A Nomogram to Predict the Outcome of Fine Needle Aspiration Cytology in Head and Neck Masses

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Fine Needle Aspiration Cytology
2.3. Statistical Analysis
3. Results
3.1. Patients
3.2. FNAC Results
3.3. Univariate Analysis
3.4. Multivariate Analysis
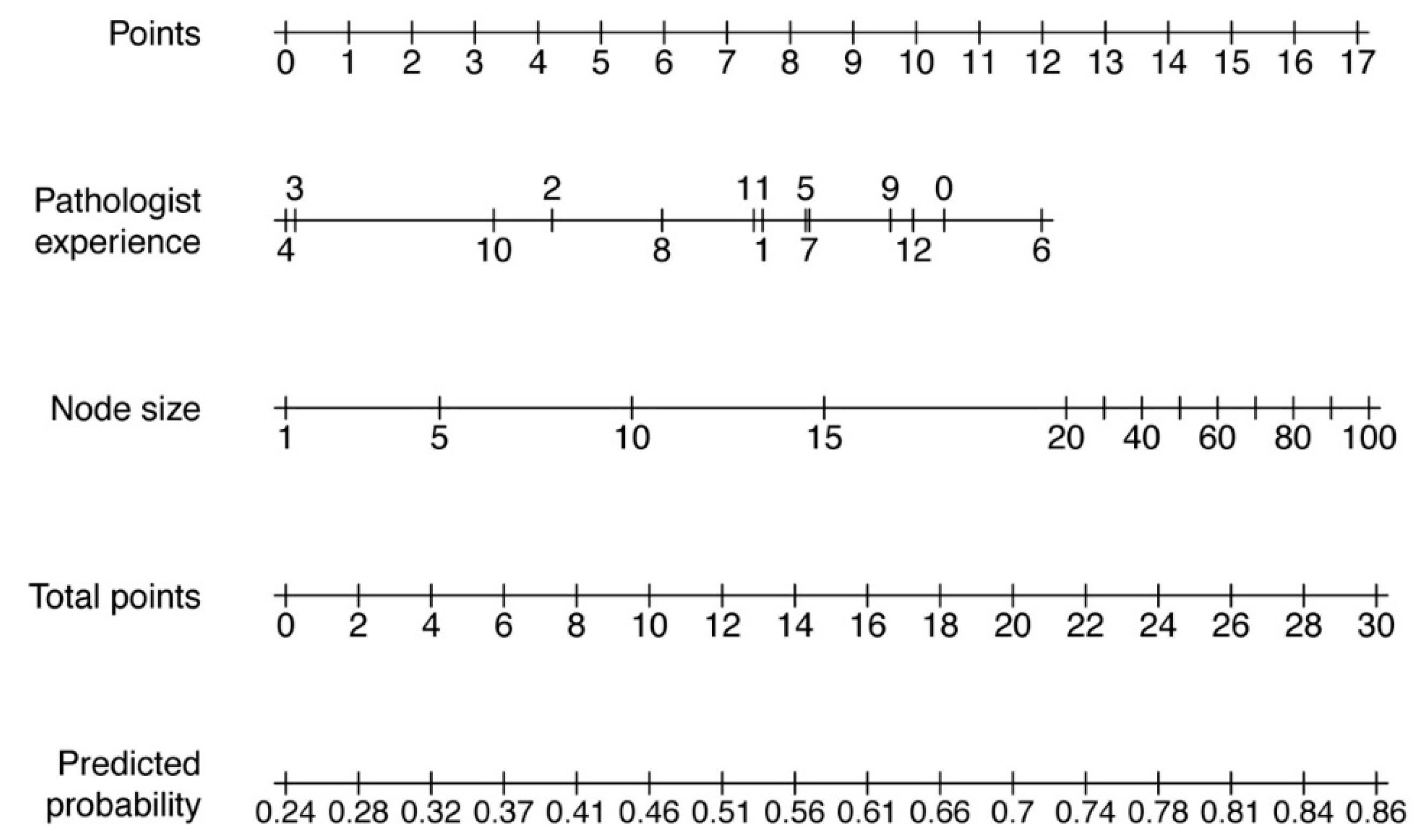
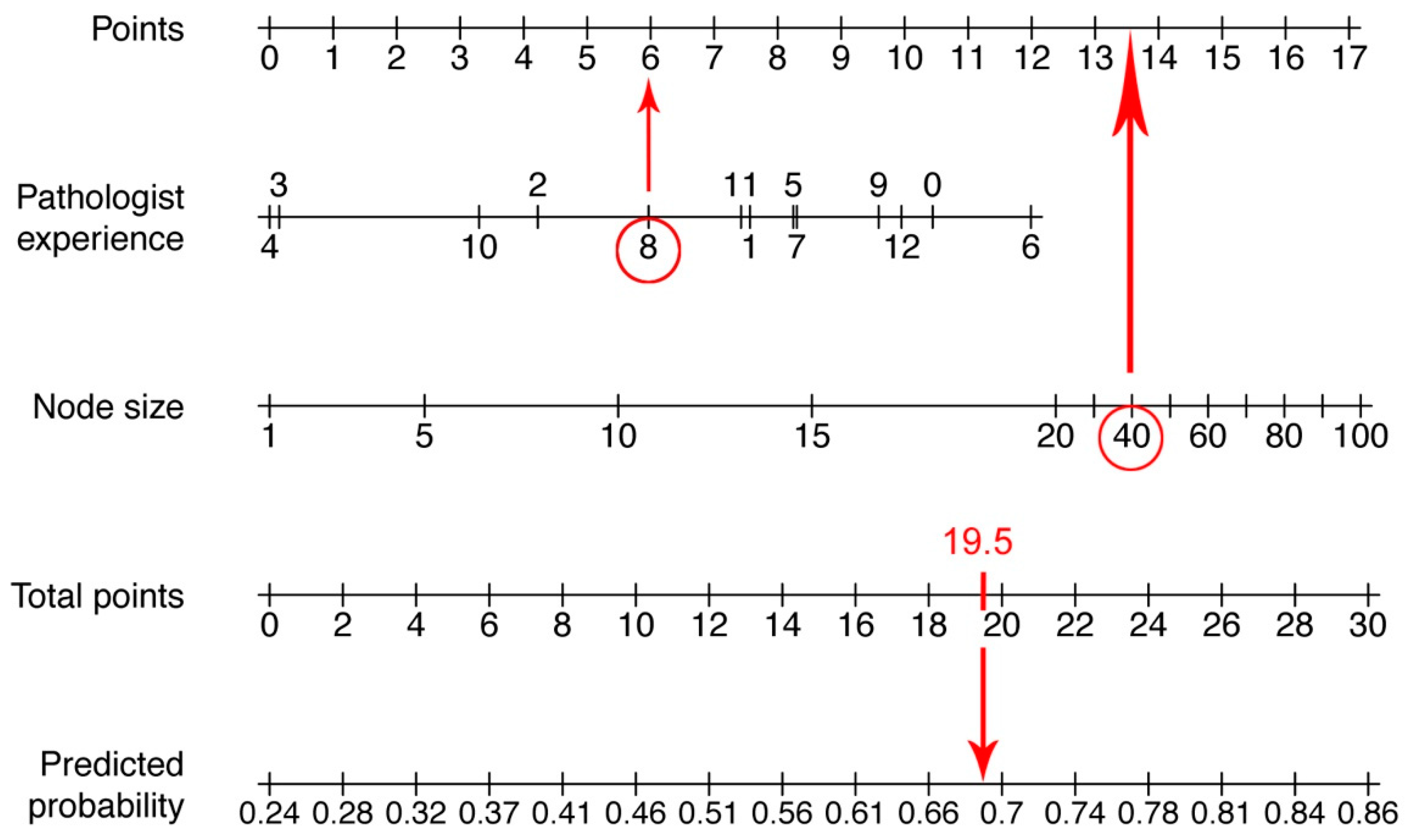
3.5. Nomogram
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Tandon, S.; Shahab, R.; Benton, J.I.; Ghosh, S.K.; Sheard, J.; Jones, T.M. Fine-needle aspiration cytology in a regional head and neck cancer center: Comparison with a systematic review and meta-analysis. Head Neck 2008, 30, 1246–1252. [Google Scholar] [CrossRef] [PubMed]
- Rammeh, S.; Romdhane, E.; Sassi, A.; Belhajkacem, L.; Blel, A.; Ksentini, M.; Lahiani, R.; Farah, F.; Salah, M.B.; Ferjaoui, M. Accuracy of fine-needle aspiration cytology of head and neck masses. Diagn. Cytopathol. 2019, 47, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, A.; Burnside, G.; Nixon, P. A systematic review of ultrasound-guided FNA of lesions in the head and neck—Focusing on operator, sample inadequacy and presence of on-spot cytology service. Br. J. Radiol. 2014, 87, 20130571. [Google Scholar] [CrossRef] [PubMed]
- Pynnonen, M.A.; Gillespie, M.B.; Roman, B.; Rosenfeld, R.M.; Tunkel, D.E.; Bontempo, L.; Brook, I.; Chick, D.A.; Colandrea, M.; Finestone, S.A.; et al. Clinical Practice Guideline: Evaluation of the Neck Mass in Adults. Otolaryngol. Head Neck Surg. 2017, 157, S1–S30. [Google Scholar] [CrossRef]
- Kotowski, U.; Brkic, F.F.; Koperek, O.; Nemec, S.F.; Perisanidis, C.; Altorjai, G.; Grasl, M.C.; Erovic, B.M. Accuracy of fine-needle aspiration cytology in suspicious neck nodes after radiotherapy: Retrospective analysis of 100 patients. Clin. Otolaryngol. 2019, 44, 384–388. [Google Scholar] [CrossRef]
- Kocjan, G.; Chandra, A.; Cross, P.; Denton, K.; Giles, T.; Herbert, A.; Smith, P.; Remedios, D.; Wilson, P. BSCC Code of Practice--fine needle aspiration cytology. Cytopathology 2009, 20, 283–296. [Google Scholar] [CrossRef]
- Isaac, A.; Jeffery, C.C.; Seikaly, H.; Al-Marzouki, H.; Harris, J.R.; O’Connell, D.A. Predictors of non-diagnostic cytology in surgeon-performed ultrasound guided fine needle aspiration of thyroid nodules. J. Otolaryngol. Head Neck Surg. 2014, 43, 48. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gönen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Houlton, J.J.; Sun, G.H.; Fernandez, N.; Zhai, Q.J.; Lucas, F.; Steward, D.L. Thyroid Fine-Needle Aspiration: Does Case Volume Affect Diagnostic Yield and Interpretation? Arch. Otolaryngol. Head Neck Surg. 2011, 137, 1136–1139. [Google Scholar] [CrossRef]
- Grasl, S.; Kadletz, L.; Janik, S.; Riedl, A.; Erlacher, B.; Formanek, M.; Grasl, M.C.; Erovic, B.M. Fine-needle aspiration cytology and intraoperative frozen section in parotid gland tumour surgery: A retrospective multicenter analysis of 417 cases. Clin. Otolaryngol. 2019, 44, 461–465. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, E.J.; Kim, S.H.; Kim, T.H.; Lee, S.H.; Kim, D.H.; Rho, M.H. Ultrasound-guided fine-needle aspiration biopsy of thyroid nodules: Comparison in efficacy according to nodule size. Thyroid 2009, 19, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.W.; Kim, D.W.; Jung, H.S.; Choo, H.J.; Park, Y.M.; Jung, S.J.; Baek, H.J. Factors Influencing the Outcome of Ultrasound-Guided Fine-Needle Aspiration for Salivary Gland Lesion Diagnosis. J. Ultrasound Med. 2016, 35, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Jandu, M.; Webster, K. The role of operator experience in fine needle aspiration cytology of head and neck masses. Int. J. Oral Maxillofac. Surg. 1999, 28, 441–444. [Google Scholar] [CrossRef]
- Nasuti, J.F.; Gupta, P.K.; Baloch, Z.W. Diagnostic value and cost-effectiveness of on-site evaluation of fine-needle aspiration specimens: Review of 5,688 cases. Diagn. Cytopathol. 2002, 27, 1–4. [Google Scholar] [CrossRef]
- Jahshan, F.; Doweck, I.; Ronen, O. Learning Curve of Fine-Needle Aspiration Cytology of Head and Neck Masses. Isr. Med. Assoc. J. 2016, 18, 350–353. [Google Scholar]
- Agcaoglu, O.; Aksakal, N.; Ozcinar, B.; Sarici, I.S.; Ercan, G.; Kucukyilmaz, M.; Yanar, F.; Ozemir, I.A.; Kilic, B.; Caglayan, K.; et al. Factors that affect the false-negative outcomes of fine-needle aspiration biopsy in thyroid nodules. Int. J. Endocrinol. 2013, 2013, 126084. [Google Scholar] [CrossRef]
- Schmidt, R.L.; Kordy, M.A.; Howard, K.; Layfield, L.J.; Hall, B.J.; Adler, D.G. Risk-benefit analysis of sampling methods for fine-needle aspiration cytology: A mathematical modeling approach. Am. J. Clin. Pathol. 2013, 139, 336–344. [Google Scholar] [CrossRef]
- Yom, S.S.; Garden, A.S.; Staerkel, G.A.; Ginsberg, L.E.; Morrison, W.H.; Sturgis, E.M.; Rosenthal, D.I.; Myers, J.N.; Edeiken-Monroe, B.S. Sonographic examination of the neck after definitive radiotherapy for node-positive oropharyngeal cancer. Am. J. Neuroradiol. 2011, 32, 1532–1538. [Google Scholar] [CrossRef]
- Addams-Williams, J.; Watkins, D.; Owen, S.; Williams, N.; Fielder, C. Non-thyroid neck lumps: Appraisal of the role of fine needle aspiration cytology. Eur. Arch. Otorhinolaryngol. 2009, 266, 411–415. [Google Scholar] [CrossRef]
- Burke, C.; Thomas, R.; Inglis, C.; Baldwin, A.; Ramesar, K.; Grace, R.; Howlett, D.C. Ultrasound-guided core biopsy in the diagnosis of lymphoma of the head and neck. A 9 year experience. Br. J. Radiol. 2011, 84, 727–732. [Google Scholar] [CrossRef]
- Tham, T.; Machado, R.; Herman, S.W.; Kraus, D.; Costantino, P.; Roche, A. Personalized prognostication In head and neck cancer: A systematic review of nomograms according to the AJCC precision medicine core (PMC) criteria. Head Neck 2019, 41, 2811–2822. [Google Scholar] [CrossRef] [PubMed]
- Nixon, I.J.; Ganly, I.; Hann, L.E.; Yu, C.; Palmer, F.L.; Whitcher, M.M.; Shah, J.P.; Shaha, A.; Kattan, M.W.; Patel, S.G. Nomogram for selecting thyroid nodules for ultrasound-guided fine-needle aspiration biopsy based on a quantification of risk of malignancy. Head Neck 2013, 35, 1022–1025. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Zhu, L.; Li, W.; Tang, Q.; Pan, F.; Wu, W.; Liu, J.; Yao, C.; Wang, S. External validation of a nomogram that predicts the pathological diagnosis of thyroid nodules in a Chinese population. PLoS ONE 2013, 8, e65162. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Benign Lesion | Malignant Lesion | No Histology Available | Total Number | |
|---|---|---|---|---|
| Non-diagnostic FNAC | 124 (10.2%) | 97 (7.9%) | 117 (9.6%) | 338 (27.7%) |
| Inconclusive FNAC | 23 (1.8%) | 51 (4.2%) | 16 (1.3%) | 90 (7.3%) |
| Benign FNAC | 273 (22.4%) | 93 (7.6%) | 153 (12.5%) | 519 (42.5%) |
| Malignant FNAC | 8 (0.7%) | 204 (16.7%) | 62 (5.1%) | 274 (22.5%) |
| Total Number | 428 (35.1%) | 445 (36.4%) | 348 (28.5%) | 1221 (100%) |
| Benign Lesion | Malignant Lesion | |
|---|---|---|
| Benign FNAC | True Negative 273 (97%) | False Negative 93 (31%) |
| Malignant FNAC | False Positive 8 (3%) | True Positive 204 (69%) |
| Variables | p-Value |
|---|---|
| Patient‘s age | 0.1848 |
| Node size (metric scale) | 0.0010 |
| Node > 20 mm (yes/no) | 0.0004 |
| Previous radiotherapy | 0.3326 |
| Localization of node | 0.2250 |
| Pathologist experience in years | 0.00003 |
| Pathologist experience in levels | 0.2715 |
| Head and neck surgeon experience in years | 0.2341 |
| Head and neck surgeon experience in levels | 0.1110 |
| Variables | p-Value |
|---|---|
| Pathologist experience after 1 year | 0.4498 |
| Pathologist experience after 2 years | 0.1025 |
| Pathologist experience after 3 years | 0.0079 |
| Pathologist experience after 4 years | 0.0080 |
| Pathologist experience after 5 years | 0.5951 |
| Pathologist experience after 6 years | 0.7170 |
| Pathologist experience after 7 years | 0.6074 |
| Pathologist experience after 8 years | 0.3104 |
| Pathologist experience after 9 years | 0.8464 |
| Pathologist experience after 10 years | 0.1008 |
| Pathologist experience after 11 years | 0.6699 |
| Pathologist experience after 12 years | 0.9483 |
| Node size (metric scale) | 0.0109 |
| Node > 20 mm (yes/no) | 0.0311 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotowski, U.; Brkic, F.F.; Koperek, O.; Pablik, E.; Grasl, S.; Grasl, M.C.; Erovic, B.M. A Nomogram to Predict the Outcome of Fine Needle Aspiration Cytology in Head and Neck Masses. J. Clin. Med. 2019, 8, 2050. https://doi.org/10.3390/jcm8122050
Kotowski U, Brkic FF, Koperek O, Pablik E, Grasl S, Grasl MC, Erovic BM. A Nomogram to Predict the Outcome of Fine Needle Aspiration Cytology in Head and Neck Masses. Journal of Clinical Medicine. 2019; 8(12):2050. https://doi.org/10.3390/jcm8122050
Chicago/Turabian StyleKotowski, Ulana, Faris F. Brkic, Oskar Koperek, Eleonore Pablik, Stefan Grasl, Matthaeus Ch. Grasl, and Boban M. Erovic. 2019. "A Nomogram to Predict the Outcome of Fine Needle Aspiration Cytology in Head and Neck Masses" Journal of Clinical Medicine 8, no. 12: 2050. https://doi.org/10.3390/jcm8122050