
Identification of Barriers Limiting the Use of Preventive Vaccinations against Influenza among the Elderly Population: A Cross-Sectional Analysis


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- Z1−a/2 is the standard normal variate (at 5% type 1 error p < 0.05), −1.96;
- p is the expected prevalence obtained from a pilot study, −0.4; and d is the absolute precision, −0.04.
2.2. Explanatory Variables
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Sociodemographic, Clinical and Mental Factors Have an Impact on Attitudes toward Preventive Influenza Vaccination
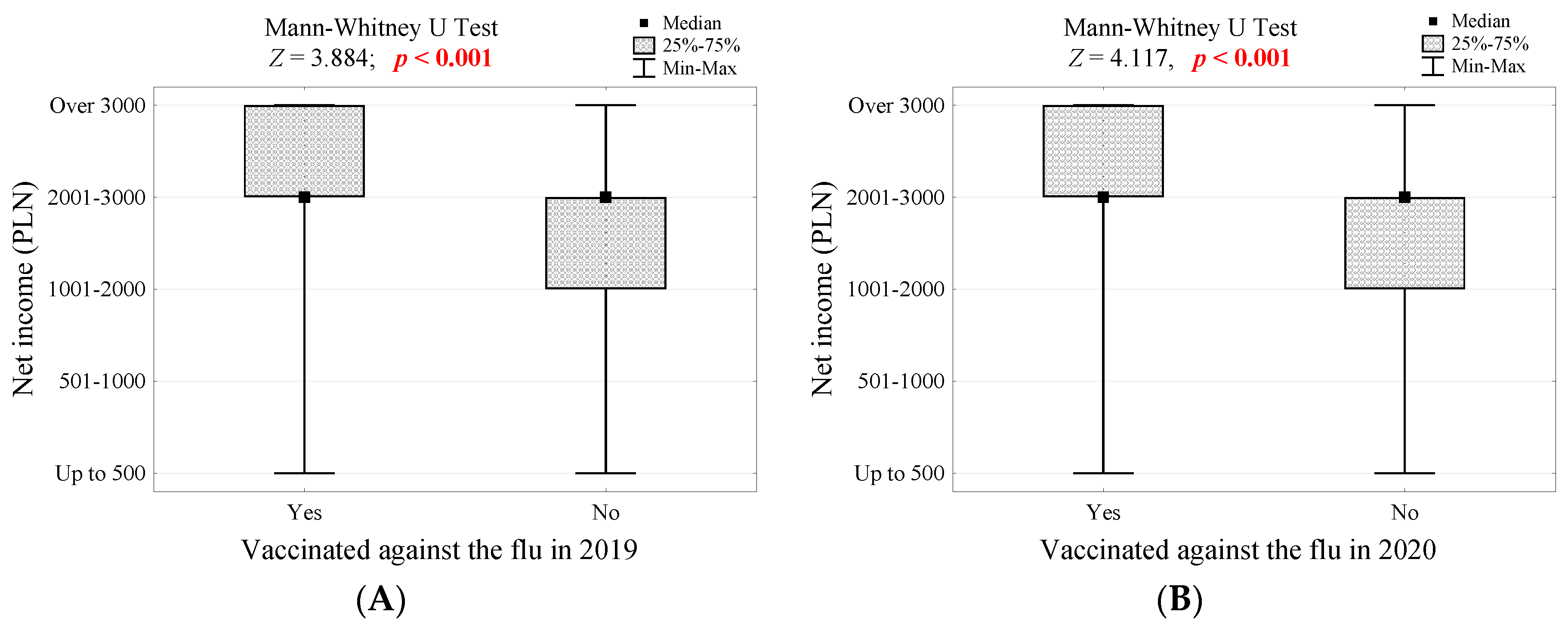
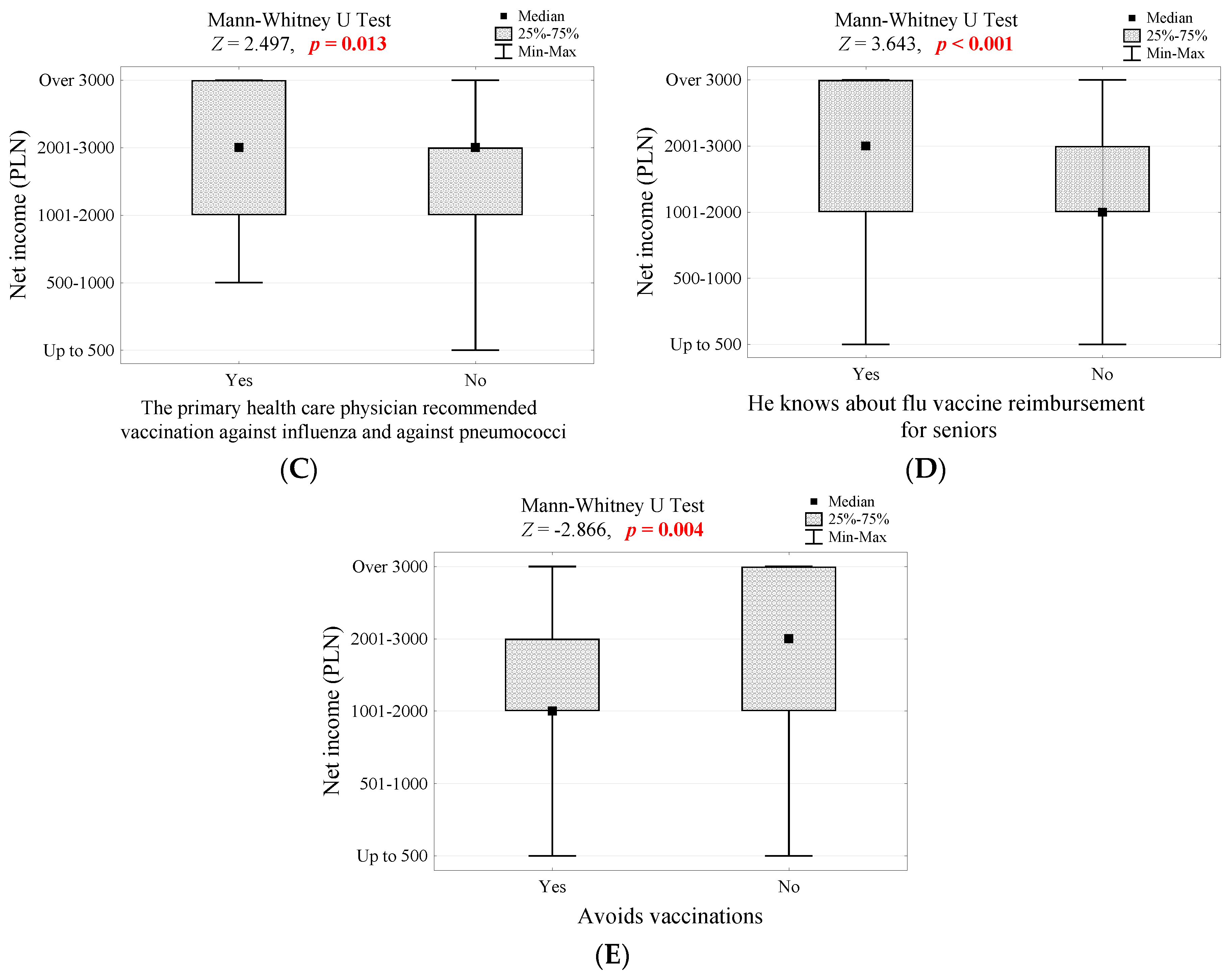
3.3. Net Income
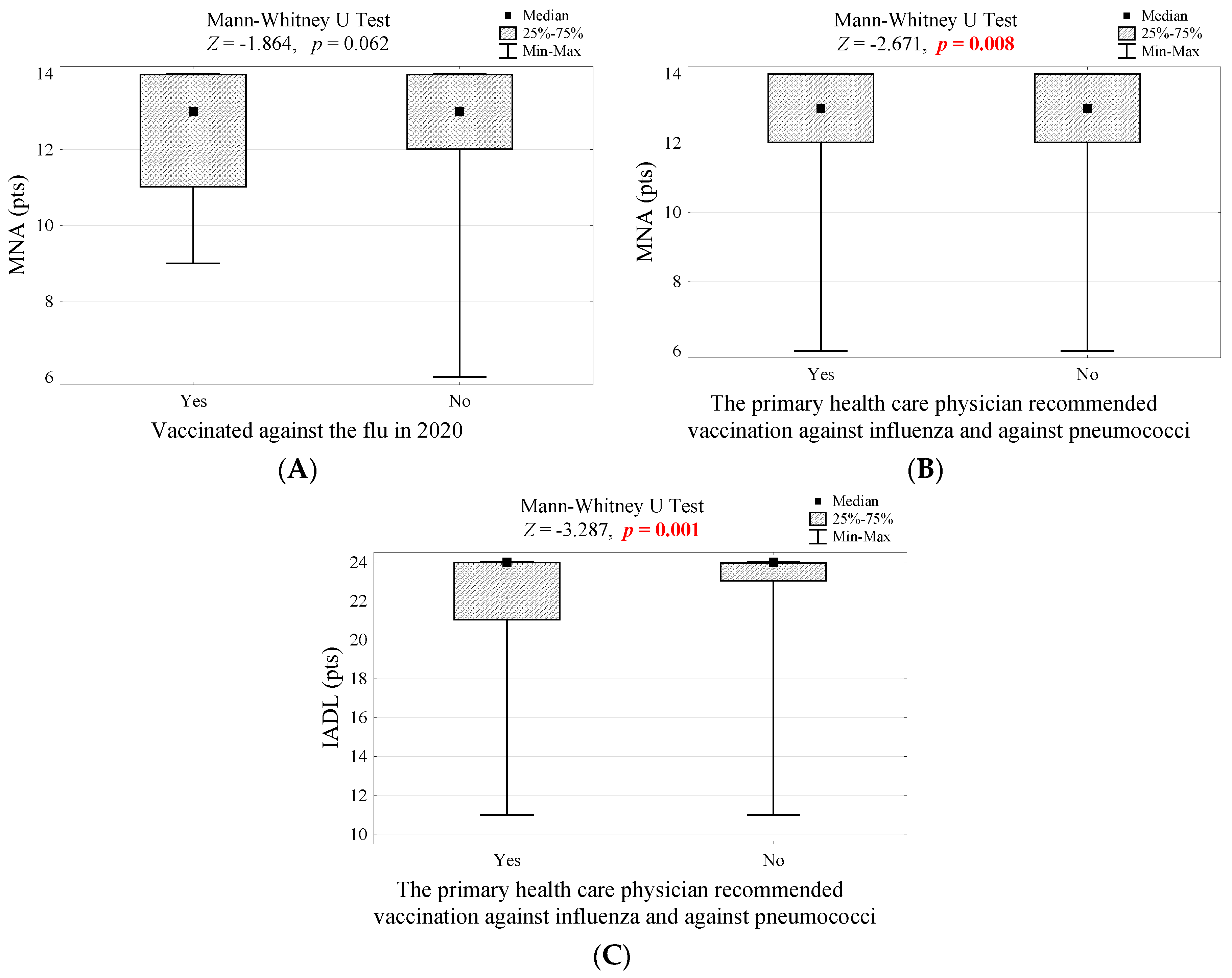
3.4. Mental Health Conditions
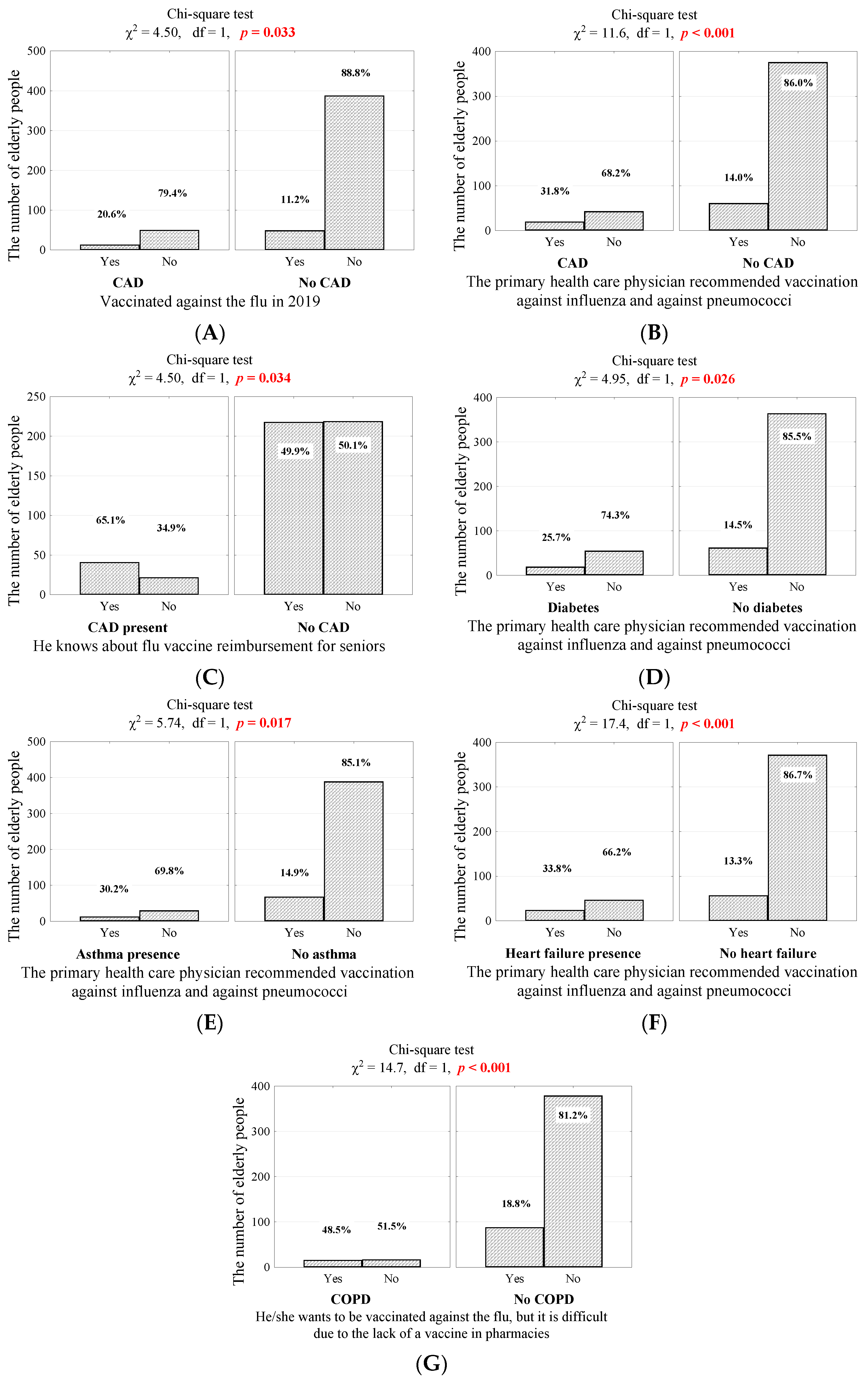
3.5. Chronic Diseases
3.6. Fear of COVID-19 Infection as a Factor Determining Attitudes toward Preventive Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Influenza (Seasonal), Fact Sheet. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 16 February 2022).
- Macias, A.E.; McElhaney, J.E.; Chaves, S.S.; Nealon, J.; Nunes, M.C.; Samson, S.I.; Seet, B.T.; Weinke, T.; Yu, H. The disease burden of influenza beyond respiratory illness. Vaccine 2021, 39 (Suppl. S1), A6–A14. [Google Scholar] [CrossRef]
- Paget, J.; Spreeuwenberg, P.; Charu, V.; Taylor, R.J.; Iuliano, A.D.; Bresee, J.; Simonsen, L.; Viboud, C. Global Seasonal Influenza-associated Mortality Collaborator Network and GLaMOR Collaborating Teams. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J. Glob. Health 2019, 9, 020421. [Google Scholar] [CrossRef]
- Costantino, C.; Vitale, F. Influenza vaccination in high-risk groups: A revision of existing guidelines and rationale for an evidence-based preventive strategy. J. Prev. Med. Hyg. 2016, 57, E13–E18. [Google Scholar]
- OECD Health Care Use—Influenza Vaccination Rates—OECD Data. Available online: https://data.oecd.org/healthcare/influenza-vaccination-rates.htm (accessed on 16 February 2022).
- Del Riccio, M.; Lina, B.; Caini, S.; Staadegaard, L.; Sytske, W.; Kynčl, J.; Combadière, B.; MacIntyre Chandini, R.; Paget, J. Letter to the editor: Increase of influenza vaccination coverage rates during the COVID-19 pandemic and implications for the upcoming influenza season in northern hemisphere countries and Australia. Eurosurveillance 2021, 26, 2101143. [Google Scholar] [CrossRef]
- Statista. Poland: Number of Influenza Vaccinations 2020|Statista. Available online: https://www.statista.com/statistics/1086732/poland-number-of-influenza-vaccinations/ (accessed on 16 February 2022).
- Jaki Jest Stan Zaszczepienia Przeciw Odrze W Polsce? Available online: https://szczepienia.pzh.gov.pl/faq/jaki-jest-poziom-zaszczepienia-przeciw-grypie-w-polsce/ (accessed on 16 February 2022).
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar]
- Bridges, C.B.; Thompson, W.W.; Meltzer, M.I.; Reeve, G.R.; Talamonti, W.J.; Cox, N.J.; Lilac, H.A.; Hall, H.; Klimov, A.; Fukuda, K. Effectiveness and cost-benefit of influenza vaccination of healthy working adults: A randomized controlled trial. JAMA 2000, 284, 1655–1663. [Google Scholar] [CrossRef] [Green Version]
- Nichol, K.L.; Margolis, K.L.; Lind, A.; Murdoch, M.; McFadden, R.; Hauge, M.; Magnan, S.; Drake, M. Side effects associated with influenza vaccination in healthy working adults. A randomized, placebo-controlled trial. Arch. Intern. Med. 1996, 156, 1546–1550. [Google Scholar] [CrossRef]
- Rome, B.N.; Feldman, W.B.; Fischer, M.A.; Desai, R.J.; Avorn, J. Influenza Vaccine Uptake in the Year After Concurrent vs Separate Influenza and Zoster Immunization. JAMA Netw. Open 2021, 4, e2135362. [Google Scholar] [CrossRef]
- Yan, S.; Wang, Y.; Zhu, W.; Zhang, L.; Gu, H.; Liu, D.; Zhu, A.; Xu, H.; Hao, L.; Ye, C. Barriers to influenza vaccination among different populations in Shanghai. Hum. Vaccines Immunother. 2021, 17, 1403–1411. [Google Scholar] [CrossRef]
- Trent, M.J.; Salmon, D.A.; MacIntyre, C.R. Predictors of pneumococcal vaccination among Australian adults at high risk of pneumococcal disease. Vaccine 2022, 40, 1152–1161. [Google Scholar] [CrossRef]
- Nicholls, L.A.B.; Gallant, A.J.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Older adults’ vaccine hesitancy: Psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine 2021, 39, 3520–3527. [Google Scholar] [CrossRef] [PubMed]
- Kałucka, S.; Dziankowska-Zaborszczyk, E.; Grzegorczyk-Karolak, I.; Głowacka, A. A comparison of the attitudes to influenza vaccination held by nursing, midwifery, pharmacy, and public health students and their knowledge of viral infections. Vaccines 2020, 8, 516. [Google Scholar] [CrossRef] [PubMed]
- Kałucka, S.; Głowacka, A.; Dziankowska-Zaborszczyk, E.; Grzegorczyk-Karolak, I. Knowledge, beliefs and attitudes towards the influenza vaccine among future healthcare workers in poland. Int. J. Environ. Res. Public Health 2021, 18, 2105. [Google Scholar] [CrossRef]
- Czajka, H.; Czajka, S.; Biłas, P.; Pałka, P.; Jędrusik, S.; Czapkiewicz, A. Who or what influences the individuals’ decision-making process regarding vaccinations? Int. J. Environ. Res. Public Health 2020, 17, 4461. [Google Scholar] [CrossRef]
- Nessler, K.; Krztoń-Królewiecka, A.; Chmielowiec, T.; Jarczewska, D.; Windak, A. Determinants of influenza vaccination coverage rates among primary care patients in Krakow, Poland and the surrounding region. Vaccine 2014, 32, 7122–7127. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Cori, L.; Curzio, O.; Adorni, F.; Prinelli, F.; Noale, M.; Trevisan, C.; Fortunato, L.; Giacomelli, A.; Bianchi, F. Fear of COVID-19 for individuals and family members: Indications from the national cross-sectional study of the epicovid19 web-based survey. Int. J. Environ. Res. Public Health 2021, 18, 3248. [Google Scholar] [CrossRef]
- Agrawal, S.; Makuch, S.; Dróżdż, M.; Strzelec, B.; Sobieszczańska, M.; Mazur, G. The impact of the COVID-19 emergency on life activities and delivery of healthcare services in the elderly population. J. Clin. Med. 2021, 10, 4089. [Google Scholar] [CrossRef]
- Agrawal, S.; Dróżdż, M.; Makuch, S.; Pietraszek, A.; Sobieszczańska, M.; Mazur, G. The assessment of fear of COVID-19 among the elderly population: A cross-sectional study. J. Clin. Med. 2021, 10, 5537. [Google Scholar] [CrossRef]
- Graeber, D.; Schmidt-Petri, C.; Schröder, C. Attitudes on voluntary and mandatory vaccination against COVID-19: Evidence from Germany. PLoS ONE 2021, 16, e0248372. [Google Scholar] [CrossRef]
- Teo, L.M.; Smith, H.E.; Lwin, M.O.; Tang, W.E. Attitudes and perception of influenza vaccines among older people in Singapore: A qualitative study. Vaccine 2019, 37, 6665–6672. [Google Scholar] [CrossRef]
- Lucyk, K.; Simmonds, K.A.; Lorenzetti, D.L.; Drews, S.J.; Svenson, L.W.; Russell, M.L. The association between influenza vaccination and socioeconomic status in high income countries varies by the measure used: A systematic review. BMC Med. Res. Methodol. 2019, 19, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Mamelund, S.E.; Shelley-Egan, C.; Rogeberg, O. The association between socioeconomic status and pandemic influenza: Systematic review and meta-analysis. PLoS ONE 2021, 16, e0244346. [Google Scholar] [CrossRef]
- Główny Inspektor Sanitarny Dziennik Urzędowy Ministra Zdrowia. Available online: http://dziennikmz.mz.gov.pl/legalact/2021/65/ (accessed on 16 February 2022).
- Ministerstwo Zdrowia, Możliwość Zaszczepienia Się Przez Skorzystanie Z: Refundacji Szczepionek W Aptece, Programu Samorządowego Lub Świadczenia Komercyjnego. 2021. Available online: https://www.gov.pl/web/zdrowie/mozliwosc-zaszczepienia-sie-przez-skorzystanie-z-refundacji-szczepionek-w-aptece-programu-samorzadowego-lub-swiadczenia-komercyjnego (accessed on 7 March 2022).
- Samel-Kowalik, P.; Jankowski, M.; Lisiecka-Biełanowicz, M.; Ostrowska, A.; Gujski, M.; Kobuszewski, B.; Pinkas, J.; Raciborski, F. Factors associated with attitudes towards seasonal influenza vaccination in poland: A nationwide cross-sectional survey in 2020. Vaccines 2021, 9, 1336. [Google Scholar] [CrossRef]
- Dz. U. 2008 Nr 234 Poz.1570 Ustawa Z Dnia 5 Grudnia 2008 R. O Zapobieganiu Oraz Zwalczaniu Zakażeń I Chorób Zakaźnych U Ludzi. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20082341570 (accessed on 7 March 2022).
- Rozporządzenie Ministra Zdrowia Z Dnia 18 Listopada 2021 R. Zmieniające Rozporządzenie W Sprawie Metody Zapobiegania Grypie Sezonowej W Sezonie 2021/2022. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20210002098 (accessed on 7 March 2022).
- Czech, M.; Balcerzak, M.; Antczak, A.; Byliniak, M.; Piotrowska-Rutkowska, E.; Drozd, M.; Juszczyk, G.; Religioni, U.; Vaillacourt, R.; Merks, P. Flu vaccinations in pharmacies—a review of pharmacists fighting pandemics and infectious diseases. Int. J. Environ. Res. Public Health 2020, 17, 7945. [Google Scholar] [CrossRef]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A.; Chung, H.; Crowcroft, N.S.; Karnauchow, T.; Katz, K.; Ko, D.T.; McGeer, A.J.; McNally, D.; et al. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. N. Engl. J. Med. 2018, 378, 345–353. [Google Scholar] [CrossRef]
- Dobrzynski, D.M.; Ndi, D.N.; Zhu, Y.; Markus, T.; Schaffner, W.; Keipp Talbot, H. Hospital readmissions after laboratory-confirmed influenza hospitalization. J. Infect. Dis. 2020, 222, 583–589. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Gaglani, M.; Martin, E.T.; Middleton, D.; Monto, A.S.; Murthy, K.; Silveira, F.P.; Talbot, H.K.; Zimmerman, R.; Alyanak, E.; et al. Prevention of Influenza Hospitalization among Adults in the United States, 2015–2016: Results from the US Hospitalized Adult Influenza Vaccine Effectiveness Network (HAIVEN). J. Infect. Dis. 2019, 220, 1265–1275. [Google Scholar] [CrossRef]
- Cheng, Y.; Cao, X.; Cao, Z.; Xu, C.; Sun, L.; Gao, Y.; Wang, Y.; Li, S.; Wu, C.; Li, X.; et al. Effects of influenza vaccination on the risk of cardiovascular and respiratory diseases and all-cause mortality. Ageing Res. Rev. 2020, 62, 101124. [Google Scholar] [CrossRef]
- Shen, S.; Dubey, V. Addressing vaccine hesitancy. Can. Fam. Physician 2019, 65, 175–181. [Google Scholar]
- Kharroubi, G.; Cherif, I.; Bouabid, L.; Gharbi, A.; Boukthir, A.; Ben Alaya, N.; Ben Salah, A.; Bettaieb, J. Influenza vaccination knowledge, attitudes, and practices among Tunisian elderly with chronic diseases. BMC Geriatr. 2021, 21, 700. [Google Scholar] [CrossRef]
- Tuckerman, J.; Crawford, N.W.; Marshall, H.S. Disparities in parental awareness of children’s seasonal influenza vaccination recommendations and influencers of vaccination. PLoS ONE 2020, 15, e0230425. [Google Scholar] [CrossRef] [Green Version]
- Maher, L.; Hope, K.; Torvaldsen, S.; Lawrence, G.; Dawson, A.; Wiley, K.; Thomson, D.; Hayen, A.; Conaty, S. Influenza vaccination during pregnancy: Coverage rates and influencing factors in two urban districts in Sydney. Vaccine 2013, 31, 5557–5564. [Google Scholar] [CrossRef]
- Stańczak-Mrozek, K.I.; Sobczak, A.; Lipiński, L.; Sienkiewicz, E.; Makarewicz, D.; Topór-Mądry, R.; Pinkas, J.; Sierpiński, R.A. The potential benefits of the influenza vaccination on COVID-19 mortality rate—A retrospective analysis of patients in Poland. Vaccines 2022, 10, 5. [Google Scholar] [CrossRef]
- Yang, M.J.; Rooks, B.J.; Le, T.T.T.; Santiago, I.O.; Diamond, J.; Dorsey, N.L.; Mainous, A.G. Influenza Vaccination and Hospitalizations among COVID-19 Infected Adults. J. Am. Board Fam. Med. 2021, 34, S179–S182. [Google Scholar] [CrossRef]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.S.; Daubenberger, C.; Brentani, A. Inactivated trivalent influenza vaccination is associated with lower mortality among patients with COVID-19 in Brazil. BMJ Evid.-Based Med. 2021, 26, 192–193. [Google Scholar] [CrossRef]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control 2021, 49, 694–700. [Google Scholar] [CrossRef]
- Martínez-Baz, I.; Trobajo-Sanmartín, C.; Arregui, I.; Navascués, A.; Adelantado, M.; Indurain, J.; Fresán, U.; Ezpeleta, C.; Castilla, J. Influenza vaccination and risk of sars-cov-2 infection in a cohort of health workers. Vaccines 2020, 8, 611. [Google Scholar] [CrossRef]
- Kissling, E.; Hooiveld, M.; Brytting, M.; Vilcu, A.M.; de Lange, M.; Martínez-Baz, I.; Sigerson, D.; Enkirch, T.; Belhillil, S.; Meijer, A.; et al. Absence of association between 2019-20 influenza vaccination and COVID-19: Results of the European I-MOVE-COVID-19 primary care project, March-August 2020. Influenza Other Respi. Viruses 2021, 15, 429–438. [Google Scholar] [CrossRef]
- Wehenkel, C. Positive association between COVID-19 deaths and influenza vaccination rates in elderly people worldwide. PeerJ 2020, 8, e10112. [Google Scholar] [CrossRef]
- Wang, R.; Liu, M.; Liu, J. The association between influenza vaccination and COVID-19 and its outcomes: A systematic review and meta-analysis of observational studies. Vaccines 2021, 9, 529. [Google Scholar] [CrossRef] [PubMed]
- Skrinda, I.; Krama, T.; Kecko, S.; Moore, F.R.; Kaasik, A.; Meija, L.; Lietuvietis, V.; Rantala, M.J.; Krams, I. Body height, immunity, facial and vocal attractiveness in young men. Naturwissenschaften 2014, 101, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Krams, I.; Skrinda, I.; Kecko, S. Body height affects the strength of immune response in young men, but not young women. Sci. Rep. 2014, 4, srep6223. [Google Scholar] [CrossRef] [Green Version]
- Pawłowski, B.; Nowak, J.; Borkowska, B.; Augustyniak, D.; Drulis-Kawa, Z. Body height and immune efficacy: Testing body stature as a signal of biological quality. Proc. R. Soc. B Biol. Sci. 2017, 284, 20171372. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Attitude toward Vaccination | |||||
|---|---|---|---|---|---|---|
| A | B | C | D | E | F | |
| Gender (1—women, 0—man) | −0.024 | 0.032 | 0.025 | −0.053 | −0.066 | −0.024 |
| Age (years) | −0.008 | −0.080 | −0.023 | 0.013 | 0.009 | −0.008 |
| Number of inhabitants in the place of residence | 0.055 | 0.023 | −0.007 | 0.098 | −0.007 | 0.055 |
| Number of household members | 0.020 | −0.015 | −0.026 | 0.004 | 0.080 | 0.020 |
| Level of education (1—basic, …, 4—higher) | −0.021 | 0.034 | −0.011 | 0.017 | −0.047 | −0.021 |
| Income (PLN) | 0.186 | 0.165 | −0.108 | 0.041 | 0.100 | 0.179 |
| Body weight (kg) | 0.034 | −0.003 | −0.053 | 0.043 | 0.051 | 0.034 |
| Body height (cm) | 0.068 | −0.007 | −0.111 | 0.101 | 0.080 | 0.053 |
| BMI (kg/m2) | −0.009 | 0.003 | 0.014 | −0.012 | 0.009 | −0.009 |
| Satisfaction with medical care (0–10) | 0.021 | −0.011 | −0.085 | 0.087 | 0.092 | 0.048 |
| ADL (pts) | −0.043 | −0.038 | 0.042 | 0.012 | 0.027 | −0.043 |
| IADL (pts) | −0.082 | −0.058 | 0.014 | −0.047 | −0.178 | −0.082 |
| AMTS (pts) | 0.044 | 0.003 | −0.064 | 0.070 | 0.023 | 0.044 |
| GDS-15 (pts) | −0.068 | −0.021 | 0.041 | −0.011 | 0.049 | −0.068 |
| GAS-10 (pts) | 0.004 | 0.061 | 0.021 | −0.024 | 0.082 | 0.004 |
| LSNS-6 (pts) | 0.033 | −0.031 | 0.001 | 0.043 | −0.030 | 0.033 |
| GLS (pts) | −0.063 | −0.081 | −0.017 | −0.024 | −0.094 | −0.063 |
| MNA (pts) | −0.041 | −0.097 | 0.043 | 0.045 | −0.123 | −0.041 |
| Fear of COVID-19 (pts) | 0.056 | 0.062 | 0.070 | 0.134 | 0.168 | −0.022 |
| Coronary artery disease | 0.095 | 0.071 | 0.017 | 0.088 | 0.160 | 0.095 |
| Diabetes | 0.014 | 0.008 | 0.057 | −0.075 | 0.107 | 0.014 |
| Asthma | 0.014 | 0.085 | 0.074 | −0.017 | 0.117 | 0.014 |
| COPD | 0.022 | −0.010 | −0.048 | 0.181 | 0.080 | 0.022 |
| Heart failure | 0.038 | 0.033 | 0.009 | 0.060 | 0.194 | 0.038 |
| Kidney failure | −0.015 | −0.001 | 0.075 | −0.054 | −0.034 | −0.015 |
| GERD | 0.045 | 0.040 | 0.009 | 0.070 | 0.158 | 0.044 |
| Risk Factors for Negative Attitude to Vaccination (NAV) | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|
| Attitude to Vaccination | p | OR (95% CI) | Beta | OR | ||||
| Negative n = 164 | Positive n = 336 | |||||||
| n | % | n | % | |||||
| Income < PLN 3000 | 140 | 85.4 | 250 | 74.4 | 0.006 | 2.01 (1.22–3.30) | 0.864 | 2.37 (1.26–4.47) |
| Body height < 174 cm | 136 | 82.9 | 215 | 64.0 | <0.001 | 2.73 (1.72–4.35) | 0.940 | 2.56 (1.51–4.33) |
| SMC < 6 pts | 66 | 45.8 | 105 | 36.6 | 0.076 | 1.47 (0.98–2.20) | 0.388 | 1.47 (0.95–2.28) |
| AMTS < 10 pts | 103 | 62.8 | 179 | 53.3 | 0.044 | 1.48 (1.01–2.17) | 0.405 | 1.50 (0.97–2.33) |
| GDS-15 ≥ 4 pts | 93 | 56.7 | 165 | 49.1 | 0.127 | 1.36 (0.93–1.98) | −0.153 | 0.86 (0.55–1.34) |
| LSND-6 < 24 pts | 159 | 97.0 | 313 | 93.2 | 0.098 | 2.34 (0.87–6.26) | 1.044 | 2.84 (0.91–8.89) |
| GLS < 16 pts | 156 | 95.1 | 298 | 88.7 | 0.021 | 2.49 (1.13–5.46) | 0.829 | 2.29 (0.89–5.93) |
| COVID-19 ≥ 23 pts | 58 | 35.4 | 78 | 23.2 | 0.005 | 1.81 (1.20–2.72) | 0.499 | 1.65 (1.02–2.66) |
| Asthma | 19 | 11.6 | 24 | 7.1 | 0.125 | 1.70 (0.90–3.21) | 0.544 | 1.72 (0.86–3.44) |
| Kidney failure | 10 | 6.1 | 10 | 3.0 | 0.142 | 2.12 (0.86–5.19) | 0.478 | 1.61 (0.59–4.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietraszek, A.; Sobieszczańska, M.; Makuch, S.; Dróżdż, M.; Mazur, G.; Agrawal, S. Identification of Barriers Limiting the Use of Preventive Vaccinations against Influenza among the Elderly Population: A Cross-Sectional Analysis. Vaccines 2022, 10, 651. https://doi.org/10.3390/vaccines10050651
Pietraszek A, Sobieszczańska M, Makuch S, Dróżdż M, Mazur G, Agrawal S. Identification of Barriers Limiting the Use of Preventive Vaccinations against Influenza among the Elderly Population: A Cross-Sectional Analysis. Vaccines. 2022; 10(5):651. https://doi.org/10.3390/vaccines10050651
Chicago/Turabian StylePietraszek, Alicja, Małgorzata Sobieszczańska, Sebastian Makuch, Mateusz Dróżdż, Grzegorz Mazur, and Siddarth Agrawal. 2022. "Identification of Barriers Limiting the Use of Preventive Vaccinations against Influenza among the Elderly Population: A Cross-Sectional Analysis" Vaccines 10, no. 5: 651. https://doi.org/10.3390/vaccines10050651