D.S. Amygdala and nucleus accumbens in responses to receipt and omission of gains in adults and adolescents. Neuroimage 2005, 25, 1279–1291. [Google Scholar] [CrossRef]
- Boettiger, C.A.; Mitchell, J.M.; Tavares, V.C.; Robertson, M.; Joslyn, G.; D’Esposito, M.; Fields, H.L. Immediate reward bias in humans: Fronto-parietal networks and a role for the catechol-O-methyltransferase 158(Val/Val) genotype. J. Neurosci. 2007, 27, 14383–14391. [Google Scholar] [CrossRef]
- Medina, K.L.; Schweinsburg, A.D.; Cohen-Zion, M.; Nagel, B.J.; Tapert, S.F. Effects of alcohol and combined marijuana and alcohol use during adolescence on hippocampal volume and asymmetry. Neurotoxicol. Teratol. 2007, 29, 141–152. [Google Scholar] [CrossRef]
- Nagel, B.J.; Schweinsburg, A.D.; Phan, V.; Tapert, S.F. Reduced hippocampal volume among adolescents with alcohol use disorders without psychiatric comorbidity. Psychiatry Res. 2005, 139, 181–190. [Google Scholar] [CrossRef]
- Medina, K.L.; McQueeny, T.; Nagel, B.J.; Hanson, K.L.; Schweinsburg, A.D.; Tapert, S.F. Prefrontal cortex volumes in adolescents with alcohol use disorders: Unique gender effects. Alcohol. Clin. Exp. Res. 2008, 32, 386–394. [Google Scholar] [CrossRef]
- Medina, K.L.; Nagel, B.J.; Tapert, S.F. Abnormal cerebellar morphometry in abstinent adolescent marijuana users. Psychiatry Res. 2010, 30, 152–159. [Google Scholar]
- The National Juvenile Court Data Archive. Available online: http://www.ojjdp.gov/pubs/239114.pdf (accessed on 15 September 2012).
- Claus, E.D.; Magnan, R.E.; Montanaro, E.; Feldstein Ewing, S.W.; Hutchison, K.E.; Bryan, A.D. Neural mechanisms of risky decision making in juvenile justice involved adolescents. 2012, Unpublished work.
- Sullivan, E.V.; Deshmukh, A.; De Rosa, E.; Rosenbloom, M.J.; Pfefferbaum, A. Striatal and forebrain nuclei volumes: Contribution to motor function and working memory deficits in alcoholism. Biol. Psychiatry 2005, 57, 768–776. [Google Scholar]
- Spanagel, R. Alcoholism: A systems approach from molecular physiology to addictive behavior. Physiol. Rev. 2009, 89, 649–705. [Google Scholar] [CrossRef]
- Giedd, J.N.; Blumenthal, J.; Jeffries, N.O.; Castellanos, F.X.; Liu, H.; Zijdenbos, A.; Paus, T.; Evans, A.C.; Rapoport, J.L. Brain development during childhood and adolescence: A longitudinal MRI study. Nat. Neurosci. 1999, 2, 861–863. [Google Scholar] [CrossRef]
- Blanton, R.E.; Levitt, J.G.; Peterson, J.R.; Fadale, D.; Sporty, M.L.; Lee, M.; To, D.; Mormino, E.C.; Thompson, P.M.; McCracken, J.T.; Toga, A.W. Gender differences in the left inferior frontal gyrus in normal children. Neuroimage 2004, 22, 626–636. [Google Scholar] [CrossRef]
- Giedd, J.N.; Castellanos, F.X.; Rajapakse, J.C.; Vaituzis, A.C.; Rapoport, J.L. Sexual dimorphism of the developing human brain. Prog. Neuropsychopharmacol. Biol. Psychiatry 1997, 21, 1185–1201. [Google Scholar] [CrossRef]
- Giedd, J.N. The teen brain: Insights from neuroimaging. J. Adolesc. Health 2008, 42, 335–343. [Google Scholar] [CrossRef]
- Gogtay, N.; Thompson, P.M. Mapping gray matter development: Implications for typical development and vulnerability to psychopathology. Brain Cogn. 2010, 72, 6–15. [Google Scholar] [CrossRef]
- Alfonso-Loeches, S.; Guerri, C. Molecular and behavioral aspects of the actions of alcohol on the adult and developing brain. Crit. Rev. Clin. Lab. Sci. 2011, 48, 19–47. [Google Scholar] [CrossRef]
- Schneider, S.; Peters, J.; Bromberg, U.; Brassen, S.; Miedl, S.F.; Banaschewski, T.; Barker, G.J.; Conrod, P.; Flor, H.; Garavan, H.; et al. Risk taking and the adolescent reward system: A potential common link to substance abuse. Am. J. Psychiatry 2012, 169, 39–46. [Google Scholar]
- Tanabe, J.; Tregellas, J.R.; Dalwani, M.; Thompson, L.; Owens, E.; Crowley, T.; Banich, M. Medial orbitofrontal cortex gray matter is reduced in abstinent substance-dependent individuals. Biol. Psychiatry 2009, 65, 160–164. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurocircuitry of addiction. Neuropsychopharmacology 2010, 35, 217–238. [Google Scholar] [CrossRef]
- Chung, T.; Smith, G.T.; Donovan, J.E.; Windle, M.; Faden, V.B.; Chen, C.M.; Martin, C.S. Drinking frequency as a brief screen for adolescent alcohol problems. Pediatrics 2012, 129, 205–212. [Google Scholar] [CrossRef]
- Sowell, E.R.; Thompson, P.M.; Holmes, C.J.; Jernigan, T.L.; Toga, A.W. In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nat. Neurosci. 1999, 2, 859–861. [Google Scholar] [CrossRef]
- Petersen, A.C.; Crockett, L.; Richards, M.; Boxer, A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J. Youth Adolesc. 1988, 2, 117–133. [Google Scholar]
- Kovacs, M. The Children’s Depression Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Conners, C.K.; Jett, J.L. Attention Deficit Hyperactivity Disorder: The Latest Assessment and Treatment Strategies, 1th ed; Compact Clinicals: Kansas, MO, USA, 1999. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont: Burlington, VT, USA, 2001. [Google Scholar]
- White, H.R.; Labouvie, E.W. Towards the assessment of adolescent problem drinking. J. Stud. Alcohol 1989, 50, 30–37. [Google Scholar]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care, 2nd ed; World Health Organization: Geneva, Switzerlands, 2001. [Google Scholar]
- Van Der Kouwe, A.J.; Benner, T.; Salat, D.H.; Fischl, B. Brain morphometry with multiecho MPRAGE. Neuroimage 2008, 40, 559–569. [Google Scholar] [CrossRef]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; van der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S.; et al. Whole brain segmentation: Automated labeling of neuroanatomical structures in the human brain. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef]
- Fischl, B.; van der Kouwe, A.; Destrieux, C.; Halgren, E.; Segonne, F.; Salat, D.H.; Busa, E.; Seidman, L.J.; Goldstein, J.; Kennedy, D.; et al. Automatically parcellating the human cerebral cortex. Cereb. Cortex 2004, 14, 11–22. [Google Scholar] [CrossRef]
- Marenco, S.; Stein, J.L.; Savostyanova, A.A.; Sambataro, F.; Tan, H.Y.; Goldman, A.L.; Verchinski, B.A.; Barnett, A.S.; Dickinson, D.; Apud, J.A.; et al. Investigation of anatomical thalamo-cortical connectivity and FMRI activation in schizophrenia. Neuropsychopharmacology 2012, 37, 499–507. [Google Scholar] [CrossRef]
- Sullivan, E.V.; Pfefferbaum, A. Neurocircuitry in alcoholism: A substrate of disruption and repair. Psychopharmacology 2005, 180, 583–594. [Google Scholar] [CrossRef]
- Steinberg, L. A social neuroscience perspective on adolescent risk-taking. Dev. Rev. 2008, 28, 78–106. [Google Scholar]
- Steinberg, L. A behavioral scientist looks at the science of adolescent brain development. Brain Cogn. 2010, 72, 160–164. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Thayer, R.E.; Crotwell, S.M.; Callahan, T.J.; Hutchison, K.E.; Bryan, A.D. Nucleus Accumbens Volume Is Associated with Frequency of Alcohol Use among Juvenile Justice-Involved Adolescents. Brain Sci. 2012, 2, 605-618. https://doi.org/10.3390/brainsci2040605
Thayer RE, Crotwell SM, Callahan TJ, Hutchison KE, Bryan AD. Nucleus Accumbens Volume Is Associated with Frequency of Alcohol Use among Juvenile Justice-Involved Adolescents. Brain Sciences. 2012; 2(4):605-618. https://doi.org/10.3390/brainsci2040605
Chicago/Turabian StyleThayer, Rachel E., Shirley M. Crotwell, Tiffany J. Callahan, Kent E. Hutchison, and Angela D. Bryan. 2012. "Nucleus Accumbens Volume Is Associated with Frequency of Alcohol Use among Juvenile Justice-Involved Adolescents" Brain Sciences 2, no. 4: 605-618. https://doi.org/10.3390/brainsci2040605