
Reducing Environmental Impacts at a Midwestern Academic Medical Center: Making Carbon Emissions Reduction a Reality


Abstract
:1. Introduction
Review of Literature
2. Materials and Methods
2.1. Setting
2.2. Interventions
2.2.1. GHG Emission Assessment/Measurement
2.2.2. Data Included
- Electricity, steam, and natural gas data were collected directly from the utility providers in the form of usage statements.
- Anesthetic gas data was collected from the MAMC’s Pharmacy Compliance Monitoring and Audit Supervisor.
- Refrigerant replacement data was collected from dated invoices showing the type of refrigerant and the volume replaced.
- An electronic report of fleet vehicle fuel usage data was shared by MAMC’s Supply Chain Logistics Specialist.
2.2.3. Education
2.2.4. Energy Audit and Goal Development
2.2.5. Measurement of Employee Knowledge
2.3. Ethical Considerations
3. Results
3.1. GHG Emissions Assessment/Measurement
3.2. Education
3.3. Data Analysis
3.4. Pre-Intervention
3.5. Post-Intervention
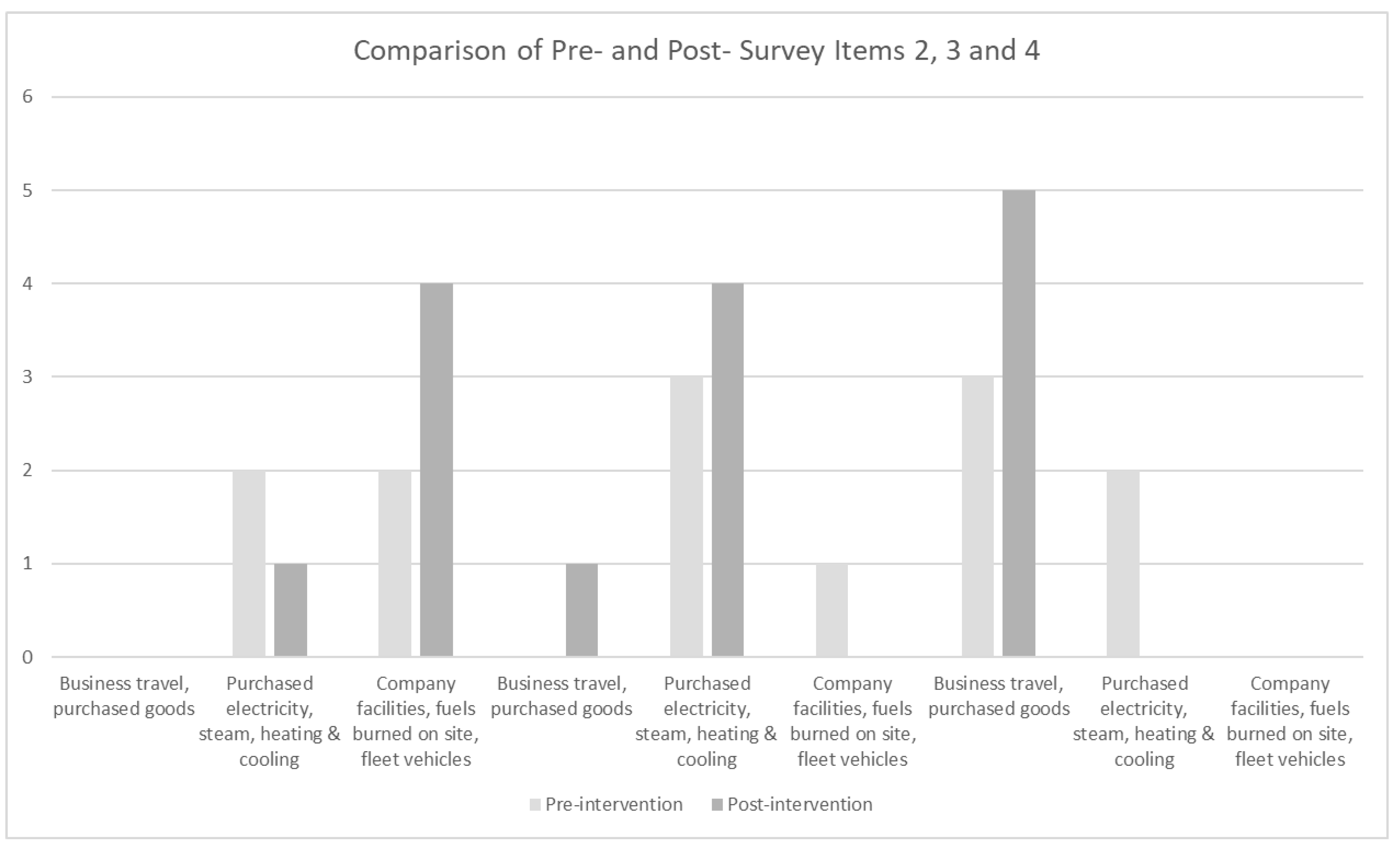
3.6. Pre-Post-Intervention Comparison
3.7. Limitations
- There are some notable limitations to this QI project. First, the sample size is not large enough to be a representative sample. This project was designed as a QI pilot for the MAMC site within a large health system, and so the accountable team of staff at the specific site was only five employees. Second, this QI project represents the first phase of a large-scale project aimed at reducing GHG emissions, so the efficacy of the GHG inventory cannot be totally measured at this stage of the project.
- The virtual training platform used for the education intervention introduced some limitations, such as the opportunity for attendees to practice data entry into the GHG inventory in real time. To remove some of these limitations, the project should be expanded across sites, involve more participants, and extend the length of the project to measure reductions in GHG emissions over time.
4. Discussion
- 3.
- Executive leaders and the accountable FD staff were presented with the results of this statistical analysis and predictive modeling. The organization made a commitment through executive sponsorship of this LSS Black Belt project to implement some improvement measures. The project owner is in the process of developing an implementation plan and leading continued discussions to determine the improvement methods that will be approved for implementation by the project’s executive sponsor. The next steps are to implement improvements, continue to collect and analyze data, measure the success of the improvement methods, and develop and implement a control plan.
- 4.
- Unexpected but propitious outcomes were the high level of engagement and interest of employees across the organization seeking to learn more about this project and the status of climate readiness at the MAMC. A movement has developed, and employees from across disciplines are seeking knowledge about the organization’s limited portfolio of environmental sustainability initiatives. Employees and community members are expressing curiosity about how climate action and environmental stewardship can be integrated into the health system’s core mission, vision, and values in a tangible way.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Intergovernmental Panel on Climate Change. Climate Change 2022: Mitigation of Climate Change. 2022. Available online: https://www.ipcc.ch/report/ar6/wg3/ (accessed on 1 March 2022).
- Atwoli, L.; Baqui, A.H.; Benfield, T.; Bosurgi, R.; Godlee, F.; Hancocks, S.; Horton, R.; Laybourn-Langton, L.; Monteiro, C.A.; Norman, I.; et al. Call for emergency action to limit global temperature increases, restore biodiversity, and protect health. N. Engl. J. Med. 2021, 385, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COP26 Special Report on Climate Change and Health: The Health Argument for Climate Action. 2021. Available online: https://www.who.int/publications/i/item/9789240036727 (accessed on 1 September 2022).
- World Health Organization. Alliance for Transformative Action on Climate and Health. 2021. Available online: https://www.who.int/initiatives/alliance-for-transformative-action-on-climate-and-health/cop26-health-programme (accessed on 1 September 2022).
- U.S. Environmental protection Agency. Sources of Greenhouse Gas Emissions. 2023. Available online: https://www.epa.gov/ghgemissions/sources-greenhouse-gas-emissions (accessed on 1 March 2022).
- Tennison, I.; Roschnik, S.; Ashby, B.; Boyd, R.; Hamilton, I.; Oreszczyn, T.; Owen, A.; Romanello, M.; Ruyssevelt, P.; Sherman, J.D.; et al. Health care’s response to climate change: A carbon footprint assessment of the NHS in England. Lancet Planet. Health 2021, 5, e84–e92. [Google Scholar] [CrossRef] [PubMed]
- Dzau, V.J.; Levine, R.; Barrett, G.; Witty, A. Decarbonizing the U.S. health sector—A call to action. N. Engl. J. Med. 2021, 385, 2117–2119. [Google Scholar] [CrossRef] [PubMed]
- Alwis, A.; Limaye, S. The Costs of Inaction: The Economic Burden of Fossil Fuels and Climate Change on Health in the United States. The Medical Society Consortium on Climate & Health; Natural Resources Defense Council. 2021. Available online: https://www.nrdc.org/sites/default/files/costs-inaction-burden-health-report.pdf (accessed on 1 October 2022).
- Silva, L.; Wood, M.; Johnson, B.; Coughlan, M.; Brinton, H.; McGuire, K.; Brigdham, S. A generalizable framework for enhanced natural climate solutions. Plant Soil 2022, 479, 3–24. [Google Scholar] [CrossRef]
- Eckelman, M.J.; Sherman, J. Environmental impacts of the U.S. health care system and effects on public health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef] [PubMed]
- Healthcare Without Harm. Health Care’s Climate Footprint: How the Health Sector Contributes to the Global Climate Crisis and Opportunities for Action. Green Paper Number One 2019. Available online: https://noharm-global.org/sites/default/files/documentsfiles/5961/HealthCaresClimateFootprint_092319.pdf (accessed on 15 June 2022).
- Salas, R.N.; Maibach, E.; Pencheon, D.; Watts, N.; Frumkin, H. A pathway to net zero emissions for healthcare. BMJ 2020, 371, m3785. [Google Scholar] [CrossRef] [PubMed]
- American Hospital Association. Sustainability Roadmap for Hospitals: A Guide to Achieving your Sustainability Goals. 2015. Available online: http://www.sustainabilityroadmap.org/about/briefguide.shtml#.Y4QT8VrMKUk (accessed on 15 July 2022).
- Healthcare Without Harm. Global Roadmap for Healthcare Decarbonization. 2021. Available online: https://healthcareclimateaction.org/sites/default/files/2021-04/HCWH%20Road%20Map%20for%20Health%20Care%20Decarbonization%20-%20Introduction.pdf (accessed on 12 July 2022).
- U.S. Environmental Protection Agency. Guide to Greenhouse Gas Management for Small Business and Low Emitters. 2020. Guide to Greenhouse Gas Management for Small Business & Low Emitters. 2020. Available online: https://www.epa.gov/sites/default/files/2017-01/documents/guide_to_greenhouse_gas_management_for_small_business_low_emitters.pdf (accessed on 1 July 2022).
- Practice Green Health. Addressing Climate Change in the Health Care Setting: Opportunities for Action. Available online: https://practicegreenhealth.org/sites/default/files/pubs/epp/ClimateChange.pdf (accessed on 10 May 2022).
- Greenhouse Gas Protocol. The Greenhouse Gas Protocol: A Corporate Accounting and Reporting Standard. 2004. Available online: https://ghgprotocol.org/sites/default/files/standards/ghg-protocol-revised.pdf (accessed on 1 September 2022).
- Laustsen, G. Environment, ecosystems, and ecological behavior: A dialogue toward developing nursing ecological theory. Adv. Nurs. Sci. 2006, 29, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Tyer-Viola, L.; Nicholas, P.; Corless, I.; Barry, D.; Hoyt, P.; Fitzpatrick, J.; Davis, S. Social responsibility of nursing: A global perspective. Policy Politics Nurs. Pract. 2009, 10, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Guzmán, C.; Aguirre, A.; Astle, B.; Barros, E.; Bayles, B.; Chimbari, M.; El-Abbadi, N.; Evert, J.; Hackett, F.; Howard, C.; et al. The Planetary Health Education Framework. The Planetary Health Alliance. 2021. Available online: https://www.planetaryhealthalliance.org/education-framework (accessed on 1 April 2022).
- American Nurses Association. Code of Ethics for Nurses with Interpretive Statements; American Nurses Publishing: Silver Spring, MD, USA, 2015. [Google Scholar]
- Quitman, C.; Rainer, S.; Danquah, I.; Herrman, A. Reducing the carbon footprint of a German university hospital: Perspectives from hospital stakeholders. J. Clim. Chang. Health 2023, 12, 100247. [Google Scholar] [CrossRef]
- Quitmann, C.; Sauerborn, R.; Danquah, I.; Herrmann, A. Climate change mitigation is a hot topic, but not when it comes to hospitals’: A qualitative study on hospital stakeholders’ perception and sense of responsibility for greenhouse gas emissions. J. Med. Ethics 2023, 49, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Institute for Healthcare Improvement. Plan-Do-Study-Act (PDSA) Worksheet. 2022. Available online: https://www.ihi.org/resources/Pages/Tools/PlanDoStudyActWorksheet.aspx (accessed on 1 May 2022).
- Institute for Healthcare Improvement. The IHI Triple Aim. 2022. Available online: https://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx (accessed on 15 June 2022).
- Mortimer, F.; Isherwood, J.; Wilkinson, A.; Vaux, E. Sustainability in quality improvement: Redefining value. Future Healthc. J. 2018, 5, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, T.; Benbow, D. The Certified Six Sigma Black Belt Handbook, 3rd ed.; American Association for Quality, Quality Press: Milwaukee, WI, USA, 2017. [Google Scholar]
- Ahmed, S.; Manaf, N.H.; Islam, R. Effects of lean six sigma application in healthcare services: A literature review. Rev. Environ. Health 2013, 28, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Keil, M. The greenhouse gas emissions of a German hospital—A case study of an easy-to-use approach based on financial data. Clean. Environ. Syst. 2023, 11, 100140. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Climate Change and Social Vulnerability in the United States: A Focus on Six Impacts. 2021. Available online: https://www.epa.gov/system/files/documents/2021-09/climate-vulnerability_september-2021_508.pdf (accessed on 10 April 2022).
- U.S. Environmental Protection Agency. Lean and Energy Toolkit. Lean & Energy Toolkit: Contents & Acknowledgements | US EPA. 2021. Available online: https://nepis.epa.gov/Exe/tiff2png.cgi/P1001XIJ.PNG?-r+75+-g+7+D%3A%5CZYFILES%5CINDEX%20DATA%5C06THRU10%5CTIFF%5C00000264%5CP1001XIJ.TIF (accessed on 1 July 2022).
- Minnesota Chamber of Commerce. Energy Smart. Available online: https://www.mnchamber.com/your-opportunity/energy-smart (accessed on 1 May 2022).


{kind=link}
{kind=link}
| Emissions Type | 2021 | 2022 | CO2e Emissions |
|---|---|---|---|
| Scope 1 Emissions | |||
| Stationary Combustion | 224 | 185 | CO2-e (MT) |
| Mobile Sources | 345 | 345 | CO2-e (MT) |
| Refrigeration/AC Equipment Use | 57 | 57 | CO2-e (MT) |
| Anesthetic Gases | 92 | 60 | CO2-e (MT) |
| Location-Based Scope 2 Emissions | |||
| Purchased and Consumed Electricity | 15,617 | 13,329 | CO2-e (MT) |
| Purchased and Consumed Steam | 12,220 | 10,927 | CO2-e (MT) |
| Market-Based Scope 2 Emissions | |||
| Purchased and Consumed Electricity | 8963 | 7650 | CO2-e (MT) |
| Purchased and Consumed Steam | 12,220 | 10,927 | CO2-e (MT) |
| Total Scope 1 and Location-Based Scope 2 | 28,462 | 24,842 | CO2-e (MT) |
| Total Scope 1 and Market-Based Scope 2 | 21,808 | 19,164 | CO2-e (MT) |
| Item 8. What Are the Organizational Barriers to Developing and Maintaining a GHG Inventory? | |
|---|---|
| Pre-survey answers | Post-Survey Answers |
● “Time” | ● “None” |
● “Time and manpower” | ● “Time and staff” |
● “We need a sustainability expert to guide this work. We currently do not have this.” | ● “We need a committed person whose sole work is this” |
● “Manpower and high regulatory standards make change difficult” | ● “Energy meters” |
● “Resources” | ● “I do not believe we have barriers” |
| Survey Item | Pre-% | Post-% |
|---|---|---|
| 1. How do you rate your knowledge of greenhouse gases (GHG)? | ||
| None | 0 | 0 |
| Very little | 50 | 20 |
| Moderate | 50 | 80 |
| Very knowledgeable | 0 | 0 |
| 5. How do you rate your experience with GHG accounting/maintaining a GHG inventory? | ||
| None | 0 | 0 |
| Beginner | 100 | 80 |
| Moderate | 0 | 20 |
| Expert | 0 | 0 |
| 6. From your perspective, how important is it that the MAMC maintain an inventory of GHG to monitor emissions? | ||
| Extremely important | 60 | 40 |
| Somewhat important | 20 | 60 |
| Neutral | 0 | 0 |
| Somewhat not important | 0 | 0 |
| Extremely not important | 20 | 0 |
| 7. From your perspective, how important is it that the MAMC strives to reduce GHG emissions? | ||
| Extremely important | 50 | 40 |
| Somewhat important | 25 | 60 |
| Neutral | 0 | 0 |
| Somewhat not important | 0 | 0 |
| Extremely not important | 25 | 0 |
| Survey Items |
|---|
| 1. How do you rate your knowledge about greenhouse gases (GHG)? |
| 2. Scope 1 emissions include ____? |
| 3. Scope 2 emissions include ____? |
| 4. Scope 3 emissions include ____? |
| 5. How do you rate your experience with GHG accounting/maintaining a GHG inventory? |
| 6. From your perspective, how important is it that the MAMC maintain an inventory of GHG to monitor emissions? |
| 7. From your perspective, how important is it that the MAMC strives to reduce GHG emissions? |
| 8. What are the organizational barriers to developing and maintaining a GHG inventory? |
| 9. GHGs contribute to climate change, which negatively impacts human health. T/F |
| 10. Developing a sustainability program at the MAMC is…? |
| 11. Which answer best describes how you feel about learning about GHG emissions and having the GHG inventory process be part of your work? |
| 1. | How do you rate your readiness to maintain the GHG inventory process after receiving training? |
| 2. | After receiving training on the GHG inventory process, how prepared do you feel to teach the process to others? |
| 3. | After participating in the Reducing GHG Emission project, can you identify two methods to begin reducing GHG emissions at the organization? |
| 4. | Please list 2 ways that we can reduce GHG emissions at our organization. |
| 5. | How has your understanding of the links between GHG emissions, climate change, and human health grown? |
| Item 15. List 2 Ways That We Can Reduce GHG Emissions at Our Organization. |
|---|
● “LED light bulbs, better recycling” |
● “LED lighting, solar” |
● “LED lights, alternative fuels for vehicles” |
● “Reduction of electrical and gas” |
● “For an immediate impact transition to LED lighting and community-based solar” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bjorgaard, J.; Potter, T. Reducing Environmental Impacts at a Midwestern Academic Medical Center: Making Carbon Emissions Reduction a Reality. Challenges 2023, 14, 42. https://doi.org/10.3390/challe14040042
Bjorgaard J, Potter T. Reducing Environmental Impacts at a Midwestern Academic Medical Center: Making Carbon Emissions Reduction a Reality. Challenges. 2023; 14(4):42. https://doi.org/10.3390/challe14040042
Chicago/Turabian StyleBjorgaard, Johannah, and Teddie Potter. 2023. "Reducing Environmental Impacts at a Midwestern Academic Medical Center: Making Carbon Emissions Reduction a Reality" Challenges 14, no. 4: 42. https://doi.org/10.3390/challe14040042
APA StyleBjorgaard, J., & Potter, T. (2023). Reducing Environmental Impacts at a Midwestern Academic Medical Center: Making Carbon Emissions Reduction a Reality. Challenges, 14(4), 42. https://doi.org/10.3390/challe14040042