
Comparison of the Pulmonary Oxidative Stress Caused by Intratracheal Instillation and Inhalation of NiO Nanoparticles when Equivalent Amounts of NiO Are Retained in the Lung

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. NiO Nanoparticles
2.2. Animals
2.3. Intratracheal Instillation
2.4. Inhalation
2.5. Measurement of Oxidative Stress-Related Proteins
2.6. Measurement of Gene Expression
3. Results and Discussion
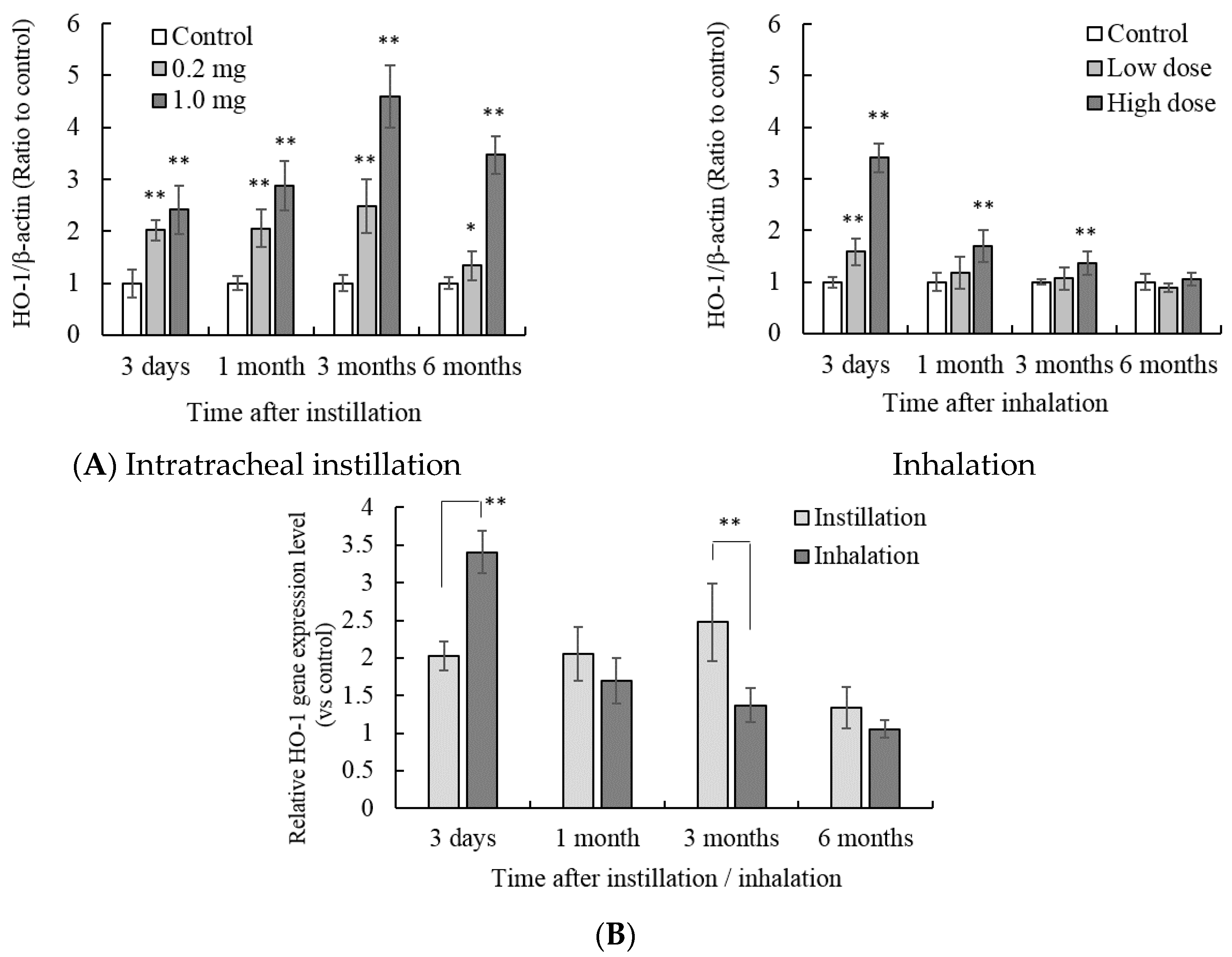
3.1. HO-1 Protein and Gene Expression in the Lung Tissue


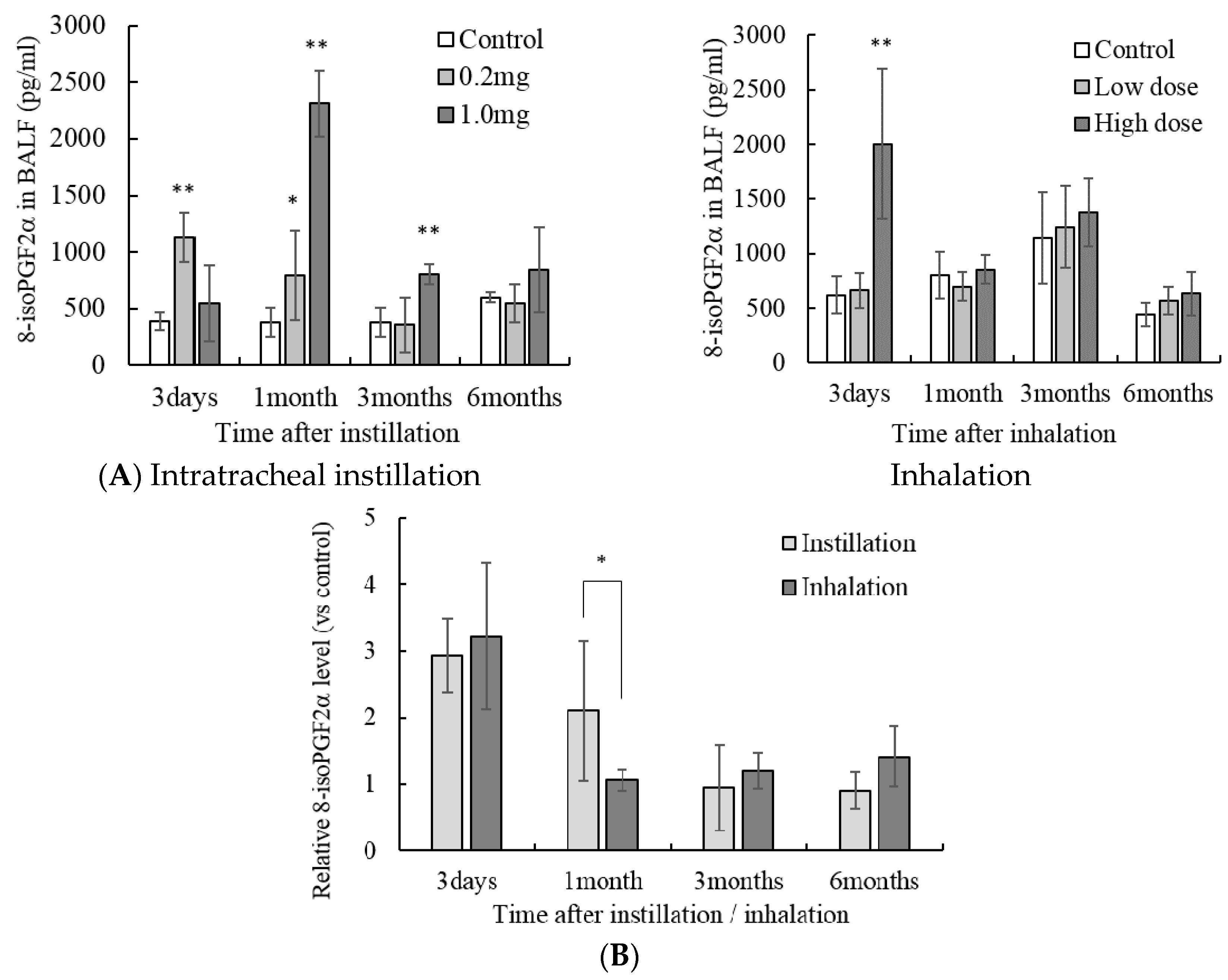
3.2. Concentration of Lipid Peroxide in the Lung Tissue

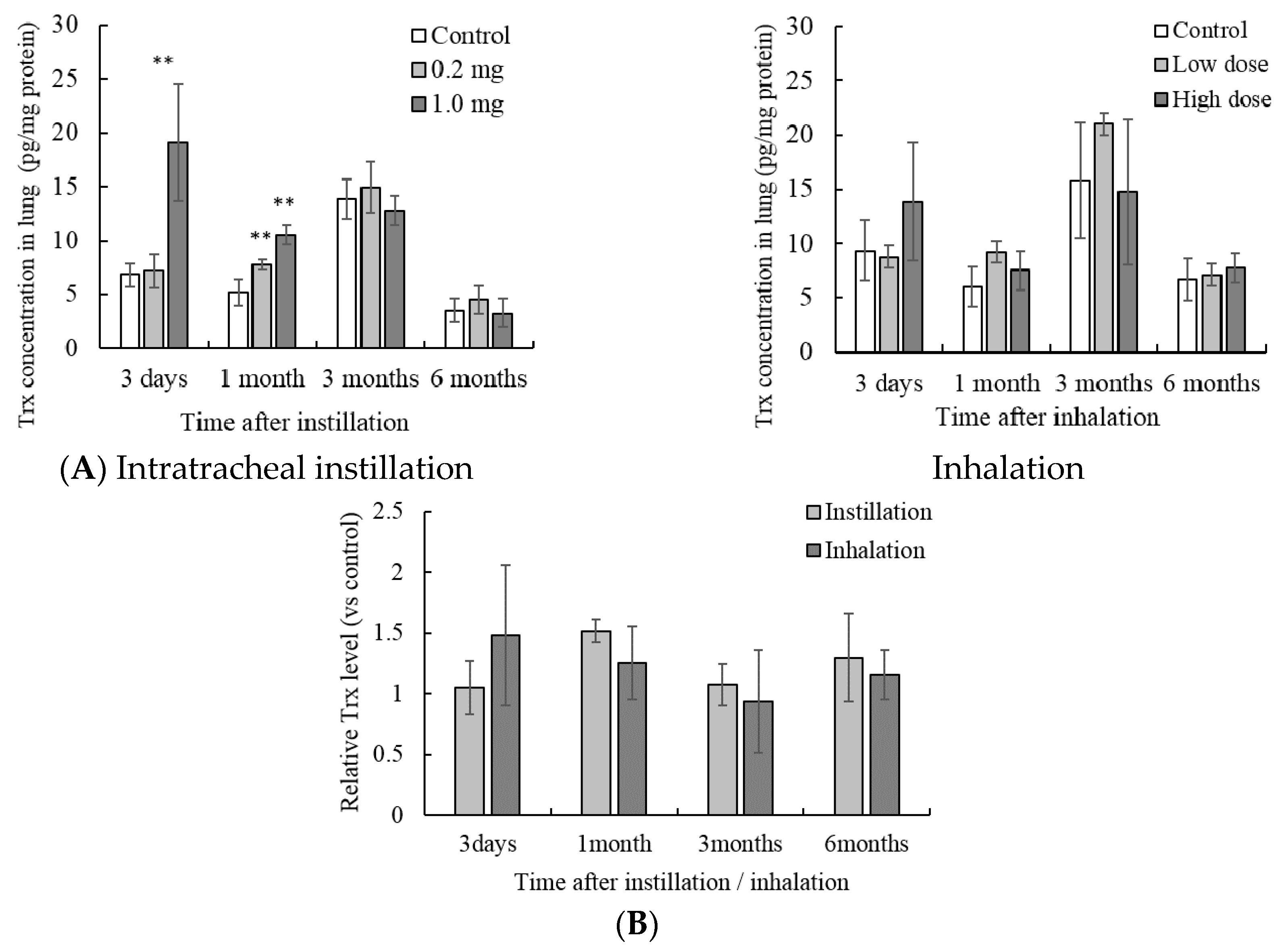
3.3. Concentration of Trx in the Lung Tissue

3.4. Gene Expression of Inducible Nitric Oxide Synthase (iNos) in the Lung Tissue
3.5. Concentration of MPO in the Lung Tissue


3.6. Gene Expression of MT in the Lung Tissue


4. Conclusions

Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brain, J.D.; Knudson, D.E.; Sorokin, S.P.; Davis, M.A. Pulmonary distribution of particles given by intratracheal instillation or by aerosol inhalation. Environ. Res. 1976, 11, 13–33. [Google Scholar] [CrossRef]
- Pritchard, J.N.; Holmes, A.; Evans, J.C.; Evans, N.; Evans, R.J.; Morgan, A. The distribution of dust in the rat lung following administration by inhalation and by single intratracheal instillation. Environ. Res. 1985, 36, 268–297. [Google Scholar] [CrossRef]
- Damon, E.G.; Halliwell, W.H.; Henderson, T.R.; Mokler, B.V.; Jones, R.K. Acute toxicity of polyethylene glycol p-isooctylphenol ether in syrian hamsters exposed by inhalation or bronchopulmonary lavage. Toxicol. Appl. Pharmacol. 1982, 63, 53–61. [Google Scholar] [CrossRef]
- Drew, R.T.; Kuschner, M.; Bernstein, D.M. The chronic effects of exposure of rats to sized glass fibres. Ann. Occup. Hyg. 1987, 31, 711–729. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, K.E.; Lindenschmidt, R.C.; Maurer, J.K.; Higgins, J.M.; Ridder, G. Pulmonary response to silica or titanium dioxide: Inflammatory cells, alveolar macrophage-derived cytokines, and histopathology. Am. J. Respir. Cell Mol. Biol. 1990, 2, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, K.E.; Maurer, J.K.; Lindenschmidt, R.C.; Romberger, D.; Rennard, S.I.; Crosby, L. Respiratory tract responses to dust: Relationships between dust burden, lung injury, alveolar macrophage fibronectin release, and the development of pulmonary fibrosis. Toxicol. Appl. Pharmacol. 1990, 106, 88–101. [Google Scholar] [CrossRef]
- Driscoll, K.E.; Lindenschmidt, R.C.; Maurer, J.K.; Perkins, L.; Perkins, M.; Higgins, J. Pulmonary response to inhaled silica or titanium dioxide. Toxicol. Appl. Pharmacol. 1991, 111, 201–210. [Google Scholar] [CrossRef]
- Morimoto, Y.; Izumi, H.; Yoshiura, Y.; Tomonaga, T.; Lee, B.W.; Okada, T.; Oyabu, T.; Myojo, T.; Kawai, K.; Yatera, K.; et al. Comparison of pulmonary inflammatory responses following intratracheal instillation and inhalation of nanoparticles. Nanotoxicology 2015, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Horie, M.; Fukui, H.; Nishio, K.; Endoh, S.; Kato, H.; Fujita, K.; Miyauchi, A.; Nakamura, A.; Shichiri, M.; Ishida, N.; et al. Evaluation of acute oxidative stress induced by NiO nanoparticles in vivo and in vitro. J. Occup. Health 2011, 53, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Horie, M.; Fukui, H.; Endoh, S.; Maru, J.; Miyauchi, A.; Shichiri, M.; Fujita, K.; Niki, E.; Hagihara, Y.; Yoshida, Y.; et al. Comparison of acute oxidative stress on rat lung induced by nano and fine-scale, soluble and insoluble metal oxide particles: NiO and TiO2. Inhal. Toxicol. 2012, 24, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Horie, M.; Endoh, S.; Kato, H.; Fujita, K.; Nishio, K.; Komaba, L.K.; Maru, J.; Miyauhi, A.; Nakamura, A.; et al. Association of zinc ion release and oxidative stress induced by intratracheal instillation of ZnO nanoparticles to rat lung. Chem. Biol. Interact. 2012, 198, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Nakaoka, A.; Morimoto, K.; Shimada, M.; Horie, M.; Morimoto, Y.; Sasaki, T. Aerosol Generation by a Spray-Drying Technique Under Coulomb Explosion and Rapid Evaporation for the Preparation of Aerosol Particles for Inhalation Tests. Aerosol Sci. Technol. 2014, 48, 698–705. [Google Scholar] [CrossRef]
- Niki, E. STRESS: Science and Health; Kyoritsu Shuppan Co., Ltd.: Tokyo, Japan, 2008; pp. 2–7. [Google Scholar]
- Beck-Speier, I.; Dayal, N.; Karg, E.; Maier, K.L.; Schumann, G.; Schulz, H.; Semmler, M.; Takenaka, S.; Stettmaier, K.; Bors, W.; et al. Oxidative stress and lipid mediators induced in alveolar macrophages by ultrafine particles. Free Radic. Biol. Med. 2005, 38, 1080–1092. [Google Scholar] [CrossRef] [PubMed]
- Nauseef, W.M. Myeloperoxidase in human neutrophil host defence. Cell Microbiol. 2014, 16, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Ohta, Y.; Akiyama, K.; Tokunaga, K. Study of oxidative damage by myeloperoxidase derived reactive oxygen. J. Anal. Bio-Sci. 2012, 35, 133–139. [Google Scholar]
- Zhang, B.; Georgiev, O.; Hagmann, M.; Günes, C.; Cramer, M.; Faller, P.; Vasák, M.; Schaffner, W. Activity of metal-responsive transcription factor 1 by toxic heavy metals and H2O2 in vitro is modulated by metallothionein. Mol. Cell. Biol. 2003, 23, 8471–8485. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.K. Regulation of metallothionein gene expression by oxidative stress and metal ions. Biochem. Pharmacol. 2000, 59, 95–104. [Google Scholar] [CrossRef]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horie, M.; Yoshiura, Y.; Izumi, H.; Oyabu, T.; Tomonaga, T.; Okada, T.; Lee, B.-W.; Myojo, T.; Kubo, M.; Shimada, M.; et al. Comparison of the Pulmonary Oxidative Stress Caused by Intratracheal Instillation and Inhalation of NiO Nanoparticles when Equivalent Amounts of NiO Are Retained in the Lung. Antioxidants 2016, 5, 4. https://doi.org/10.3390/antiox5010004
Horie M, Yoshiura Y, Izumi H, Oyabu T, Tomonaga T, Okada T, Lee B-W, Myojo T, Kubo M, Shimada M, et al. Comparison of the Pulmonary Oxidative Stress Caused by Intratracheal Instillation and Inhalation of NiO Nanoparticles when Equivalent Amounts of NiO Are Retained in the Lung. Antioxidants. 2016; 5(1):4. https://doi.org/10.3390/antiox5010004
Chicago/Turabian StyleHorie, Masanori, Yukiko Yoshiura, Hiroto Izumi, Takako Oyabu, Taisuke Tomonaga, Takami Okada, Byeong-Woo Lee, Toshihiko Myojo, Masaru Kubo, Manabu Shimada, and et al. 2016. "Comparison of the Pulmonary Oxidative Stress Caused by Intratracheal Instillation and Inhalation of NiO Nanoparticles when Equivalent Amounts of NiO Are Retained in the Lung" Antioxidants 5, no. 1: 4. https://doi.org/10.3390/antiox5010004