
Quantification of Aortic Valve Calcification in Contrast-Enhanced Computed Tomography

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Computed Tomography Acquisition and Reconstruction
2.3. Agatston Score
2.4. Threshold Measurement in Contrast-Enhanced Computed Tomography
2.5. Predictive Quantification of Aortic Valve Calcification in Contrast-Enhanced Computed Tomography
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics
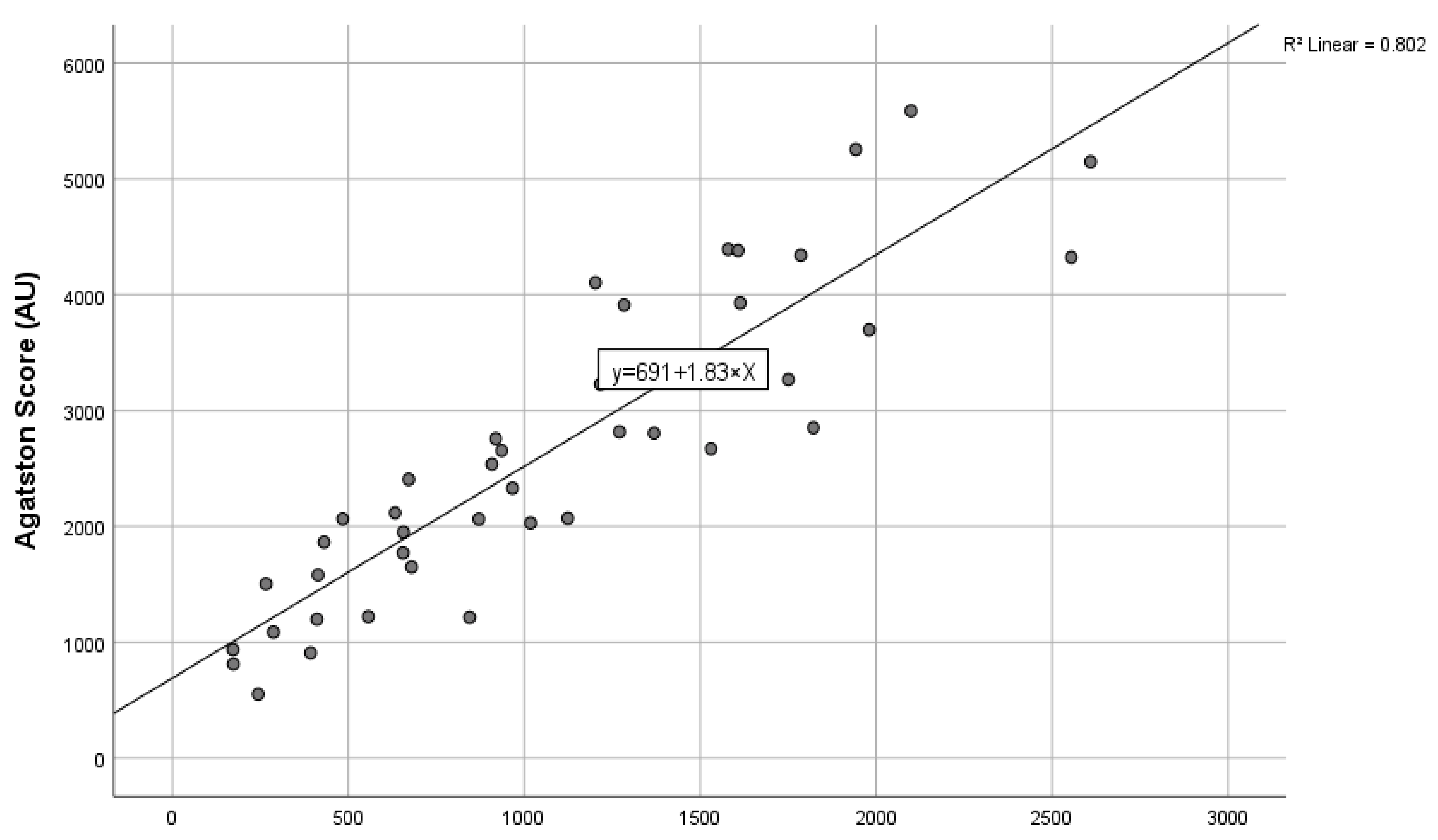
3.2. Derivation of the Conversion Formula to Calculate the Agatston Score in Contrast-Enhanced Computed Tomography Scans
3.3. Confirmation of Agreement in the Validation Cohort
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Data
4.3. Importance of Agatston Score as a Prognostic Tool
4.4. Pixel Noise Detection
4.5. Fixed and Dynamic Thresholds for the Quantification of Aortic Valve Calcification
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pawade, T.; Clavel, M.A.; Tribouilloy, C.; Dreyfus, J.; Mathieu, T.; Tastet, L.; Renard, C.; Gun, M.; Jenkins, W.S.A.; Macron, L.; et al. Computed Tomography Aortic Valve Calcium Scoring in Patients with Aortic Stenosis. Circ. Cardiovasc. Imaging 2018, 11, e007146. [Google Scholar] [CrossRef] [PubMed]
- Pawade, T.; Sheth, T.; Guzzetti, E.; Dweck, M.R.; Clavel, M.A. Why and How to Measure Aortic Valve Calcification in Patients With Aortic Stenosis. JACC Cardiovasc. Imaging 2019, 12, 1835–1848. [Google Scholar] [CrossRef] [PubMed]
- Rosenhek, R.; Binder, T.; Porenta, G.; Lang, I.; Christ, G.; Schemper, M.; Maurer, G.; Baumgartner, H. Predictors of outcome in severe, asymptomatic aortic stenosis. N. Engl. J. Med. 2000, 343, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.S.; Budoff, M.J.; Katz, R.; Takasu, J.; Shavelle, D.M.; Carr, J.J.; Heckbert, S.R.; Otto, C.M.; Probstfield, J.L.; Kronmal, R.A.; et al. Aortic valve calcium independently predicts coronary and cardiovascular events in a primary prevention population. JACC Cardiovasc. Imaging 2012, 5, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Fujita, B.; Kutting, M.; Seiffert, M.; Scholtz, S.; Egron, S.; Prashovikj, E.; Borgermann, J.; Schafer, T.; Scholtz, W.; Preuss, R.; et al. Calcium distribution patterns of the aortic valve as a risk factor for the need of permanent pacemaker implantation after transcatheter aortic valve implantation. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Buellesfeld, L.; Stortecky, S.; Heg, D.; Gloekler, S.; Meier, B.; Wenaweser, P.; Windecker, S. Extent and distribution of calcification of both the aortic annulus and the left ventricular outflow tract predict aortic regurgitation after transcatheter aortic valve replacement. EuroIntervention 2014, 10, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Possner, M.; Vontobel, J.; Nguyen-Kim, T.D.; Zindel, C.; Holy, E.W.; Stampfli, S.F.; Zuber, M.; Kaufmann, P.A.; Nietlispach, F.; Maisano, F.; et al. Prognostic value of aortic regurgitation after TAVI in patients with chronic kidney disease. Int. J. Cardiol. 2016, 221, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Minners, J.; Allgeier, M.; Gohlke-Baerwolf, C.; Kienzle, R.P.; Neumann, F.J.; Jander, N. Inconsistencies of echocardiographic criteria for the grading of aortic valve stenosis. Eur. Heart J. 2008, 29, 1043–1048. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Messika-Zeitoun, D.; Aubry, M.C.; Detaint, D.; Bielak, L.F.; Peyser, P.A.; Sheedy, P.F.; Turner, S.T.; Breen, J.F.; Scott, C.; Tajik, A.J.; et al. Evaluation and clinical implications of aortic valve calcification measured by electron-beam computed tomography. Circulation 2004, 110, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Koos, R.; Mahnken, A.H.; Kuhl, H.P.; Muhlenbruch, G.; Mevissen, V.; Stork, L.; Dronskowski, R.; Langebartels, G.; Autschbach, R.; Ortlepp, J.R. Quantification of aortic valve calcification using multislice spiral computed tomography: Comparison with atomic absorption spectroscopy. Investig. Radiol. 2006, 41, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Linde, L.; Carter-Storch, R.; Christensen, N.L.; Dahl, J.; Ovrehus, K.A.; Diederichsen, A.; Jensen, P.S.; Rasmussen, L.M.; Moller, J.E. Strong Correlation between Aortic Valve Calcification Score by Cardiac Computed Tomography and Total Valve Calcium in Patients with Severe Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2018, 71, 1985. [Google Scholar] [CrossRef]
- Eberhard, M.; Mastalerz, M.; Frauenfelder, T.; Tanner, F.C.; Maisano, F.; Nietlispach, F.; Seifert, B.; Alkadhi, H.; Nguyen-Kim, T.D.L. Quantification of aortic valve calcification on contrast-enhanced CT of patients prior to transcatheter aortic valve implantation. EuroIntervention 2017, 13, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.M.; Boczar, K.E.; Kansal, V.; Chan, K.; Dwivedi, G.; Chow, B.J. Quantifying Aortic Valve Calcification using Coronary Computed Tomography Angiography. J. Cardiovasc. Comput. Tomogr. 2017, 11, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Ruile, P.; Pache, G.; Minners, J.; Hein, M.; Neumann, F.J.; Breitbart, P. Fusion imaging of pre- and post-procedural computed tomography angiography in transcatheter aortic valve implantation patients: Evaluation of prosthesis position and its influence on new conduction disturbances. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Cueff, C.; Serfaty, J.M.; Cimadevilla, C.; Laissy, J.P.; Himbert, D.; Tubach, F.; Duval, X.; Iung, B.; Enriquez-Sarano, M.; Vahanian, A.; et al. Measurement of aortic valve calcification using multislice computed tomography: Correlation with haemodynamic severity of aortic stenosis and clinical implication for patients with low ejection fraction. Heart 2011, 97, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Abdelkhalek, M.; Daeian, M.; Chavarria, J.; Sellers, S.; Gulsin, G.; Leipsic, J.; Sheth, T.; Keshavarz-Motamed, Z. Patterns and Structure of Calcification in Aortic Stenosis: An Approach on Contrast-Enhanced CT Images. JACC Cardiovasc. Imaging 2023, 16, 1224–1226. [Google Scholar] [CrossRef] [PubMed]
- Abdelkhalek, M.; Daeian, M.; Keshavarz-Motamed, Z. Regional assessment of aortic valve calcification using topographic maps in contrast-enhanced CT: In-vivo sex and severity-based differences in calcific presentation. Quant. Imaging Med. Surg. 2024, 14, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, H.; Hoelschermann, F.; Seifert, M.; Tambor, G.; Okamoto, M.; Moeller, V.; Neuss, M.; Butter, C. Predictors of permanent pacemaker implantation after transcatheter aortic valve implantation for aortic stenosis using Medtronic new generation self-expanding CoreValve Evolut R. Heart Vessel. 2019, 34, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Katchi, F.; Bhatt, D.; Markowitz, S.M.; Szymonifka, J.; Cheng, E.P.; Minutello, R.M.; Bergman, G.W.; Wong, S.C.; Salemi, A.; Truong, Q.A. Impact of Aortomitral Continuity Calcification on Need for Permanent Pacemaker After Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Imaging 2019, 12, e009570. [Google Scholar] [CrossRef] [PubMed]
- Maeno, Y.; Abramowitz, Y.; Kawamori, H.; Kazuno, Y.; Kubo, S.; Takahashi, N.; Mangat, G.; Okuyama, K.; Kashif, M.; Chakravarty, T.; et al. A Highly Predictive Risk Model for Pacemaker Implantation After TAVR. JACC Cardiovasc. Imaging 2017, 10, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Ali, O.F.; Schultz, C.; Jabbour, A.; Rubens, M.; Mittal, T.; Mohiaddin, R.; Davies, S.; Di Mario, C.; Van der Boon, R.; Ahmad, A.S.; et al. Predictors of paravalvular aortic regurgitation following self-expanding Medtronic CoreValve implantation: The role of annulus size, degree of calcification, and balloon size during pre-implantation valvuloplasty and implant depth. Int. J. Cardiol. 2015, 179, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Greason, K.L.; Williamson, E.E.; Suri, R.M.; Mathew, V. High Agatston aortic valve calcium score predicts transcatheter paravalvular aortic regurgitation. J. Thorac. Cardiovasc. Surg. 2014, 147, 1991. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.Y.; Kao, H.L.; Chen, Y.C.; Lin, L.C.; Liu, Y.J.; Yeh, C.F.; Huang, C.C.; Chen, Y.H.; Chen, Y.S.; Lin, M.S. Temporal Change in Paravalvular Leakage after Transcatheter Aortic Valve Replacement with a Self-Expanding Valve: Impact of Aortic Valve Calcification. Acta Cardiol. Sin. 2020, 36, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.K.; van Rosendael, P.J.; van der Kley, F.; de Weger, A.; Kamperidis, V.; Regeer, M.V.; Marsan, N.A.; Bax, J.J.; Delgado, V. Impact of Different Iterations of Devices and Degree of Aortic Valve Calcium on Paravalvular Regurgitation after Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 118, 567–571. [Google Scholar] [CrossRef]
- Higashigaito, K.; Schmid, T.; Puippe, G.; Morsbach, F.; Lachat, M.; Seifert, B.; Pfammatter, T.; Alkadhi, H.; Husarik, D.B. CT Angiography of the Aorta: Prospective Evaluation of Individualized Low-Volume Contrast Media Protocols. Radiology 2016, 280, 960–968. [Google Scholar] [CrossRef]
- Winklehner, A.; Goetti, R.; Baumueller, S.; Karlo, C.; Schmidt, B.; Raupach, R.; Flohr, T.; Frauenfelder, T.; Alkadhi, H. Automated attenuation-based tube potential selection for thoracoabdominal computed tomography angiography: Improved dose effectiveness. Invest Radiol. 2011, 46, 767–773. [Google Scholar] [CrossRef]
- Flores-Umanzor, E.; Keshvara, R.; Reza, S.; Asghar, A.; Rashidul Anwar, M.; Cepas-Guillen, P.L.; Osten, M.; Halankar, J.; Abrahamyan, L.; Horlick, E. A systematic review of contrast-enhanced computed tomography calcium scoring methodologies and impact of aortic valve calcium burden on TAVI clinical outcomes. J. Cardiovasc. Comput. Tomogr. 2023, 17, 373–383. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Derivation Cohort (n = 45) | Validation Cohort (n = 20) | p |
|---|---|---|---|
| Age (years) | 81.0 ± 6.2 | 78.5 ± 5.0 | 0.472 |
| Female (n (%)) | 22 (48.9%) | 6 (30%) | 0.156 |
| Weight (kg) | 75.2 ± 13.7 | 84.3 ± 16.6 | 0.023 |
| Height (cm) | 166.8 ± 7.9 | 166.6 ± 15.1 | 0.144 |
| BMI (kg/m2) | 27.0 ± 4.5 | 29.1 ± 4.9 | 0.094 |
| Hypertension (n (%)) | 40 (89.0%) | 15 (75.0%) | 0.152 |
| Diabetes (n (%)) | 15 (33.3%) | 9 (45.0%) | 0.368 |
| Dyslipidaemia (n (%)) | 27 (60.0%) | 15 (75.0%) | 0.243 |
| Smoking (n (%)) | 6 (13.3%) | 5 (25.0%) | 0.247 |
| Coronary artery disease (n (%)) | 30 (66.7%) | 12 (60.0%) | 0.604 |
| Renal disease (n (%)) | 7 (15.6%) | 5 (25.0%) | 0.365 |
| Peripheral artery disease (n (%)) | 9 (20.0%) | 5 (25.0%) | 0.651 |
| Non-contrast CT | |||
| Tube voltage (kV) | 120 | 120 | |
| Tube current (mAs) | 142.9 ± 29.4 | 152.8 ± 34.5 | 0.249 |
| Contrast-enhanced CT | |||
| Tube voltage (kV) | 100 ± 0 | 100 ± 0 | |
| Tube current (mAs) | 480.7 ± 113.3 | 512.3 ± 111.5 | 0.320 |
| AVC segmentation threshold (HU) | 471 ± 117 | 461 ± 88 | 0.537 |
| Interclass correlation coefficient of the Derivation cohort | 0.942 CI (0.894–0.968), p < 0.001 |
| Interclass correlation coefficient of the Validation cohort | 0.915 CI (0.786–0.966), p < 0.001 |
| Goodness of fit (R2) | 0.802, p < 0.001 |
| Bland–Altman linear proportional bias P | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laohachewin, D.; Ruile, P.; Breitbart, P.; Minners, J.; Jander, N.; Soschynski, M.; Schlett, C.L.; Neumann, F.-J.; Westermann, D.; Hein, M. Quantification of Aortic Valve Calcification in Contrast-Enhanced Computed Tomography. J. Clin. Med. 2024, 13, 2386. https://doi.org/10.3390/jcm13082386
Laohachewin D, Ruile P, Breitbart P, Minners J, Jander N, Soschynski M, Schlett CL, Neumann F-J, Westermann D, Hein M. Quantification of Aortic Valve Calcification in Contrast-Enhanced Computed Tomography. Journal of Clinical Medicine. 2024; 13(8):2386. https://doi.org/10.3390/jcm13082386
Chicago/Turabian StyleLaohachewin, Danai, Philipp Ruile, Philipp Breitbart, Jan Minners, Nikolaus Jander, Martin Soschynski, Christopher L. Schlett, Franz-Josef Neumann, Dirk Westermann, and Manuel Hein. 2024. "Quantification of Aortic Valve Calcification in Contrast-Enhanced Computed Tomography" Journal of Clinical Medicine 13, no. 8: 2386. https://doi.org/10.3390/jcm13082386