

The Inflammatory and Oxidative Status of Newly Diagnosed Class III and Class IV Lupus Nephritis, with Six-Month Follow-Up

 , , , , ,
, , , , ,
Abstract
:1. Introduction
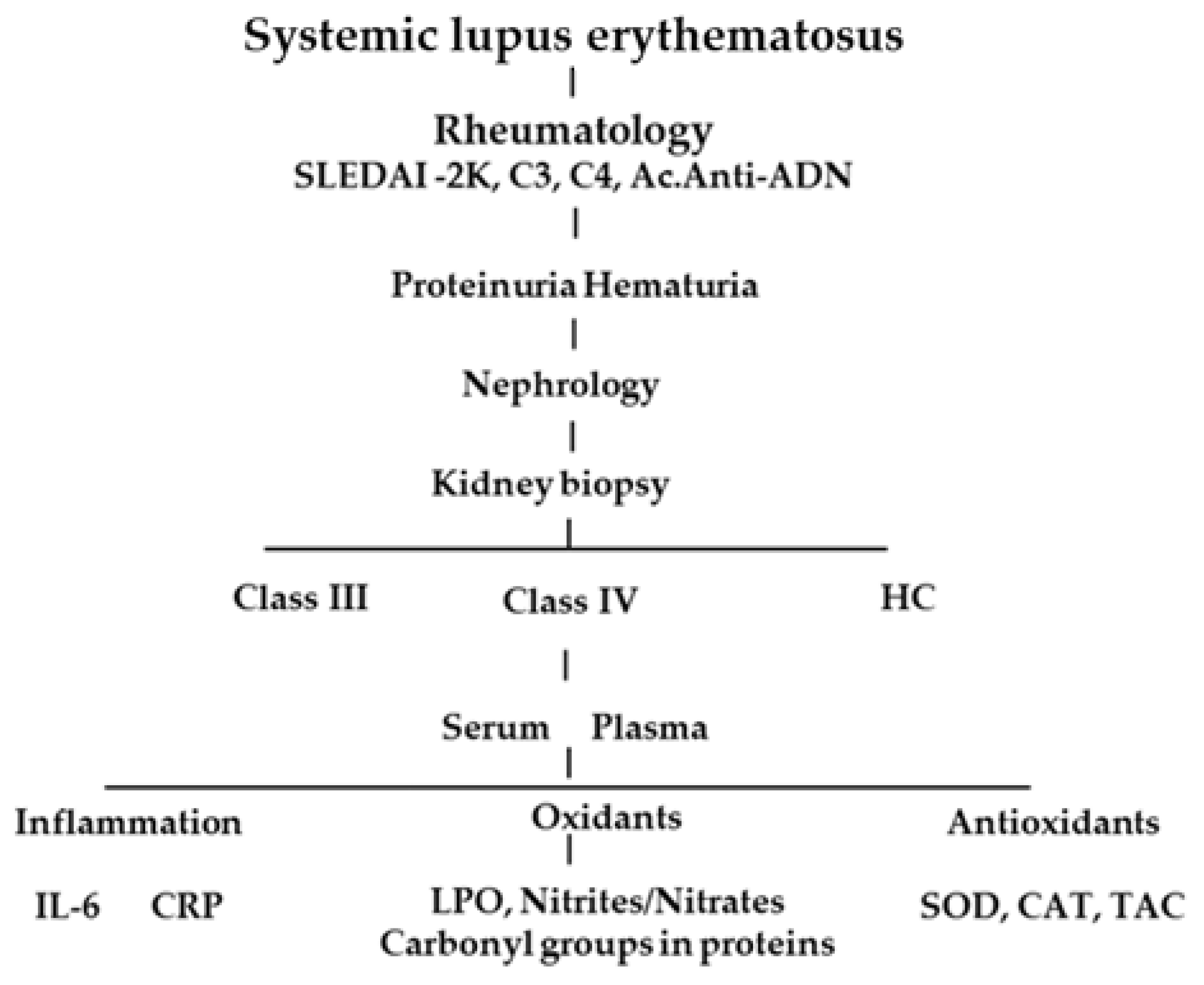
2. Materials and Methods
2.1. Data Collection
2.2. Oxidative Stress Markers
2.2.1. LPO
2.2.2. Nitrites/Nitrates
2.2.3. Carbonyl Groups in Proteins
2.3. Inflammation Markers
2.3.1. CRP
2.3.2. IL-6
2.4. Antioxidants
2.4.1. SOD
2.4.2. Total Antioxidant Capacity
2.4.3. Catalase
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schur, P.H.; Hahn, B.H. Epidemiology and Pathogenesis of Systemic Lupus Erythematosus; Up to date: Waltham, MA, USA, 2011. [Google Scholar]
- Mccarty, D.J.; Manzi, S.; Medsger, T.A., Jr.; Ramsey-Goldman, R.; Laporte, R.E.; Kwoh, C.K. Incidence of systemic lupus erythematosus race and gender differences. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1995, 38, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Fortuna, G.; Brennan, M.T. Systemic lupus erythematosus: Epidemiology, pathophysiology, manifestations, and management. Dent. Clin. 2013, 57, 631–655. [Google Scholar]
- Fava, A.; Petri, M. Systemic lupus erythematosus: Diagnosis and clinical management. J. Autoimmun. 2019, 96, 1–13. [Google Scholar] [CrossRef]
- Gasparotto, M.; Gatto, M.; Binda, V.; Doria, A.; Moroni, G. Lupus nephritis: Clinical presentations and outcomes in the 21st century. Rheumatology 2020, 59, v39–v51. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.; Mahajan, N.; Sah, S.; Nath, S.K.; Paudyal, B. Oxidative stress and its biomarkers in systemic lupus erythematosus. J. Biomed. Sci. 2014, 21, 23. [Google Scholar] [CrossRef]
- Ahsan, H.; Ali, A.; Ali, R. Oxygen free radicals and systemic autoimmunity. Clin. Exp. Immunol. 2003, 131, 398–404. [Google Scholar] [CrossRef]
- Spengler, M.I.; Svetaz, M.J.; Leroux, M.B.; Bertoluzzo, S.M.; Parente, F.M.; Bosch, P. Lipid peroxidation affects red blood cells membrane properties in patients with systemic lupus erythematosus. Clin. Hemorheol. Microcirc. 2013, 58, 489–495. [Google Scholar] [CrossRef]
- Bona, N.; Pezzarini, E.; Balbi, B.; Daniele, S.M.; Rossi, M.F.; Monje, A.L.; Basiglio, C.L.; Pelusa, H.F.; Arriaga, S.M.M. Oxidative stress, inflammation and disease activity biomarkers in lupus nephropathy. Lupus 2020, 29, 311–323. [Google Scholar] [CrossRef]
- Uchida, K. 4-Hydroxy-2-nonenal: A product and mediator of oxidative stress. Prog. Lipid Res. 2003, 42, 318–343. [Google Scholar] [CrossRef]
- Lopez, L.R.; Simpson, D.F.; Hurley, B.L.; Matsuura, E. OxLDL/beta2GPI complexes and autoantibodies in patients with systemic lupus erythematosus, systemic sclerosis, and antiphospholipid syndrome: Pathogenic implications for vascular involvement. Ann. N. Y. Acad. Sci. 2005, 1051, 313–322. [Google Scholar] [CrossRef]
- Dalle-Donne, I.; Rossi, R.; Colombo, R.; Giustarini, D.; Milzani, A. Biomarkers of oxidative damage in human disease. Clin. Chem. 2006, 52, 601–623. [Google Scholar] [CrossRef] [PubMed]
- Vipartene, D.; Iasiulevichute, L.; Butkene, B.; Valiukene, K.; Keturkene, A.; Redaitene, E. Pro- and antioxidant blood system in patients with rheumatoid arthritis and systemic lupus erythematosus. Ter. Arkh. 2006, 78, 10–14. [Google Scholar]
- Ginzler, E.; Guedes Barbosa, L.S.; D’Cruz, D.; Furie, R.; Maksimowicz-McKinnon, K.; Oates, J.; Santiago, M.B.; Saxena, A.; Sheikh, S.; Bass, D.L.; et al. Phase III/IV, Randomized, fifty-two-week study of the efficacy and safety of belimumab in patients of black african ancestry with systemic lupus erythematosus. Arthritis Rheumatol. 2022, 74, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.; Rovin, B.; Mysler, E.F.; Furie, R.A.; Houssiau, F.A.; Trasieva, T.; Knagenhjelm, J.; Schwetje, E.; Chia, Y.L.; Tummala, R.; et al. Phase II randomised trial of type I interferon inhibitor anifrolumab in patients with active lupus nephritis. Ann. Rheum. Dis. 2022, 81, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Tenorio, L.F.A.; del Valle, M.L.; Pastelin, H.G. Validación de un método analítico espectrofotométrico para la cuantificación de metabolitos estables de óxido nítrico en fluidos biológicos. Rev. Mex. De Cienc. Farm. 2005, 36, 31–41. [Google Scholar]
- Lenz, A.G.; Costabel, U.; Shaltiel, S.; Levine, R.L. Determination of carbonyl groups in oxidatively modified proteins by reduction with tritiated sodium borohydride. Anal. Biochem. 1989, 177, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, L.; Başkan, K.S.; Tütem, E.; Apak, R. Combined HPLC-CUPRAC (cupric ion reducing antioxidant capacity) assay of parsley, celery leaves, and nettle. Talanta 2008, 77, 304–313. [Google Scholar] [CrossRef]
- Hadwan, M.H.; Abed, H.N. Data supporting the spectrophotometric method for the estimation of catalase activity. Data Brief 2015, 17, 194–199. [Google Scholar] [CrossRef]
- Wang, H.; Ren, Y.L.; Chang, J.; Gu, L.; Sun, L.Y. A systematic review and meta-analysis of prevalence of biopsy-proven lupus nephritis. Arch. Rheumatol. 2017, 33, 17–25. [Google Scholar] [CrossRef]
- Emad, G.; Al-Barshomy, S.M. Anti-C1q antibodies in lupus nephritis and their correlation with the disease activity. Saudi J. Kidney Dis. Transpl. 2020, 31, 342–352. [Google Scholar] [PubMed]
- Iwano, M.; Dohi, K.; Hirata, E.; Kurumatani, N.; Horii, Y.; Shiiki, H.; Fukatsu, A.; Matsuda, T.; Hirano, T.; Kishimoto, T.; et al. Urinary levels of IL-6 in patients with active lupus nephritis. Clin. Nephrol. 1993, 40, 16–21. [Google Scholar] [PubMed]
- Cash, H.; Relle, M.; Menke, J.; Brochhausen, C.; Jones, S.A.; Topley, N.; Galle, P.R.; Schwarting, A. Interleukin 6 (IL-6) deficiency delays lupus nephritis in MRL-Faslpr mice: The IL-6 pathway as a new therapeutic target in treatment of autoimmune kidney disease in systemic lupus erythematosus. J. Rheumatol. 2010, 37, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Lei, C.T.; Zhang, C. Interleukin-6 signaling pathway and its role in kidney disease: An update. Front. Immunol. 2017, 21, 405. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K. Does the interdependence between oxidative stress and inflammation explain the antioxidant paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [PubMed]
- Podkowińska, A.; Formanowicz, D. Chronic Kidney Disease as Oxidative Stress- and Inflammatory-Mediated Cardiovascular Disease. Antioxidants 2020, 9, 752. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Hammond, D.J., Jr.; Singh, S.K.; Thompson, J.A.; Beeler, B.W.; Rusiñol, A.E.; Pangburn, M.K.; Potempa, L.A.; Agrawal, A. Identification of acidic pH-dependent ligands of pentameric C-reactive protein. J. Biol. Chem. 2010, 285, 36235–36244. [Google Scholar] [CrossRef]
- Enocsson, H.; Gullstrand, B.; Eloranta, M.L.; Wetterö, J.; Leonard, D.; Rönnblom, L.; Bengtsson, A.A.; Sjöwall, C. C-reactive protein levels in systemic lupus erythematosus are modulated by the interferon gene signature and CRP gene polymorphism rs1205. Front. Immunol. 2021, 11, 622326. [Google Scholar] [CrossRef]
- Song, L.J.; Liu, W.W.; Fan, Y.C.; Qiu, F.; Chen, Q.L.; Li, X.F.; Ding, F. The positive correlations of apolipoprotein E with disease activity and related cytokines in systemic lupus erythematosus. Diagn. Pathol. 2013, 8, 175. [Google Scholar] [CrossRef]
- Tanaka, Y. State-of-the-art treatment of systemic lupus erythematosus. Int. J. Rheum. Dis. 2020, 23, 465–471. [Google Scholar] [CrossRef]
- Otaki, N.; Chikazawa, M.; Nagae, R.; Shimozu, Y.; Shibata, T.; Ito, S.; Takasaki, Y.; Fujii, J.; Uchida, K. Identification of a lipid peroxidation product as the source of oxidation-specific epitopes recognized by anti-DNA autoantibodies. J. Biol. Chem. 2010, 285, 33834–33842. [Google Scholar] [CrossRef]
- El Hajj, S.; Canabady-Rochelle, L.; Gaucher, C. Nature-inspired bioactive compounds: A promising approach for ferroptosis-linked human diseases? Molecules 2023, 28, 2636. [Google Scholar] [CrossRef] [PubMed]
- Bevan, R.J.; Durand, M.F.; Hickenbotham, P.T.; Kitas, G.D.; Patel, P.R.; Podmore, I.D.; Griffiths, H.R.; Waller, H.L.; Lunec, J. Validation of a novel ELISA for measurement of MDA-LDL in human plasma. Free Radic. Biol. Med. 2003, 35, 517–527. [Google Scholar] [CrossRef]
- Wang, G.; Pierangeli, S.S.; Willis, R.; Gonzalez, E.B.; Petri, M.; Khan, M.F. Significance of lipid-derived reactive aldehyde-specific immune complexes in systemic lupus erythematosus. PLoS ONE 2016, 11, e0164739. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; de Leeuw, K.; Arends, S.; Doornbos-van der Meer, B.; Bulthuis, M.L.; van Goor, H.; Westra, J. Biomarkers of Oxidative Stress in Systemic Lupus Erythematosus Patients with Active Nephritis. Antioxidants 2023, 12, 1627. [Google Scholar] [CrossRef]
- Nagy, G.; Koncz, A.; Telarico, T.; Fernandez, D.; Ersek, B.; Buzás, E.; Perl, A. Central role of nitric oxide in the pathogenesis of rheumatoid arthritis and systemic lupus erythematosus. Arthritis Res. Ther. 2010, 12, 210. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.E.; Sturgess, A.D.; Hennessy, A.; Davies, M.J. Serum protein oxidation and apolipoprotein CIII levels in people with systemic lupus erythematosus with and without nephritis. Free Radic. Res. 2007, 41, 1301–1312. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, N.; Wang, H.; Wang, G.; Boor, P.J.; Khan, M.F. Redox-sensitive Nrf2 and MAPK signaling pathways contribute to trichloroethene-mediated autoimmune disease progression. Toxicology 2021, 457, 152804. [Google Scholar] [CrossRef]
- Morgan, P.E.; Sturgess, A.D.; Davies, M.J. Evidence for chronically elevated serum protein oxidation in systemic lupus erythematosus patients. Free Radic. Res. 2009, 43, 117–127. [Google Scholar] [CrossRef]
- Rysz, J.; Franczyk, B.; Ławiński, J.; Gluba-Brzózka, A. Oxidative Stress in ESRD Patients on Dialysis and the Risk of Cardiovascular Diseases. Antioxidants 2020, 9, 1079. [Google Scholar] [CrossRef] [PubMed]
- Németh, B.; Péter, I.; Boncz, I.; Jagicza, A.; Kiss, I.; Csergő, Á.; Kőszegi, T.; Kustán, P.; Horváth, I.G.; Ajtay, Z. Urinary orosomucoid: A new marker of cardiovascular risk in psoriatic patients? Ther. Clin. Risk Manag. 2019, 15, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Gaál, K.; Tarr, T.; Lőrincz, H.; Borbás, V.; Seres, I.; Harangi, M.; Fülöp, P.; Paragh, G. High-density lipopoprotein antioxidant capacity, subpopulation distribution and paraoxonase-1 activity in patients with systemic lupus erythematosus. Lipids Health Dis. 2016, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Cantisani, V.; Anania, C.; Bonaiuto, E.; Martino, F.; Pascone, R.; Chiesa, C. Serum uric acid and its association with metabolic syndrome and carotid atherosclerosis in obese children. Eur. J. Endocrinol. 2009, 160, 45–52. [Google Scholar] [CrossRef]
- Fridovich, I. The trail to superoxide dismutase. Protein Sci. 1998, 7, 2688–2690. [Google Scholar] [CrossRef]
- Sun, Y.; Oberley, L.W.; Li, Y.A. Simple method for clinical assay of superoxide dismutase. Clin. Chem. 1988, 34, 497–500. [Google Scholar] [CrossRef]
- Lv, Y.; He, S.; Zhang, Z.; Li, Y.; Hu, D.; Zhu, K.; Cheng, H.; Zhou, F.; Chen, G.; Zheng, X.; et al. Confirmation of C4 gene copy number variation and the association with systemic lupus erythematosus in Chinese Han population. Rheumatol. Int. 2012, 32, 3047–3053. [Google Scholar] [CrossRef]
- Angeletti, A.; Bruschi, M.; Kajana, X.; Spinelli, S.; Verrina, E.; Lugani, F.; Caridi, G.; Murtas, C.; Candiano, G.; Prunotto, M.; et al. Mechanisms liimiting renal tissue protection and repair in glomerulonephritis. Int. J. Mol. Sci. 2023, 24, 8318. [Google Scholar] [CrossRef]
- Cai, Z.; Zhang, S.; Wu, P.; Ren, Q.; Wei, P.; Hong, M.; Feng, Y.; Wong, C.K.; Tang, H.; Zeng, H. A novel potential target of IL-35-regulated JAK/STAT signaling pathway in lupus nephritis. Clin. Transl. Med. 2021, 11, e309. [Google Scholar] [CrossRef]
- Weinstein, A.; Alexander, R.V.; Zack, D.J. A review of complement activation in SLE. Curr. Rheumatol. Rep. 2021, 23, 16. [Google Scholar] [CrossRef]
- Nesarkigar, P.N.; Spiller, B.; Chavez, R. The complement system: History, pathways, cascade and inhibitors. Eur. J. Microbiol. Immunol. 2012, 2, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, A.; Bordwell, B.; Stone, B.; Tibbetts, C.; Rothfield, N.F. Antibodies to native DNA and serum complement (C3) levels. Application to the diagnosis and classification of systemic lupus erythematosus. Am. J. Med. 1983, 74, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- Pisetsky, D.S. Antinuclear antibodies in rheumatic disease: A proposal for a function-based classification. Scand. J. Immunol. 2012, 76, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Gatto, M.; Zen, M.; Iaccarino, L.; Punzi, L. Optimizing outcome in SLE: Treating-to-target and definition of treatment goals. Autoimmun. Rev. 2014, 13, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Hajji, M.; Harzallah, A.; Kaaroud, H.; Barbouch, S.; Hamida, F.B.; Abdallah, T.B. Factors associated with relapse of lupus nephritis: A single center study of 249 cases. Saudi J. Kidney Dis. Transpl. 2017, 28, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, I.; Birmingham, D.; Rovin, B.; Hebert, L. Commentary on the current guidelines for the diagnosis of lupus nephritis flare. Curr. Rheumatol. Rep. 2019, 21, 12. [Google Scholar] [CrossRef]
- Lakshmi, V.R.; Vangala, N.; Uppin, M.S.; Gudithi, S.; Taduri, G.; Raju, S.B. Revisiting vasculopathy in lupus nephritis: A renal biopsy evaluation study. Indian J. Nephrol. 2022, 32, 28–33. [Google Scholar]
- United States Renal Data System. 2023 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Available online: https://usrds-adr.niddk.nih.gov/2023 (accessed on 30 November 2023).
- Broder, A.; Mowrey, W.B.; Khan, H.N.; Jovanovic, B.; Londono-Jimenez, A.; Izmirly, P.; Putterman, C. Tubulointerstitial damage predicts end stage renal disease in lupus nephritis with preserved to moderately impaired renal function: A retrospective cohort study. Semin. Arthritis Rheum. 2018, 47, 545–551. [Google Scholar] [CrossRef]
- Yan, Z.; Chen, Q.; Xia, Y. Oxidative Stress Contributes to Inflammatory and Cellular Damage in Systemic Lupus Erythematosus: Cellular Markers and Molecular Mechanism. J. Inflamm. Res. 2023, 16, 453–465. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class III N-12 | Class IV N-12 | p | |
|---|---|---|---|
| Gender | |||
| Female n (%) | 10 (83.3) | 11 (91.7) | 0.55 |
| Male n (%) | 2 (16.7) | 1 (8.3) | |
| Arterial Hypertension n% | 3 (25) | 3 (25) | 1 |
| Age years | 27.83 ± 7.06 | 33.00 ± 7.87 | 0.11 |
| Weight Kg | 68.48 ± 23.26 | 63.21 ± 15.64 | 0.52 |
| Height cm | 163.42 ± 10.80 | 155.92 ± 4.46 | 0.037 |
| BMI Kg/m2 | 24.95 ± 1.26 | 25.66 ± 1.47 | 0.72 |
| Systemic lupus erythematosus data | |||
| SLEDAI -2K | 20.08 ± 6.92 | 25.33 ± 6.01 | 0.060 |
| C3 mg/dL | 115.97 ± 37.80 | 62.82 ± 11.40 | <0.001 |
| C4 mg/dL | 25.36 ± 6.34 | 12.18 ± 3.90 | <0.001 |
| Anti-DNA IU/mL | 25.12 ± 32.75 | 73.69 ± 74.69 | 0.05 |
| Biochemical data | |||
| Hemoglobin g/dL | 12.17 ± 2.40 | 11.23 ± 1.98 | 0.31 |
| Hematocrit g/dL | 35.04 ± 6.50 | 35.76 ± 5.41 | 0.77 |
| Platelets thousands/uL | 260.92 ± 64.19 | 239.92 ± 98.87 | 0.54 |
| Leukocytes thousands/uL | 7.67 ± 3.31 | 7.46 ± 4.24 | 0.89 |
| Glucose mg/dL | 90.76 ± 10.26 | 98.77 ± 12.34 | 0.09 |
| Albumin mg/dL | 3.54 ± 1.00 | 3.40 ± 0.69 | 0.69 |
| Chlorine mm/L | 110.17 ± 6.82 | 107.58 ± 2.87 | 0.24 |
| Potassium mm/L | 4.33 ± 1.03 | 4.58 ± 0.97 | 0.56 |
| Phosphorus mm/L | 4.08 ± 0.80 | 3.87 ± 0.82 | 0.54 |
| Calcium mm/L | 2.24 ± 0.26 | 2.32 ± 0.17 | 0.42 |
| Sodium mm/L | 137.75 ± 3.05 | 138.50 ± 3.15 | 0.56 |
| Magnesium mm/L | 0.78 ± 0.13 | 0.83 ± 0.09 | 0.28 |
| Renal function | |||
| Glomerular filtration rate mL/min/1.73 m2 | 79.23 ± 30.97 | 104.48 ± 40.85 | 0.10 |
| Urea mg/dL | 33.60 ± 7.82 | 43.90 ± 18.35 | 0.09 |
| Creatinine mg/dL | 1.16 ± 0.44 | 0.87 ± 0.51 | 0.15 |
| Proteinuria g/L | 2.16 ± 1.62 | 3.33 ± 1.98 | 0.13 |
| Albuminuria mg/24 h | 64.88 ± 88.61 | 126.60 ± 120.85 | 0.17 |
| Urinary creatinine mg/dL | 2.43 ± 2.71 | 1.36 ± 0.30 | 0.19 |
| Hematuria g/L | 42.25 ± 69.89 | 37.08 ± 58.81 | 0.85 |
| Class III N-12 | Class IV N-12 | |||||
|---|---|---|---|---|---|---|
| Baseline | Six-Month Follow-Up | p | Baseline | Six-Month Follow-Up | p | |
| Systemic lupus erythematosus data | ||||||
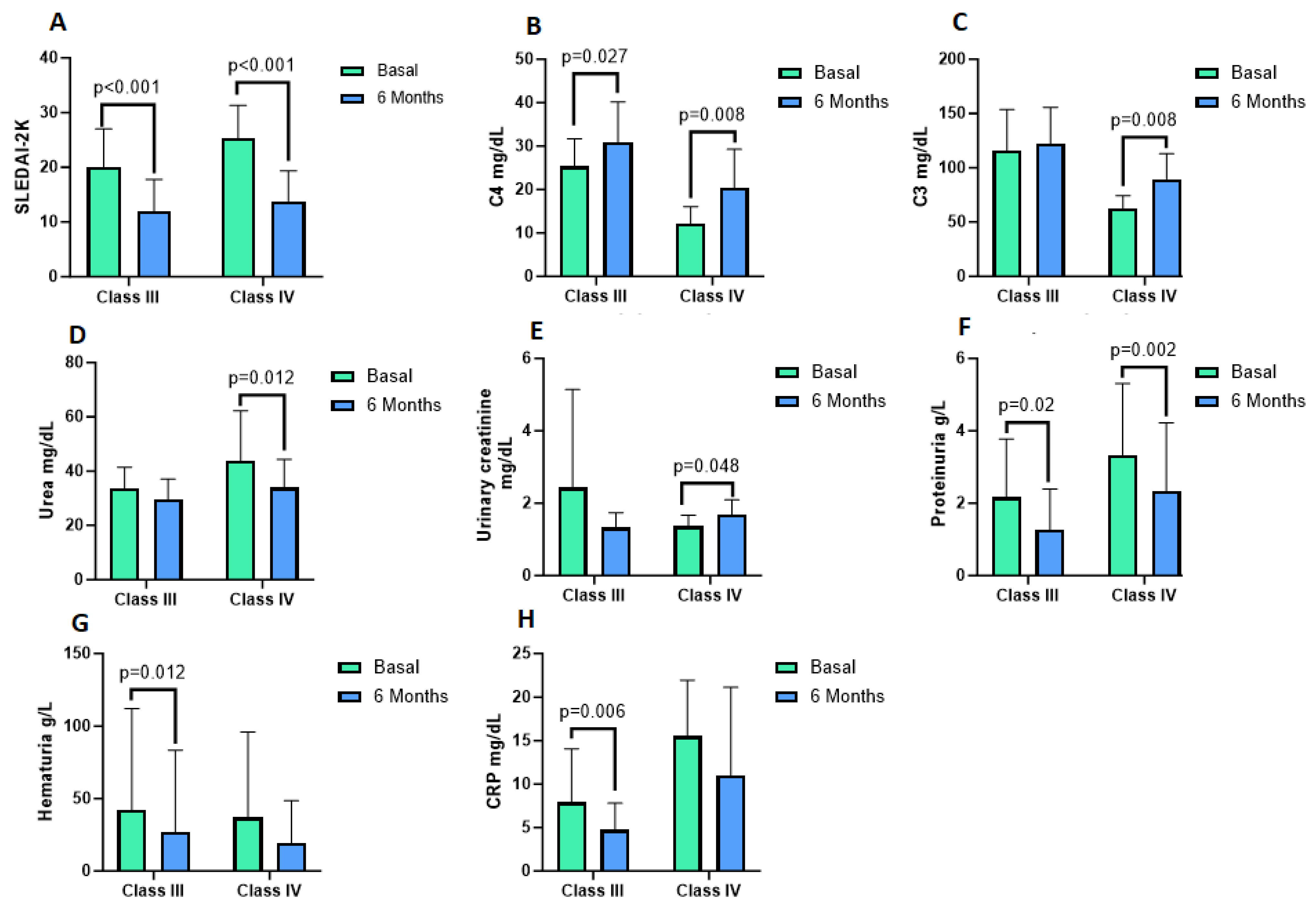
| SLEDAI -2K | 20.08 ± 6.92 | 11.92 ± 5.87 | <0.001 | 25.33 ± 6.01 | 13.83 ± 5.52 | <0.001 |
| C3 mg/dL | 115.97 ± 37.80 | 122.43 ± 33.26 | 0.54 | 62.82 ± 11.40 | 89.64 ± 23.22 | 0.008 |
| C4 mg/dL | 25.36 ± 6.34 | 30.91 ± 9.22 | 0.027 | 12.18 ± 3.90 | 20.33 ± 8.95 | 0.008 |
| Anti DNA IU/mL | 25.12 ± 32.75 | 18.33 ± 17.18 | 0.23 | 73.69 ± 74.69 | 41.72 ± 27.42 | 0.06 |
| Biochemical data | ||||||
| Hemoglobin g/dL | 12.17 ± 2.40 | 13.00 ± 1.63 | 0.12 | 11.23 ± 1.98 | 12.13 ± 1.34 | 0.08 |
| Hematocrit % | 35.04 ± 6.50 | 38.57 ± 7.94 | 0.28 | 35.76 ± 5.41 | 39.29 ± 6.75 | 0.009 |
| Platelets thousands/uL | 260.92 ± 64.19 | 266.67 ± 68.12 | 0.73 | 239.92 ± 98.87 | 269.33 ± 72.79 | 0.22 |
| Leukocytes | 7.67 ± 3.31 | 7.79 ± 2.28 | 0.89 | 7.46 ± 4.24 | 7.99 ± 2.18 | 0.74 |
| Glucose mg/dL | 90.76 ± 10.26 | 89.06 ± 8.75 | 0.56 | 98.77 ± 12.34 | 82.45 ± 9.82 | 0.005 |
| Albumin mg/dL | 3.54 ± 1.00 | 3.67 ± 0.72 | 0.66 | 3.40 ± 0.69 | 3.52 ± 1.00 | 0.61 |
| Chlorine mmol/L | 110.17 ± 6.82 | 103.92 ± 4.78 | 0.007 | 107.58 ± 2.87 | 105.00 ± 3.33 | 0.05 |
| Potassium mm/L | 4.33 ± 1.03 | 4.41 ± 0.51 | 0.76 | 4.58 ± 0.97 | 4.40 ± 0.42 | 0.42 |
| Phosphorus mm/L | 4.08 ± 0.80 | 3.41 ± 1.36 | 0.19 | 3.87 ± 0.82 | 3.27 ± 1.45 | 0.35 |
| Calcium mmol/L | 2.24 ± 0.26 | 2.35 ± 0.15 | 0.14 | 2.32 ± 0.17 | 2.23 ± 0.16 | 0.15 |
| Sodium mmol/L | 137.75 ± 3.05 | 138.33 ± 1.23 | 0.56 | 138.50 ± 3.15 | 140.25 ± 3.25 | 0.09 |
| Magnesium mmol/L | 0.78 ± 0.13 | 0.81 ± 0.12 | 0.27 | 0.83 ± 0.09 | 0.83 ± 0.11 | 0.85 |
| Renal function | ||||||
| Glomerular filtration rate mL/min/1.73 m2 | 79.23 ± 30.97 | 88.55 ± 17.95 | 0.26 | 104.48 ± 40.85 | 104.44 ± 26.47 | 0.99 |
| Urea mg/dL | 33.60 ± 7.82 | 29.65 ± 7.46 | 0.23 | 43.90 ± 18.35 | 33.93 ± 10.46 | 0.012 |
| Creatinine mg/dL | 1.16 ± 0.44 | 0.97 ± 0.25 | 0.15 | 0.87 ± 0.51 | 0.79 ± 0.27 | 0.47 |
| Proteinuria g/L | 2.16 ± 1.62 | 1.26 ± 1.13 | 0.02 | 3.33 ± 1.98 | 2.33 ± 1.89 | 0.002 |
| Albuminuria mg/24 g | 64.88 ± 88.61 | 20.68 ± 20.71 | 0.08 | 126.60 ± 120.85 | 138.92 ± 382.82 | 0.90 |
| Urinary creatinine mg/dL | 2.43 ± 2.71 | 1.16 ± 1.49 | 0.68 | 1.36 ± 0.30 | 1.69 ± 0.41 | 0.048 |
| Hematuria g/L | 42.25 ± 69.89 | 27.00 ± 56.41 | 0.012 | 37.08 ± 58.81 | 19.42 ± 29.11 | 0.11 |
| HC N-12 | Class III N-12 | HC vs. Class III p | Class IV N-12 | HC vs. Class IV p | Class III vs. Class IV p | |
|---|---|---|---|---|---|---|
| Inflammation markers | ||||||
| CRP mg/dL | 7.93 ± 6.14 | 4.72 ± 3.08 | 0.09 | 15.53 ± 6.45 | 10.99 ± 10.17 | 0.08 |
| IL-6 pg/mL | 805.45 ± 260.54 | 545.41 ± 206.32 | 0.02 | 429.34 ± 202.43 | 0.001 | 0.19 |
| Oxidants | ||||||
| Lipoperoxides mM | 0.06 ± 0.01 | 0.54 ± 0.11 | 0.0001 | 0.51 ± 0.12 | 0.0001 | 0.64 |
| Nitrites /nitrates µg/mL | 0.45 ± 0.25 | 0.44 ± 0.19 | 0.89 | 0.38 ± 0.09 | 0.39 | 0.39 |
| Carbonyl groups in proteins µmol | 0.45 ± 0.25 | 4.08 ± 0.58 | 0.0001 | 4.29 ± 0.47 | 0.0001 | 0.35 |
| Antioxidants | ||||||
| Total antioxidant capacity micromol trolox equivalents | 59.22 ± 7.29 | 46.30 ± 17.37 | 0.03 | 53.99 ± 9.97 | 0.16 | 0.19 |
| Catalase KU/mL | 79.16 ± 6.87 | 68.13 ± 15.65 | 0.04 | 64.36 ± 11.56 | 0.001 | 0.51 |
| Superoxide dismutase U/mL | 0.01 ± 0.01 | 0.02 ± 0.01 | 0.29 | 0.019 ± 0.01 | 0.10 | 0.42 |
| Class III N-12 | Class IV N-12 | |||||
|---|---|---|---|---|---|---|
| Baseline | Six-Month | p | Baseline | Six-Month | p | |
| Inflammation markers | ||||||
| CRP mg/dL | 7.93 ± 1.77 | 4.72 ± 3.23 | 0.006 | 15.53 ± 6.45 | 10.99 ± 10.17 | 0.21 |
| IL-6 pg/mL | 545.41 ± 206.32 | 462.84 ± 228.87 | 0.56 | 429.34 ± 202.42 | 471.21 ± 242.43 | 0.79 |
| Oxidants | ||||||
| Lipoperoxides | 0.54 ± 0.11 | 0.49 ± 0.16 | 0.20 | 0.51 ± 0.12 | 0.52 ± 0.09 | 0.61 |
| Nitrites/nitrates | 0.44 ± 0.19 | 0.42 ± 0.18 | 0.65 | 0.38 ± 0.09 | 0.43 ± 0.08 | 0.29 |
| Carbonyl groups in proteins µmol | 4.08 ± 0.58 | 5.16 ± 4.5 | 0.38 | 4.29 ± 0.47 | 4.42 ± 1.59 | 0.78 |
| Antioxidants | ||||||
| Total antioxidant capacidad micromol trolox equivalents | 46.30 ± 17.37 | 52.73 ± 8.95 | 0.26 | 53.99 ± 9.97 | 54.57 ± 16.17 | 0.93 |
| Catalase KU/mL | 68.13 ± 15.65 | 66.72 ± 12.72 | 0.76 | 64.36 ± 11.56 | 65.72 ± 12.13 | 0.71 |
| Superoxide dismutase U/mL | 0.02 ± 0.01 | 0.02 ± 0.01 | 0.18 | 0.02 ± 0.01 | 0.02 ± 0.01 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerrillos-Gutiérrez, J.I.; Medina-Pérez, M.; Andrade-Sierra, J.; De Alba-Razo, A.; Pacheco-Moisés, F.P.; Cardona-Muñoz, E.G.; Campos-Pérez, W.; Martínez-López, E.; Sánchez-Lozano, D.I.; García-Sánchez, A.; et al. The Inflammatory and Oxidative Status of Newly Diagnosed Class III and Class IV Lupus Nephritis, with Six-Month Follow-Up. Antioxidants 2023, 12, 2065. https://doi.org/10.3390/antiox12122065
Cerrillos-Gutiérrez JI, Medina-Pérez M, Andrade-Sierra J, De Alba-Razo A, Pacheco-Moisés FP, Cardona-Muñoz EG, Campos-Pérez W, Martínez-López E, Sánchez-Lozano DI, García-Sánchez A, et al. The Inflammatory and Oxidative Status of Newly Diagnosed Class III and Class IV Lupus Nephritis, with Six-Month Follow-Up. Antioxidants. 2023; 12(12):2065. https://doi.org/10.3390/antiox12122065
Chicago/Turabian StyleCerrillos-Gutiérrez, José Ignacio, Miguel Medina-Pérez, Jorge Andrade-Sierra, Alejandra De Alba-Razo, Fermín Paul Pacheco-Moisés, Ernesto Germán Cardona-Muñoz, Wendy Campos-Pérez, Erika Martínez-López, Daniela Itzel Sánchez-Lozano, Andrés García-Sánchez, and et al. 2023. "The Inflammatory and Oxidative Status of Newly Diagnosed Class III and Class IV Lupus Nephritis, with Six-Month Follow-Up" Antioxidants 12, no. 12: 2065. https://doi.org/10.3390/antiox12122065