
Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study

 ,
,  ,
,  ,
,  ,
,  ,
,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
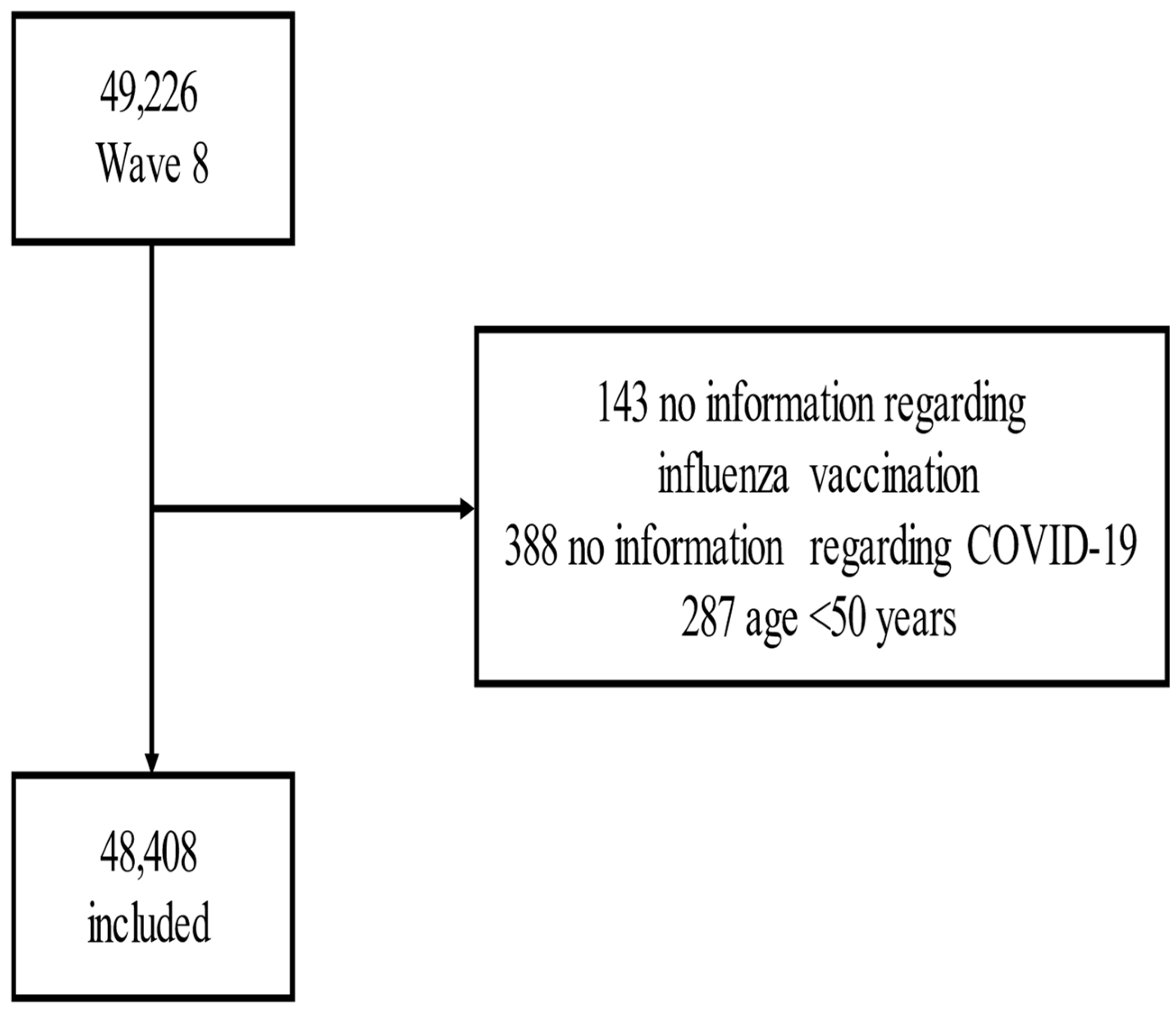
2.1. Sample and Data
2.2. Exposure: Influenza Vaccination
2.3. Outcomes: COVID-19
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Weekly Operational Update on COVID-19; Issue No. 97. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19---30-march-2022#.YkwrvaHCh8g.link (accessed on 30 March 2022).
- Lloyd-Sherlock, P.G.; Kalache, A.; McKee, M.; Derbyshire, J.; Geffen, L.; Casas, F.G.-O.; Gutierrez, L.M. WHO must prioritise the needs of older people in its response to the covid-19 pandemic. BMJ 2020, 368, m1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 18, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Külper-Schiek, W.; Reda, S.; Treskova-Schwarzbach, M.; Koch, J.; Vygen-Bonnet, S.; Wichmann, O. Effectiveness of COVID-19 vaccines against SARS-CoV-2 infection with the Delta (B. 1.617. 2) variant: Second interim results of a living systematic review and meta-analysis, 1 January to 25 August 2021. Eurosurveillance 2021, 26, 2100920. [Google Scholar]
- Ma, S.; Lai, X.; Chen, Z.; Tu, S.; Qin, K. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan, China. Int. J. Infect. Dis. 2020, 96, 683–687. [Google Scholar] [CrossRef]
- Noale, M.; Trevisan, C.; Maggi, S.; Antonelli Incalzi, R.; Pedone, C.; Di Bari, M.; Adorni, F.; Jesuthasan, N.; Sojic, A.; Galli, M. The association between influenza and pneumococcal vaccinations and SARS-Cov-2 infection: Data from the EPICOVID19 web-based survey. Vaccines 2020, 8, 471. [Google Scholar] [CrossRef]
- Giacomelli, A.; Galli, M.; Maggi, S.; Noale, M.; Trevisan, C.; Pagani, G.; Antonelli-Incalzi, R.; Molinaro, S.; Bastiani, L.; Cori, L. Influenza Vaccination Uptake in the General Italian Population during the 2020–2021 Flu Season: Data from the EPICOVID-19 Online Web-Based Survey. Vaccines 2022, 10, 293. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Poland, G. Influenza immunization and COVID-19. Vaccine 2020, 38, 6078. [Google Scholar] [CrossRef]
- Veronese, N.; Vassallo, G.; Armata, M.; Cilona, L.; Casalicchio, S.; Masnata, R.; Costantino, C.; Vitale, F.; Giammanco, G.M.; Maggi, S.; et al. Multidimensional Frailty and Vaccinations in Older People: A Cross-Sectional Study. Vaccines 2022, 10, 555. [Google Scholar] [CrossRef]
- Cowling, B.J.; Fang, V.J.; Nishiura, H.; Chan, K.-H.; Ng, S.; Ip, D.K.; Chiu, S.S.; Leung, G.M.; Peiris, J.M. Increased risk of noninfluenza respiratory virus infections associated with receipt of inactivated influenza vaccine. Clin. Infect. Dis. 2012, 54, 1778–1783. [Google Scholar] [CrossRef] [Green Version]
- Belingheri, M.; Paladino, M.; Latocca, R.; De Vito, G.; Riva, M. Association between seasonal flu vaccination and COVID-19 among healthcare workers. Occup. Med. 2020, 70, 665–671. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2020, 93, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Del Riccio, M.; Lorini, C.; Bonaccorsi, G.; Paget, J.; Caini, S. The association between influenza vaccination and the risk of SARS-CoV-2 infection, severe illness, and death: A systematic review of the literature. Int. J. Environ. Res. Public Health 2020, 17, 7870. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Wang, H.; Sun, C.; Li, N.; Guo, X.; Song, Q.; Liang, Q.; Liang, M.; Ding, X.; Sun, Y. The Association Between Previous Influenza Vaccination and Coronavirus Disease 2019 Infection Risk and Severity: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Liu, M.; Liu, J. The association between influenza vaccination and COVID-19 and its outcomes: A systematic review and meta-analysis of observational studies. Vaccines 2021, 9, 529. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Scherpenzeel, A.; Axt, K.; Bergmann, M.; Douhou, S.; Oepen, A.; Sand, G.; Schuller, K.; Stuck, S.; Wagner, M.; Börsch-Supan, A. Collecting survey data among the 50+ population during the COVID-19 outbreak: The Survey of Health, Ageing and Retirement in Europe (SHARE). Surv. Res. Methods 2020, 14, 217–221. [Google Scholar]
- Arnault, L.; Jusot, F.; Renaud, T. Economic vulnerability and unmet healthcare needs among the population aged 50+ years during the COVID-19 pandemic in Europe. Eur. J. Ageing 2021, 1–15. [Google Scholar] [CrossRef]
- Chłoń-Domińczak, A.; Holzer-Żelażewska, D. Economic stress of people 50+ in European countries in the Covid-19 pandemic–do country policies matter? Eur. J. Ageing 2021, 1–20. [Google Scholar] [CrossRef]
- Wallace, M.; Shelkey, M. Katz index of independence in activities of daily living (ADL). Urol. Nurs. 2007, 27, 93–94. [Google Scholar]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontol. 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Haukoos, J.S.; Lewis, R.J. The propensity score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef] [PubMed]
- Indicators, O. Health at a Glance 2019, OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Tramuto, F.; Mazzucco, W.; Maida, C.M.; Colomba, G.M.E.; Di Naro, D.; Coffaro, F.; Graziano, G.; Costantino, C.; Restivo, V.; Vitale, F. COVID-19 emergency in Sicily and intersection with the 2019-2020 influenza epidemic. J. Prev. Med. Hyg. 2021, 62, E10. [Google Scholar] [PubMed]
- Domnich, A.; Cambiaggi, M.; Vasco, A.; Maraniello, L.; Ansaldi, F.; Baldo, V.; Bonanni, P.; Calabrò, G.E.; Costantino, C.; de Waure, C. Attitudes and beliefs on influenza vaccination during the COVID-19 pandemic: Results from a representative Italian survey. Vaccines 2020, 8, 711. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Domínguez-Andrés, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.; van der Meer, J.W.; Mhlanga, M.M.; Mulder, W.J. Defining trained immunity and its role in health and disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Pinho, M.P.; Buckley, P.R.; Woodhouse, I.B.; Ogg, G.; Simmons, A.; Napolitani, G.; Koohy, H. Potential CD8+ T cell cross-reactivity against SARS-CoV-2 conferred by other coronavirus strains. Front. Immunol. 2020, 11, 2878. [Google Scholar] [CrossRef]
- Cardillo, F.; Bonfim, M.; da Silva Vasconcelos Sousa, P.; Mengel, J.; Ribeiro Castello-Branco, L.R.; Pinho, R.T. Bacillus Calmette–Guérin immunotherapy for cancer. Vaccines 2021, 9, 439. [Google Scholar] [CrossRef]
- Debisarun, P.A.; Gössling, K.L.; Bulut, O.; Kilic, G.; Zoodsma, M.; Liu, Z.; Oldenburg, M.; Rüchel, N.; Zhang, B.; Xu, C.-J. Induction of trained immunity by influenza vaccination-impact on COVID-19. PLoS Pathog. 2021, 17, e1009928. [Google Scholar] [CrossRef]
- Flerlage, T.; Boyd, D.F.; Meliopoulos, V.; Thomas, P.G.; Schultz-Cherry, S. Influenza virus and SARS-CoV-2: Pathogenesis and host responses in the respiratory tract. Nat. Rev. Microbiol. 2021, 19, 425–441. [Google Scholar] [CrossRef]
- Gabutti, G.; d’Anchera, E.; De Motoli, F.; Savio, M.; Stefanati, A. The epidemiological characteristics of the covid-19 pandemic in europe: Focus on Italy. Int. J. Environ. Res. Public Health 2021, 18, 2942. [Google Scholar] [CrossRef]
- Demurtas, J.; Celotto, S.; Beaudart, C.; Sanchez-Rodriguez, D.; Balci, C.; Soysal, P.; Solmi, M.; Celotto, D.; Righi, E.; Smith, L. The efficacy and safety of influenza vaccination in older people: An umbrella review of evidence from meta-analyses of both observational and randomized controlled studies. Ageing Res. Rev. 2020, 62, 101118. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Overall Sample | Influenza Vaccination (n = 18,655) | No Influenza Vaccination (n = 29,753) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Mean age (SD) | 67.0 (9.7) | 70.5 (9.7) | 64.9 (9.0) | <0.0001 |
| Females (%) | 54.1 | 54.2 | 54.1 | <0.0001 |
| Current smokers (%) | 11.0 | 8.0 | 12.9 | <0.0001 |
| Daily alcohol drinking (%) | 1.7 | 1.9 | 1.7 | <0.0001 |
| Mean years of education (SD) | 11.4 (4.3) | 11.3 (4.6) | 11.5 (4.2) | <0.0001 |
| Retired (%) | 34.7 | 63.0 | 44.1 | <0.0001 |
| Medical and functional information | ||||
| Mean BMI (SD) | 27.0 (4.7) | 26.9 (4.6) | 27.0 (4.8) | <0.0001 |
| Mean mobility limitation (SD) | 1.53 (2.28) | 1.76 (2.38) | 1.37 (2.20) | <0.0001 |
| Mean limitation in ADL (SD) | 0.21 (0.81) | 0.27 (0.92) | 0.18 (0.73) | <0.0001 |
| Mean limitations in IADL (SD) | 0.40 (1.32) | 0.51 (1.51) | 0.34 (1.18) | <0.0001 |
| Hip fracture (%) | 0.3 | 0.3 | 0.3 | <0.0001 |
| Diabetes (%) | 1.6 | 1.9 | 1.5 | <0.0001 |
| High blood pressure (%) | 3.9 | 4.6 | 3.6 | <0.0001 |
| Heart problems (%) | 2.1 | 2.7 | 1.8 | <0.0001 |
| Lung disease (%) | 1.1 | 1.5 | 0.8 | <0.0001 |
| Cancer (%) | 1.3 | 2.1 | 0.8 | <0.0001 |
| Regularly takes prescription drugs (%) | 69.5 | 82.7 | 63.4 | <0.0001 |
| Vaccination history | ||||
| Vaccination against COVID-19 (%) | 82.5 | 95.5 | 74.4 | <0.0001 |
| Vaccination against pneumococcus (%) | 11.5 | 23.8 | 3.8 | <0.0001 |
| Influenza Vaccination | Percentage of Events | Fully-Adjusted 1 OR, 95% CI | Propensity Score 2 Adjusted OR, 95% CI |
|---|---|---|---|
| Positivity for COVID-19 | |||
| No | 4.8 | 1 [reference] | 1 [reference] |
| Yes | 6.2 | 0.95 (0.94–0.96) p ≤ 0.0001 | 0.86 (0.85–0.87) p ≤ 0.0001 |
| Symptomatic COVID-19 | |||
| No | 8.1 | 1 [reference] | 1 [reference] |
| Yes | 5.8 | 0.87 (0.86–0.88) p ≤ 0.0001 | 0.96 (0.96–0.97) p ≤ 0.0001 |
| Hospitalization COVID-19 | |||
| No | 1.1 | 1 [reference] | 1 [reference] |
| Yes | 0.9 | 0.95 (0.94–0.96) p ≤ 0.0001 | 0.78 (0.77–0.79) p ≤ 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veronese, N.; Smith, L.; Di Gennaro, F.; Bruyère, O.; Yang, L.; Demurtas, J.; Maggi, S.; Sabico, S.; Al-Daghri, N.M.; Barbagallo, M.; et al. Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study. Vaccines 2022, 10, 899. https://doi.org/10.3390/vaccines10060899
Veronese N, Smith L, Di Gennaro F, Bruyère O, Yang L, Demurtas J, Maggi S, Sabico S, Al-Daghri NM, Barbagallo M, et al. Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study. Vaccines. 2022; 10(6):899. https://doi.org/10.3390/vaccines10060899
Chicago/Turabian StyleVeronese, Nicola, Lee Smith, Francesco Di Gennaro, Olivier Bruyère, Lin Yang, Jacopo Demurtas, Stefania Maggi, Shaun Sabico, Nasser M. Al-Daghri, Mario Barbagallo, and et al. 2022. "Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study" Vaccines 10, no. 6: 899. https://doi.org/10.3390/vaccines10060899
APA StyleVeronese, N., Smith, L., Di Gennaro, F., Bruyère, O., Yang, L., Demurtas, J., Maggi, S., Sabico, S., Al-Daghri, N. M., Barbagallo, M., Dominguez, L. J., & Koyanagi, A. (2022). Influenza Vaccination and COVID-19 Outcomes in People Older than 50 Years: Data from the Observational Longitudinal SHARE Study. Vaccines, 10(6), 899. https://doi.org/10.3390/vaccines10060899