

Collagen as a Biomaterial for Skin and Corneal Wound Healing
by
 ,
,
Renáta Sklenářová
1,2,
Naoufal Akla
2,3,
Meagan Jade Latorre
2,
Jitka Ulrichová
1 and
Jana Franková
1,* 1
Department of Medical Chemistry and Biochemistry, Faculty of Medicine and Dentistry, Palacký University in Olomouc, 775 15 Olomouc, Czech Republic
2
Maisonneuve-Rosemont Hospital Research Centre, Montréal, QC H1T 2M4, Canada
3
Department of Ophthalmology, Université de Montréal, Montréal, QC H3C 3J7, Canada
*
Author to whom correspondence should be addressed.
J. Funct. Biomater. 2022, 13(4), 249; https://doi.org/10.3390/jfb13040249
Submission received: 24 October 2022
/
Revised: 11 November 2022
/
Accepted: 15 November 2022
/
Published: 16 November 2022
(This article belongs to the Special Issue Feature Papers in Biomaterials for Tissue Engineering and Regenerative Medicine)
Abstract
:The cornea and the skin are two organs that form the outer barrier of the human body. When either is injured (e.g., from surgery, physical trauma, or chemical burns), wound healing is initiated to restore integrity. Many cells are activated during wound healing. In particular, fibroblasts that are stimulated often transition into repair fibroblasts or myofibroblasts that synthesize extracellular matrix (ECM) components into the wound area. Control of wound ECM deposition is critical, as a disorganized ECM can block restoration of function. One of the most abundant structural proteins in the mammalian ECM is collagen. Collagen type I is the main component in connective tissues. It can be readily obtained and purified, and short analogs have also been developed for tissue engineering applications, including modulating the wound healing response. This review discusses the effect of several current collagen implants on the stimulation of corneal and skin wound healing. These range from collagen sponges and hydrogels to films and membranes.
1. Introduction
The skin and cornea form the outer barrier of the body, providing protection against external influences. Being superficially located, skin and corneal injuries may result from severe infection, burns, physical or chemical trauma, and ultraviolet damage. Although they have similar anatomic structures (e.g., the dermis and stroma are both connective tissues, while the epidermis and corneal epithelium are composed of stratified epithelia [1]), their wound healing mechanisms differ. Severe injuries can result in scarring due mainly to uncontrolled deposition of injury stimulated extracellular matrix (ECM), mainly collagen. To avoid scarring or to allow for scar revisions, a range of natural and artificial polymers based on collagen have been developed to modulate wound healing [2,3,4,5].
Wound healing is an important physiological process, consisting of several phases leading to tissue regeneration after trauma. The wound healing process is complex and depends on the coordinated presence of multiple types of cells, growth factors and cytokines that regulate many cellular processes including growth, migration, differentiation, survival, homeostasis, and morphogenesis [6]. The ECM, discussed in more detail below, also plays an important structural role in this process [7].
The most abundant protein present in the human and mammalian body is collagen, and due to its structural role, is also the most widely used protein for tissue engineering of scaffolds [8,9]. Collagens are found in a wide range of organisms [10]. They can be categorized into fibrillar (e.g., collagens I, II, III) and non-fibrillar types (e.g., collagen IV, collagen-like proteins). The fibrillar collagens provides a highly biocompatible and structural environment for cells, tissues and organs with form, stability, and connectivity [11]. Due to its properties, such as its high tensile strength, controllable biodegradability, biocompatibility, availability and the high versatility of its in vitro and in vivo applications [1], it is suitable for the preparation of medical implants such as dressings for burns/wounds, corneal implants, bone filling materials and drug delivery systems. In tissues, collagen is the scaffold material that provides an optimal environment for highly physiologically active cells and cellular components [12].
Currently, biomedical companies manufacture many implants from collagen-rich tissues derived from human or animal sources [13]. These implants differ in structure, crosslinking technology, collagen sources and species and sterilization techniques [14,15,16]. Due to these unique properties, this review discusses the influence of collagen in the cornea and skin in wound healing. Furthermore, its main focus is on collagen-based materials, which are currently being developed, have excellent biocompatible properties and can be further modified. These materials can be used in ophthalmology or in the healing of skin wounds, as a non-immunogenic implant replacing the transplantation of donor cornea or skin tissue.
2. Extracellular Matrix
The ECM is a non-cellular structure that surrounds the cells in all tissues. The ECM in mammals comprises approximately 300 [17] proteins that are differentially distributed in individual tissues [18,19,20,21]. The ECM proteins interact with cells and regulate many functions, such as cell proliferation, migration and differentiation [17]. Matrix components bind each other, as well as cell adhesion receptors, forming a complex in all tissues and organs where cells are present. This highly dynamic structural network is mainly composed of proteins (e.g., collagen, elastin, laminin, fibrillin, fibronectin [7,22,23,24,25]) and proteoglycans (e.g., hyaluronate, dermatan sulfate, heparan sulfate, keratan sulfate, and chondroitin sulfate [26]), (Figure 1).
Cell adhesion to the ECM is mainly mediated by integrins. Integrins function as transmembrane receptors and mediate the interaction between the cell cytoskeleton and ECM proteins. [27]. They are capable of interacting with proteins and various signaling molecules [28]. Due to these interactions, integrins can regulate many cellular functions such as cell adhesion, migration, growth and differentiation, and, consequently, can influence the process of tissue repair or regeneration [29,30,31]. Each integrin is composed of two noncovalently-associated transmembrane glycoprotein subunits that are a combination of one to 18 unique α and one to eight β subunits, to form 24 distinct dimers that bind to specific sites of ECM proteins. Integrins αβ heterodimers are divided into four classes (leukocyte, collagen-, Arg-Gly-Asp (RGD)- and laminin-binding integrins) [32]. The α1β1, α2β1, α3β1, α10β1 and α11β1 integrins with characteristic β1 subunits, constitute a subset of the integrin family with an affinity for collagens. Collagen-binding integrins have important functions with respect to the wound healing process: α2β1 affects thrombus formation and α11β1 is a main collagen receptor for collagen remodeling on activated fibroblasts in wounds, fibrotic tissues and the tumor stroma [33]. Therefore, controlling specific cell–ECM interactions offers the possibility to modulate distinct phases of the healing process.
The group of proteins that we will focus on in more detail in this review are collagens. Collagens are the main structural components in various connective tissues and determinants of their tensile strength. Collagens constitute nearly 33% of protein in humans [34]. The structure of collagen consists of three polypeptide chains—α chains—that can form right-handed triple helices, comprising Gly-X-Y repetitions [9]. At positions X and Y, proline and hydroxyproline are often found. The triple helix is stabilized by hydrogen bonds and electrostatic interactions [9,35]. According to their properties, collagens can be divided into several groups: fibril-forming collagens, fibril-associated collagens with interrupted triple helices, network-forming collagens, collagens VI, VII, XXVI and XXVIII, membrane collagens and multi-plexins (collagen XV and XVIII) [8].
Collagens type I and III (fibrillar collagens) are the main structural elements of the dermis followed by fibril-associated collagens type XII, XIV, XVI, and VI [8]. However, the content and distribution of collagens type I and III in the skin varies with age [23]. In the cornea, the major fibril-forming collagens of the ECM are types I and V. The minor collagen types such as collagen III, IV, VII and VIII, are essential in other corneal structures such as basement membranes (BM) and during ECM remodeling [36]. More specifically, collagen type VII anchoring fibrils ensure the adhesion of the epithelium to the underlying structures [37] while disruption of collagen type IV, one of the BM’s principal components, has been shown to lead to several physiological and clinical abnormalities including corneal visual impairments in humans involving corneal opacification [38].
A recent study has shown that collagen type I can bind inflammatory interleukins (IL) such as IL-1β, IL-6, and IL-8 and is capable of forming a physiological wound milieu that supports the healing process [39]. Moreover, collagen type I has exhibited a binding capacity for elastase and matrix metalloproteinase 2 (MMP-2) [40,41].
3. The Wound Healing Process
3.1. Skin Wound Healing
The skin represents the first barrier protecting the body against injury. Its upper layer, the epidermis, consists mainly of keratinocytes, while the inner, the dermis, consists mainly of fibroblasts [42]. Wound healing is a complex process (Figure 2) involving several successive phases that overlap to some degree: haemostasis, inflammation, proliferation and tissue remodeling [43]. Haemostasis consists of several steps that concludes with the formation of a fibrin clot.
In vertebrates, almost every cell (with exceptions of avascular tissues such as the cornea) is located within a distance of 100 microns from a capillary. In the highly vascularized skin, the capillaries are damaged during injuries [44,45]. The first step is a localized transient vasoconstriction of blood vessels to limit blood loss, followed by activated thrombocytes binding to exposed collagen and endothelial lining to form a platelet plug. This temporary seal is further solidified by the intrinsic and extrinsic coagulation clotting cascade which forms a more robust fibrin mesh at the wounded site [45,46]. These processes are assisted by multiple sources and chemical mediators including endothelin, serotonin, Von Willebrand factor, Adenosine diphosphate, integrins and collagen-binding glycoprotein VI as well as the release of chemotactic and growth factors such as transforming growth factor β (TGF-β), contributing to the restoration of normal homeostasis after trauma [47,48,49].
The inflammatory response and phagocytosis stimulated by the wounding acts to clear pathogens, foreign bodies or damaged tissue present in the wound [49] allowing for repair through proliferation and remodeling that involves interactions between ECM and cells. Once bleeding has stopped, the phase of inflammation is established by the widening of blood vessels. This hyperemic state is initiated by locally released chemicals from plasma, damaged cells, or pre-formed cellular or synthesized pro-inflammatory mediators [46]. These factors act to increase blood flow and permeability to plasma molecules and immune cells within the wound [50]. This is paramount to support anabolic processes necessary to fully perfuse and repair damaged tissues by providing oxygenation and nutrients for new tissue to arise [50,51,52]. Pattern recognition receptors (PRRs) can sense damage- or pathogen-associated molecular patterns (DAMPs and PAMPs) and promote the release of many proinflammatory cytokines [53,54]. The release of inflammatory cytokines and growth factors, such as IL-1, IL-6, IL-8, TNF-α, platelet derived growth factor (PDGF) and endothelial cell growth factor (VEGF), increase the influx of inflammatory cells [50]. Vascular permeability in and around the injured tissue facilitates the infiltration of leukocytes (neutrophils and monocytes) that clean up the wound by phagocytizing cell debris and pathogens in the interstitial space. The presence of elevated cytokines and growth factors support the migration and proliferation of skin cells and the synthesis of ECM molecules necessary for wound regeneration [55]. In the injured skin, matrix metalloproteinase 1 (MMP-1) production is also induced by keratinocytes that bind to type I collagen in the dermis through α2 and β1 integrins [56]. Overproduction of these degradative matrix metalloproteinases (MMPs) could damage host healthy tissue around the wound area [57].
After a few days, a transition from the inflammatory phase to the proliferation phase is necessary for tissue formation and efficient wound closure. Tissue remodeling and establishment of new blood vessels through angiogenesis is critical in wound healing and takes place concurrently during all phases of the reparative process [51]. The onset of angiogenesis is upregulated by several factors, mainly VEGF and TGF-β [51]. Another protein that strongly stimulates this process is collagen type I. It appears that the binding of α1β1/α2β1 integrin receptors on the surface of endothelial cells is crucial for its angiogenic activity [58]. Fibroblasts that migrate into the wound contribute to granulation tissue formation. Granulation tissue is composed of new connective tissue and tiny blood vessels that proliferate profusely and produce the matrix proteins [59]. Subsequently, fibroblasts transform into contractile myofibroblast phenotypes that attach to fibronectin and collagen in the extracellular matrix [60]. In the proliferative phase, the key event is the production of TGF-β that affects the transcription genes of collagen, decreases the production of MMPs and increases the levels of protease inhibitors—TIMPs [61]. The reepithelization process, which is important for restoring an intact epidermis, is mainly provided by keratinocytes which migrate along the fibrin blood clot and on to the surface of the granulation tissue [62].
3.2. Corneal Wound Healing
While both the skin and cornea are ectoderm-derived, the cornea possesses two striking differences, its optical transparency and avascularity [4]. The cornea is also the most innervated and sensitive tissue in the human body [65,66]. It consists of three main cellular layers—an outermost epithelial layer, middle stroma layer and an innermost endothelial layer [67] (Figure 2). These layers are separated by acellular layers, the Bowman’s membrane between the epithelium and stroma and the Dua’s (pre-Decemet’s layer) and Descemet’s membrane (DM) between the stroma and endothelium. Each cellular layer has different regenerative capacities and differ in their involvement in corneal wound healing. There is well-documented cross talk between epithelial and stromal cells during the wound healing process that leads to restoration of corneal integrity [65]. Maintaining corneal transparency and avascularity during wound healing is essential to preserve optimal vision [66,68].
The inflammatory response paradigm of the cornea differs from that of the skin as multiple anti-angiogenic molecules normally present in the cornea contribute to its “avascular privilege”. The avascularity also contributes to its “immune privilege”, also referred to as “lymphangiogenic/haemangiogenic privilege” as there are very few mature immune cells within the cornea [69]. It has been reported that the expression of soluble VEGF receptors in the healthy cornea (e.g., sVEGFR-1, -2, -3) [4,70], binds and inhibits the activity of vascular VEGF and prevents the in-growth of blood vessels or lymphatics [71]. Other growth factors that contribute to the avascularity and immune privilege include thrombospondins (TSP-1 and TSP-2) [72] and PEDF [73]. Anatomical components such as the ECM-dense0 collagen fibers and derived bioactive precursor fragments such as endostatin, tumstatin, arresten, canstatin, neostatin, restin and angiostatins also maintain the barrier to vessels and immune cells [71]. Anti-angiogenic factors found in the aqueous humor and the limbal region are also thought to contribute to the avascular nature of this tissue [71,74,75].
The sensitive dynamic between pro-angiogenic and anti-angiogenic substances can promote or inhibit corneal haemangiogenesis and lymphangiogenesis. Important orchestraters of this delicate equilibrium are MMPs. More than 16 MMPs have been identified in the cornea which include collagenases (e.g., MMP-1, 8 and 13) gelatinases (e.g., MMP-2 and 9) and membrane type MMPs (e.g., MMP-14) which can act as either pro or anti-angiogenic modulators [76]. In some corneal pathologies (infection, inflammation, ischemia, degeneration, trauma, surgery, herpes) [77], the balance can be shifted towards the pro-angiogenic status if sustained, leading to neovascularization [71,74,78]. In such cases of inflammation and severe pathology, the immune privilege of the cornea is gone [79]. A key molecule involved in pathogenic corneal neovascularization is VEGF [80]. Expression of VEGF has been attributed to stimulation by inflammatory cytokines, notably interleukins-1,6 and tumor necrosis factor-alpha (IL-1, IL-6, TNF-α) [81,82,83]. Interestingly in some pathologies, corneal neovascularization occurs in parallel with epithelial hyperplasia, disruption of the Bowman layer, disorganized stromal collagen fibers and fibroblast activation [4].
3.2.1. Corneal Epithelial Healing
Corneal epithelial wounding can stimulate an acute inflammatory response at the limbus leading to the accumulation of leukocytes, the migration of neutrophils, dendritic cells and macrophages, and the influx of lymphocytes within the stroma and the wounded epithelium [65,84].
The entire corneal epithelium can be replenished in approximately seven to ten days [4,85]. This process is accelerated when the injury is superficial such as with most corneal abrasions that heal without any complications [4,86]. Stem cells and, in particular, progenitor cells such as the transient amplifying cells of the limbal epithelium contribute to the rapid healing [82,86,87,88]. Corneal epithelial wound healing involves several key phases: adhesion of the ingrowing cells to the BM, migration to cover the wound, cell proliferation and differentiation [87,89,90]. The epithelium and keratocytes around the wound remain viable after a surface injury and reconstitute a new BM. However, they will undergo apoptosis or necrosis in severe damage or deep wounds, prolonging the wound closure [68,91]. While several major collagen types are differentially distributed across all corneal layers, the BM is composed mainly of collagen type IV which provides adherence to epithelium [92], other types may also be found (IV, VII, XII, XV, XVII, XVIII) and play an important role in the morphology and pathology of corneal disease [37]. The collagen of the underlying Bowman layer, consisting mainly of collagen types I, followed by III, V and XII, does not regenerate after injury by keratocytes, but can be substituted by a structurally different Bowman’s-like layer [92,93].
3.2.2. Corneal Stromal Healing
In continuum with the Bowman’s layer is the corneal stroma. It is the thickest layer of the cornea that is made mostly of collagen fibrils (types I and V) [92,94]. Epithelial and stromal cells interact through the BM. The first stromal response after epithelial or epi-stromal injury is mediated by IL-1 and TNF-α release and is characterized by keratocyte apoptosis in the area of the injury. This is followed by the activation of adjacent quiescent stromal keratocytes and their conversion into fibroblasts [68,95]. In addition to apoptosis, in some cases, such as in severe alkali burns, necrosis can occur [96]. The release of IL-1, TNF-α, IL-6, CXC chemokines, and MCP-1 by the injured cells promotes the infiltration of inflammatory cells into the wound area [4,68,97]. Within 24 hours, activated fibroblasts migrate to the wound, subsequently proliferate and then trans-differentiate into contractile opaque myofibroblasts, the prominent repair phenotype [95] mediating wound closure and contraction [4]. To facilitate tissue repair and wound closure, the differentiated myofibroblasts proliferate and migrate towards the site of injury and deposit excessive amounts of ECM collagen, including type I, III, IV, and V and matrix stabilizing proteoglycan [36]. Fibroblasts and myofibroblasts deposit several components of the ECM including collagen type III, fibronectin, tenascin, elastin and proteoglycans which enables the migration of fibroblasts [4,68,98]. Although still debated [99], collagen III is weakly expressed in the normal cornea, but its expression increases several-fold during wound healing. It forms fibers by association with collagen type I and therefore serves as one of the main markers of stromal matrix remodeling observed after corneal injury [100]. However, as large amounts of collagen III are not normally present in stroma, its elaboration after stromal injury may interfere with collagen fibril lamellar assembly during remodeling and contribute to scar formation [68,101]. During corneal wound healing, the abnormal deposition of the various types of collagens at the wrong place or the wrong time including types III, IV and XII are responsible for corneal opacities and scarring [68,101].
Multiple factors influence either a regenerative or fibrotic healing outcome. These include multiple secreted growth factors, particularly the TGFβ’s from the epithelium, tears and to a lesser extent the stromal cells. Normal levels of these regulators are reestablished with BM regeneration during physiological corneal repair after wound closure, after which myofibroblasts undergo apoptosis. Persistence of wound healing growth factors and myofibroblasts can otherwise result in uncontrolled disorganized matrix secretion in which there is excess collagen deposition. The resulting disorganized matrix becomes resistant to collagenase remodeling, leading to scarring and haze [68,95,102,103,104]. Myofibroblast persistence also hinders the regenerative capacity of the cornea including the BM and corneal nerves [68]. Corneal fibrosis is considered irreversible with few preventive options and may require surgery or transplantation, if human donor corneas are available [103]. Corneal stromal regeneration is very slow and can take months or years. The normal form and function of the stroma are slowly restored by the removal of infiltrating inflammatory cells, resorption of abnormal scar ECM, and, finally, repopulation of stroma by keratocytes and elaboration of ECM components found in the healthy cornea [68].
3.2.3. Corneal Endothelial Healing
The human corneal endothelium separates the aqueous humor from the rest of the corneal layers [105]. It consists of a flattened monolayer resting on a basal membrane called Descemet’s membrane, which itself lies next to the recently discovered Dua’s layer [106]. Relative to the BM, DM has reduced regenerative capacity and is mainly composed of non-fibrillar collagens type VIII and type IV produced by corneal endothelial cells [100,107,108]. However, only collagen IV remains adjacent to endothelial cells in both infant and adults, while collagen VIII becomes displaced towards the stromal side with age [108]. The integrity of the corneal endothelium and DM are critical for the corneal fluid homeostasis that in turn controls corneal transparency. The endothelium is responsible for the bidirectional exchange between the cornea and aqueous humor of fluids, nutrients and bioactive molecules such as growth factors or cytokines [100,105,107,108]. Extensive loss of endothelial cells caused by disease, injury or aging can lead to corneal edema due to excessive fluid accumulation [4]. Corneal endothelial cells have very limited regenerative potential and proliferative capacity, but they can nevertheless expand, migrate and undergo endothelial–mesenchymal transition (EnMT) acquiring a phenotype to repair wounds [4,36,65,100]. This transformation is mediated by factors such as TGF-β, FGF-2, IL-1 and involves NFκB activation and upregulation of collagen type I. In severe pathologies such as alkali burns or infections, EnMT results in aberrant ECM deposition posterior to DM and endothelial fibrosis that leads to sight threatening complications [4,68,108,109,110,111].
Figure 2.
The Wound healing process. Wound healing is an important physiological process to maintain the integrity of the skin or cornea after trauma. Diagram (A) shows the course of skin healing—individual phases such as hemostasis, inflammation, proliferation and skin remodeling. Figures created with BioRender.com (accessed on 1 October 2022). (A) Modified according to Ref. [112] and (B) [95].
Figure 2.
The Wound healing process. Wound healing is an important physiological process to maintain the integrity of the skin or cornea after trauma. Diagram (A) shows the course of skin healing—individual phases such as hemostasis, inflammation, proliferation and skin remodeling. Figures created with BioRender.com (accessed on 1 October 2022). (A) Modified according to Ref. [112] and (B) [95].

4. Biomaterials
Because the human body has limited regenerative capabilities, current treatment options to replace damaged tissue and organs is by donor tissue and organ transplantation [113]. Over the last two decades, research efforts in the field of regenerative medicine and tissue engineering have increasingly focused on the replacement of transplantation using bioimplants made of biocompatible materials. Individual biomaterials are used in different ways, depending on their applications and location e.g., hydrogels or scaffolds that are made of 3D bioprinted tissue [108] and are designed based on understanding of the process of healing individual tissues. Basically, these materials must not be toxic and must be biocompatible with the patients’ tissues [114]. Prepared materials need to have mechanical, chemical, or physical properties that are appropriate for those of the target organ, as well the ability to promote seamless integration into the host. Many of these materials contain main proteins of the ECM, such as collagen, fibronectin or ECM´s polysaccharides [115,116].
5. Collagen Biomaterials for Wound Healing
Collagen is the most common protein in the human body and is suitable for the production of biomaterials used in tissue engineering [117]. It contributes to the mechanical strength and elasticity of tissues and acts as a natural substrate for cellular attachment, proliferation, and differentiation. It can mediate a lot of pro-regenerative physiological interactions during the complex wound healing process ranging, from angiogenesis to re-epithelialization [117]. In addition, it can bind and inactivate excessive amounts of MMPs that occur in non-healing wounds [118,119]. Excellent biocompatibility and intrinsic biodegradability by endogenous collagenases make exogenous collagen ideal biomaterial for use in biomedical applications [120]. Collagen-based biomaterials can be classified into two categories—i) decellularized collagen matrices that retain the original tissue properties and ECM structure, and ii) scaffolds prepared via extraction, purification, and collagen polymerization [1,121]. All prepared biomaterials must meet the limits of assessment of biocompatibility and toxicity of the material, in vitro and subsequently in vivo.
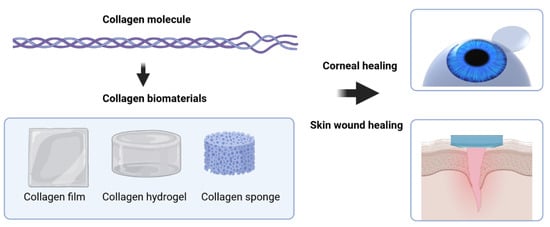
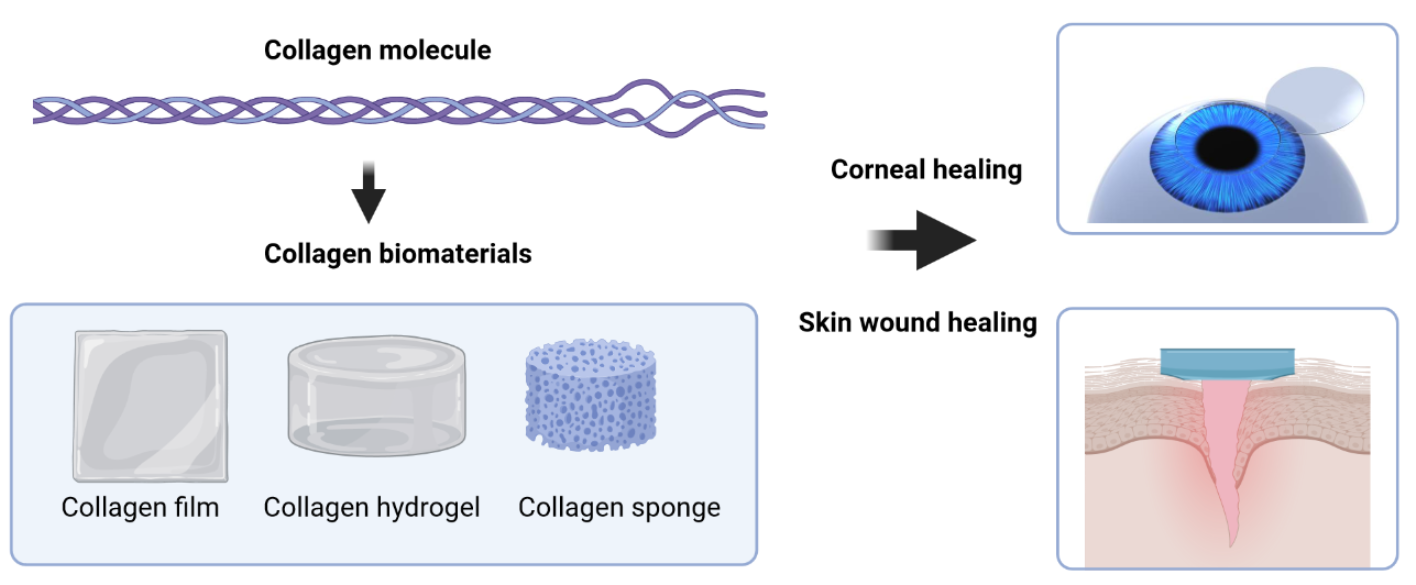
The final biological application of collagen products depends on the type of the injury and biomaterial character. Frequently used forms of biomaterial (Figure 3) include gels, membranes, sponges, hollow fiber tubing and spheres [120]. Examples of commercial collagen products for skin healing are presented in Table 1.
Collagen for use as biomaterials in wound healing and regenerative medicine are also within the research realm and are being developed and tested in various forms for use in skin and corneal wound healing. There are numerous variations, so only a selection will be discussed.
Currently, nano forms of collagen are also being explored, produced by electrostatic spinning, which has advantages over the conventional three-dimensional (3D) design of collagen, mainly due to its nanoscale, which contributes to a higher surface-to-volume ratio and helps to withstand large loads with minimal stress [132].
The ideal materials for cornea healing should replicate the properties of the natural cornea and show seamless biointegration with host tissues, be resistant to infection, have excellent optical properties [133]. The commercial biomaterials-based implants that allow corneal vision restoration after limited wound healing include the keratoprostheses (KPros) or artificial corneas. KPros that are currently used are the Boston type 1 keratoprosthesis (Boston KPro-1) for eyes with good ocular surface and the Osteo-odonto-keratoprosthesis (OOKP) and Boston KPro-2 for treatment of dry eyes and damaged ocular surfaces based on polymethylmethacrylate (PMMA) [133,134]. However, because of their very limited capacity for regeneration and the prevalence of severe side effects, these are only used in end-stage eyes. Presently, research has focused primarily on the production of collagen-based or inspired corneal implants that promote regeneration. The most common collagens are type I and III in the form of hydrogels, which have already been evaluated in clinical trials. In vitro tests of collagen sponges are also in progress [134,135,136].
5.1. Collagen Sponges
Commercial collagen sponges are insoluble, prepared mostly by lyophilized aqueous collagen solutions. Their use reduces the formation of scarring and promotes hemostasis, so they are used as a biomaterial for skin wound healing [137,138,139]. These sponges are capable of absorbing large amounts of tissue exudate, and will adhere to a wet wound, maintain a moist environment and protect wounds from mechanical trauma and bacterial infection [140]. Implanted collagen sponges are infiltrated with tissue containing glycosaminoglycans (GAGs), fibronectin, and new collagen, followed by various cells (e.g., sponge implantation in burn wounds leads to a rapid recovery of the skin due to an intense infiltration of neutrophils in the sponge) [141]. These sponges are also effective depots for the storing and releasing of exogenous growth factors (such as TGF [142]) to wounds and are also suitable for the short-term delivery of antibiotics. They are especially useful in wound healing because their wet-strength allows for them to be sutured to soft tissue and provides a template for new tissue growth. Immunohistochemistry results published by Chang at al. showed that collagen type I and III expression was increased in the wounds treated with collagen-containing sponges [143]. Regeneration of the epidermis and collagen fiber deposition was observed also in a study by Cheng at al., where they used a collagen sponge with carboxymethyl chitosan on burn wounds [144].
5.2. Hydrogels
Hydrogels are aggregates of hydrophilic polymers that can absorb or contain large amounts of fluids, even ≥90% of water [147,148]. Collagen hydrogels are often considered the most promising wound healing candidate owing to their mechanical properties, gelling ability, stability, biocompatibility and low toxicity [122]. These hydrogels have a wide range of uses, they present a large uniform surface area for supporting cell growth and their high water content allows for the exchange of gases, nutrients and waste products and helps them serve as depots for drugs. Sturdier hydrogels can also act as barriers against bacterial contamination [149]. Another advantage of the hydrogel over conventional wound dressings is their reported capacity for reducing pain through a cooling effect, while injectable hydrogels have low adhesion to the tissue and do not cause pain when removed [129]. Collagen hydrogels often incorporate other biological matrix molecules such as glycoasminoglycans (GAGs). Based on the type of GAGs used (hyaluronic acid (HA), heparin, heparan sulfate (HS), chondroitin sulfate (CS), dermatan sulfate (DS), and keratan sulfate (KS)), the hydrogels have different functionalities for in vivo use [121]. Collagen-hyaluronan-based hydrogels have also been used to develop in vitro organotypic models to mimic healthy or malignant extracellular matrices [150].
Injectable hydrogels, which have good fluidity and consist of collagen I and hyaluronic acid (COL-HA), have been proposed for non-healing wounds [151]. Collagen has been modified with a number of other substances to ensure that the bioimplants have good mechanical properties. Fabrication of three-dimensional (3D) composite scaffolds based on collagen and chitosan in different proportions have been reported [152]. Chitosan–collagen hydrogels have good haemostatic (blood coagulation) capacity and make promising wound dressing [153,154]. These hybrid hydrogels possess good thermal stability, injectability, and pH sensitivity [155] and have superior mechanical strength compared to chitosan-only hydrogels [156].
Plastic compressed type I collagen hydrogels with incorporated keratinocytes and fibroblasts are being tested in a phase two clinical trial as denovoSkinTM [157,158]. These constructs are characterized by an epidermis that is properly stratified during transplantation, appear to develop a functional basement membrane and dermo-epidermal junction, and exhibit an almost normal functional dermis [157].
Collagen hydrogels are also being examined for use in ophthalmology [159,160]. Collagen type I, the primary molecule of the native cornea, is a suitable biomaterial for corneal tissue engineering applications. These hydrogels are frequently used as models for studying neovascularization in the cornea. The importance of collagen I in angiogenesis is evident because collagen degradation releases proangiogenic factors [161,162]. Furthermore, the type of collagen used has an impact on the physical properties of the final product. For instance, the addition of soluble tropocollagen improves transparency and strength. While collagen (type I and type III) hydrogels have comparable tensile strength and elasticity, collagen type III hydrogels tend to be slightly mechanically and optically superior [163].
Several in vitro and in vivo studies have reported that short ECM-mimicking peptides can stimulate regeneration in a range of organ systems. As an alternative to full-length collagen, short collagen-like peptides (CLPs) have been used to fabricate soft hydrogels [154] or have been conjugated to synthetic polymer for better mechanical strength as implants [164,165].
One synthetic polymer that is commonly used to conjugate CLP is polyethylene glycol (PEG) which is chemically inert [164,166,167]. CLP-PEG implants can be enhanced with 2-methacryloyloxyethyl phosphorylcholine (MPC), an artificial lipid that suppress the inflammation. The resulting CLP-PEG-MPC implants improved the reduction of corneal swelling, haze, and neovascularization in comparison with CLP-PEG implants [136]. PEG–collagen hydrogels also enable the encapsulation of viable mesenchymal stem cells (MSCs) that could be a promising method in cases of ocular inflammatory diseases, such as alkali burn injury [167].
Full-length recombinant human collagen type III (RHCIII), which behaves like native collagen, has been used to fabricate implants on their own, or as composites with polymers of MPC. The resulting RHCIII–MPC hydrogels are robust and have been shown to allow precision femtosecond laser cutting to produce complementing implants and host surgical beds for subsequent tissue welding [168]. Another material suitable for femtosecond laser surgery is a bioengineered porcine collagen (BPC) platform based on high-purity, medical-grade collagen extracted from porcine skin. The BPC is highly compatible with cell ingrowth and has favorable optical and mechanical properties. It can replace a portion of the native corneal stroma with rapid wound healing promoting a transparent cornea [160]. However, xenogeneic materials extracted from animals must be used cautiously as they can cause severe allergies [169], or as seen in the recent COVID-19 pandemic, zoonotic transmission can occur [170].
5.3. Other Applications: Films and Membranes
Collagen is one of the most effective materials for the preparation of membranes and films, due to their ease of manufacture. Collagen membranes that are mechanically strong have been widely used in medicine and dentistry, due to their high biocompatibility and resorbability [119]. Recently, biodegradable collagen membranes have been applied in guided bone regeneration with comparable outcomes to non-resorbable membranes [171]. Many collagen films are prepared by a process of crosslinking and some of these are mixed with other polymers that improve their properties. Currently, one of the most studied films for wound healing are collagen–chitosan films that are doubly crosslinked, e.g., using tannic acid and genipin. When compared with other collagen–polymer blends or to pure collagen, they show higher antimicrobial activity and improved physicochemical properties [172]. These membranes and films can be hydrated to allow the exchange of gases (such as O2 and CO2). Such dual crosslinked polymeric films are being increasingly examined for use in ophthalmology, especially as temporary implants for injured corneas [173]. Moreover, films combining collagen with hyaluronic acid or with chitosan have found applications in cosmetics and tissue engineering [153,174].
An overview of the currently developed material discussed in this review (mentioned in Section 5.1, Section 5.2 and Section 5.3) is also given in Table 2.
6. Conclusions
This review highlights several examples of collagen-based or inspired biomaterials that are being used for skin and corneal tissue wound healing and regenerative medicine. These biomaterials are well-tolerated, facilitate rapid wound closure, promote cell proliferation and also the formation of new ECM in a very short time. In addition, collagen-based biomaterials can be modified by bioactive substances to suppress inflammatory responses. They can also be combined with other materials to fine-tune the physical, chemical and mechanical properties of the resulting biomaterials and, hence, their functionality. The collagen-based hydrogels, sponges, films and membranes presented here are some examples that have excellent biocompatible healing properties and can be further modified based on their use.
Author Contributions
Conceptualization, R.S. and N.A.; validation, R.S., N.A. and J.F.; writing—original draft preparation, R.S. and N.A.; writing—review and editing, R.S., N.A., J.F. and J.U.; visualization, R.S., M.J.L. and N.A.; supervision, J.F.; project administration, J.U.; funding acquisition, J.F. and J.U. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Institutional Support of Palacký University in Olomouc (RVO:61989592) and grant IGA_LF_2022_025.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The figures were created using BioRender.com, accessed on 1 October 2022. We thank May Griffith, Dept. of Ophthalmology and Institute of Biomedical Engineering, Université de Montréal and the Maisonneuve-Rosemont Hospital Research Centre, Montreal, Quebec, Canada, for hosting RS as an exchange student.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Parenteau-Bareil, R.; Gauvin, R.; Berthod, F. Collagen-Based Biomaterials for Tissue Engineering Applications. Materials 2010, 3, 1863–1887. [Google Scholar] [CrossRef] [Green Version]
- Son, Y.J.; Tse, J.W.; Zhou, Y.; Mao, W.; Yim, E.K.F.; Yoo, H.S. Biomaterials and controlled release strategy for epithelial wound healing. Biomater. Sci. 2019, 7, 4444–4471. [Google Scholar] [CrossRef] [PubMed]
- Netto, M.V.; Mohan, R.R.; Ambrósio, R.; Hutcheon, A.E.K.; Zieske, J.; Wilson, S. Wound Healing in the Cornea. Cornea 2005, 24, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Bukowiecki, A.; Hos, D.; Cursiefen, C.; Eming, S.A. Wound-Healing Studies in Cornea and Skin: Parallels, Differences and Opportunities. Int. J. Mol. Sci. 2017, 18, 1257. [Google Scholar] [CrossRef]
- Li, Y.; Jeong, J.; Song, W. Molecular Characteristics and Distribution of Adult Human Corneal Immune Cell Types. Front. Immunol. 2022, 13, 798346. [Google Scholar] [CrossRef]
- Nour, S.; Baheiraei, N.; Imani, R.; Khodaei, M.; Alizadeh, A.; Rabiee, N.; Moazzeni, S.M. A review of accelerated wound healing approaches: Biomaterial- assisted tissue remodeling. J. Mater. Sci. Mater. Med. 2019, 30, 120. [Google Scholar] [CrossRef]
- Frantz, C.; Stewart, K.M.; Weaver, V.M. The extracellular matrix at a glance. J. Cell Sci. 2010, 123, 4195–4200. [Google Scholar] [CrossRef] [Green Version]
- Ricard-Blum, S. The Collagen Family. Cold Spring Harb. Perspect. Biol. 2011, 3, a004978. [Google Scholar] [CrossRef] [Green Version]
- Shoulders, M.D.; Raines, R.T. Collagen Structure and Stability. Annu. Rev. Biochem. 2009, 78, 929–958. [Google Scholar] [CrossRef] [Green Version]
- Kananavičiūtė, R.; Kvederavičiūtė, K.; Dabkevičienė, D.; Mackevičius, G.; Kuisienė, N. Collagen-like sequences encoded by extremophilic and extremotolerant bacteria. Genomics 2019, 112, 2271–2281. [Google Scholar] [CrossRef]
- Yamauchi, M.; Taga, Y.; Hattori, S.; Shiiba, M.; Terajima, M. Methods in Cell Biology. In Analysis of Collagen and Elastin Cross-Links; Academic Press: Cambridge, MA, USA, 2018; Volume 143, pp. 115–132. [Google Scholar] [CrossRef]
- Costa, A.; Naranjo, J.D.; Londono, R.; Badylak, S.F. Biologic Scaffolds. Cold Spring Harb. Perspect. Med. 2017, 7, a025676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, M. Processing of collagen based biomaterials and the resulting materials properties. Biomed. Eng. Online 2019, 18, 1–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramshaw, J.A.M. Biomedical applications of collagens. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 104, 665–675. [Google Scholar] [CrossRef]
- Ramshaw, J.A.M.; Werkmeister, J.A.; Dumsday, G.J. Bioengineered collagens. Bioengineered 2014, 5, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.; Tang, C.; Xiong, S.; Yuan, Q.; Gu, Z.P.; Li, Z.; Hu, Y. Modification of Collagen for Biomedical Applications: A Review of Physical and Chemical Methods. Curr. Org. Chem. 2016, 20, 1797–1812. [Google Scholar] [CrossRef]
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef] [PubMed]
- Theocharis, A.D.; Manou, D.; Karamanos, N.K. The extracellular matrix as a multitasking player in disease. FEBS J. 2019, 286, 2830–2869. [Google Scholar] [CrossRef] [Green Version]
- Manou, D.; Caon, I.; Bouris, P.; Triantaphyllidou, I.-E.; Giaroni, C.; Passi, A.; Karamanos, N.K.; Vigetti, D.; Theocharis, A.D. The Complex Interplay between Extracellular Matrix and Cells in Tissues; Springer Nature: Berlin, Germany, 2019; Volume 1952, p. 485. [Google Scholar] [CrossRef]
- Theocharis, A.D.; Skandalis, S.S.; Gialeli, C.; Karamanos, N.K. Extracellular matrix structure. Adv. Drug Deliv. Rev. 2016, 97, 4–27. [Google Scholar] [CrossRef]
- Karamanos, N.K. Extracellular matrix: Key structural and functional meshwork in health and disease. FEBS J. 2019, 286, 2826–2829. [Google Scholar] [CrossRef] [Green Version]
- Vindin, H.; Mithieux, S.M.; Weiss, A.S. Elastin architecture. Matrix Biol. 2019, 84, 4–16. [Google Scholar] [CrossRef]
- Kular, J.K.; Basu, S.; Sharma, R.I. The extracellular matrix: Structure, composition, age-related differences, tools for analysis and applications for tissue engineering. J. Tissue Eng. 2014, 5, 2041731414557112. [Google Scholar] [CrossRef]
- Parisi, L.; Toffoli, A.; Ghezzi, B.; Mozzoni, B.; Lumetti, S.; Macaluso, G.M. A glance on the role of fibronectin in controlling cell response at biomaterial interface. Jpn. Dent. Sci. Rev. 2019, 56, 50–55. [Google Scholar] [CrossRef]
- Sabatier, L.; Chen, D.; Fagotto-Kaufmann, C.; Hubmacher, D.; McKee, M.D.; Annis, D.S.; Mosher, D.F.; Reinhardt, D.P. Fibrillin Assembly Requires Fibronectin. Mol. Biol. Cell 2009, 20, 846–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köwitsch, A.; Zhou, G.; Groth, T. Medical application of glycosaminoglycans: A review. J. Tissue Eng. Regen. Med. 2017, 12, e23–e41. [Google Scholar] [CrossRef] [PubMed]
- Kechagia, J.Z.; Ivaska, J.; Roca-Cusachs, P. Integrins as biomechanical sensors of the microenvironment. Nat. Rev. Mol. Cell Biol. 2019, 20, 457–473. [Google Scholar] [CrossRef] [PubMed]
- Harburger, D.S.; Calderwood, D.A. Integrin signalling at a glance. J. Cell Sci. 2009, 122, 159–163. [Google Scholar] [CrossRef] [Green Version]
- Pankov, R.; Yamada, K.M. Fibronectin at a glance. J. Cell Sci. 2002, 115, 3861–3863. [Google Scholar] [CrossRef] [Green Version]
- Rousselle, P.; Montmasson, M.; Garnier, C. Extracellular matrix contribution to skin wound re-epithelialization. Matrix Biol. 2018, 75–76, 12–26. [Google Scholar] [CrossRef]
- Dhavalikar, P.; Robinson, A.; Lan, Z.; Jenkins, D.; Chwatko, M.; Salhadar, K.; Jose, A.; Kar, R.; Shoga, E.; Kannapiran, A.; et al. Review of Integrin-Targeting Biomaterials in Tissue Engineering. Adv. Health Mater. 2020, 9, 2000795. [Google Scholar] [CrossRef]
- Mezu-Ndubuisi, O.J.; Maheshwari, A. The role of integrins in inflammation and angiogenesis. Pediatr. Res. 2020, 89, 1619–1626. [Google Scholar] [CrossRef]
- Zeltz, C.; Gullberg, D. The integrin–collagen connection–a glue for tissue repair? J. Cell Sci. 2016, 129, 653–664. [Google Scholar] [CrossRef] [Green Version]
- Adamiak, K.; Sionkowska, A. Current methods of collagen cross-linking: Review. Int. J. Biol. Macromol. 2020, 161, 550–560. [Google Scholar] [CrossRef]
- Heino, J. The collagen family members as cell adhesion proteins. BioEssays 2007, 29, 1001–1010. [Google Scholar] [CrossRef]
- Lorenzo-Martín, E.; Gallego-Muñoz, P.; Mar, S.; Fernández, I.; Cidad, P.; Martínez-García, M.C. Dynamic changes of the extracellular matrix during corneal wound healing. Exp. Eye Res. 2019, 186, 107704. [Google Scholar] [CrossRef]
- Torricelli, A.A.M.; Singh, V.; Santhiago, M.R.; Wilson, S.E. The Corneal Epithelial Basement Membrane: Structure, Function, and Disease. Investig. Opthalmol. Vis. Sci. 2013, 54, 6390–6400. [Google Scholar] [CrossRef]
- Coupry, I.; Sibon, I.; Mortemousque, B.; Rouanet, F.; Miné, M.; Goizet, C. Ophthalmological Features Associated With COL4A1 Mutations. Arch. Ophthalmol. 2010, 128, 483–489. [Google Scholar] [CrossRef]
- Wiegand, C.; Schönfelder, U.; Abel, M.; Ruth, P.; Kaatz, M.; Hipler, U.-C. Protease and pro-inflammatory cytokine concentrations are elevated in chronic compared to acute wounds and can be modulated by collagen type I in vitro. Arch. Dermatol. Res. 2009, 302, 419–428. [Google Scholar] [CrossRef]
- Metzmacher, I.; Ruth, P.; Abel, M.; Friess, W. In vitro binding of matrix metalloproteinase-2 (MMP-2), MMP-9, and bacterial collagenase on collagenous wound dressings. Wound Repair Regen. 2007, 15, 549–555. [Google Scholar] [CrossRef]
- Schönfelder, U.; Abel, M.; Wiegand, C.; Klemm, D.; Elsner, P.; Hipler, U.-C. Influence of selected wound dressings on PMN elastase in chronic wound fluid and their antioxidative potential in vitro. Biomaterials 2005, 26, 6664–6673. [Google Scholar] [CrossRef]
- Ryšavá, A.; Čížková, K.; Franková, J.; Roubalová, L.; Ulrichová, J.; Vostálová, J.; Vrba, J.; Zálešák, B.; Svobodová, A.R. Effect of UVA radiation on the Nrf2 signalling pathway in human skin cells. J. Photochem. Photobiol. B Biol. 2020, 209, 111948. [Google Scholar] [CrossRef]
- Wang, P.-H.; Huang, B.-S.; Horng, H.-C.; Yeh, C.-C.; Chen, Y.-J. Wound healing. J. Chin. Med Assoc. 2018, 81, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Sarveswaran, K.; Kurz, V.; Dong, Z.; Tanaka, T.; Penny, S.; Timp, G. Synthetic Capillaries to Control Microscopic Blood Flow. Sci. Rep. 2016, 6, 21885. [Google Scholar] [CrossRef] [Green Version]
- Alberts, B.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. Molecular Biology of the Cell, 4th ed.; Garland Science: New York, NY, USA, 2002. [Google Scholar]
- Mosier, D. Chapter 2-Vascular Disorders and Thrombosis1. In Pathologic Basis of Veterinary Disease, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 44–72.e1. [Google Scholar]
- Golebiewska, E.M.; Poole, A.W. Platelet secretion: From haemostasis to wound healing and beyond. Blood Rev. 2015, 29, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farndale, R.W.; Sixma, J.J.; Barnes, M.J.; De Groot, P.G. The role of collagen in thrombosis and hemostasis. J. Thromb. Haemost. 2004, 2, 561–573. [Google Scholar] [CrossRef]
- Schultz, G.S.; Davidson, J.M.; Kirsner, R.S.; Bornstein, P.; Herman, I.M. Dynamic reciprocity in the wound microenvironment. Wound Repair Regen. 2011, 19, 134–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 2014, 6, 265sr6. [Google Scholar] [CrossRef] [Green Version]
- DiPietro, L.A. Angiogenesis and wound repair: When enough is enough. J. Leukoc. Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Demling, R. Nutrition, anabolism, and the wound healing process: An overview. Eplasty 2009, 9, e9. [Google Scholar]
- Roh, J.S.; Sohn, D.H. Damage-Associated Molecular Patterns in Inflammatory Diseases. Immune Netw. 2018, 18, e27. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Ridiandries, A.; Tan, J.T.M.; Bursill, C.A. The Role of Chemokines in Wound Healing. Int. J. Mol. Sci. 2018, 19, 3217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revilla, G.; Darwin, E.; Rantam, F. Effect of Allogeneic Bone Marrow-mesenchymal Stem Cells (BM-MSCs) to Accelerate Burn Healing of Rat on the Expression of Collagen Type I and Integrin α2β1. Pak. J. Biol. Sci. 2016, 19, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, R.; Liang, H.; Clarke, E.; Jackson, C.; Xue, M. Inflammation in Chronic Wounds. Int. J. Mol. Sci. 2016, 17, 2085. [Google Scholar] [CrossRef]
- Twardowski, T.; Fertala, A.; Orgel, J.; Antonio, J.S. Type I Collagen and Collagen Mimetics as Angiogenesis Promoting Superpolymers. Curr. Pharm. Des. 2007, 13, 3608–3621. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. Fibroblast—Extracellular Matrix Interactions in Tissue Fibrosis. Curr. Pathobiol. Rep. 2016, 4, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Ramasastry, S.S. Acute Wounds. Clin. Plast. Surg. 2005, 32, 195–208. [Google Scholar] [CrossRef]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; La Rosa, C.C.-D.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef]
- Pastar, I.; Stojadinovic, O.; Yin, N.C.; Ramirez, H.; Nusbaum, A.G.; Sawaya, A.; Patel, S.B.; Khalid, L.; Isseroff, R.R.; Tomic-Canic, M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care 2014, 3, 445–464. [Google Scholar] [CrossRef] [Green Version]
- Reinke, J.; Sorg, H. Wound Repair and Regeneration. Eur. Surg. Res. 2012, 49, 35–43. [Google Scholar] [CrossRef]
- Velnar, T.; Bailey, T.; Smrkolj, V. The Wound Healing Process: An Overview of the Cellular and Molecular Mechanisms. J. Int. Med. Res. 2009, 37, 1528–1542. [Google Scholar] [CrossRef]
- Ljubimov, A.V.; Saghizadeh, M. Progress in corneal wound healing. Prog. Retin. Eye Res. 2015, 49, 17–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero-Moreno, A.; Baudouin, C.; Parsadaniantz, S.M.; Goazigo, A.R.-L. Morphological and Functional Changes of Corneal Nerves and Their Contribution to Peripheral and Central Sensory Abnormalities. Front. Cell. Neurosci. 2020, 14, 610342. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, M.S. Anatomy of cornea and ocular surface. Indian J. Ophthalmol. 2018, 66, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Kamil, S.; Mohan, R.R. Corneal stromal wound healing: Major regulators and therapeutic targets. Ocul. Surf. 2021, 19, 290–306. [Google Scholar] [CrossRef] [PubMed]
- Azimzade, Y.; Hong, J.; Mashaghi, A. Immunophysical analysis of corneal neovascularization: Mechanistic insights and implications for pharmacotherapy. Sci. Rep. 2017, 7, 12220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clahsen, T.; Büttner, C.; Hatami, N.; Reis, A.; Cursiefen, C. Role of Endogenous Regulators of Hem- And Lymphangiogenesis in Corneal Transplantation. J. Clin. Med. 2020, 9, 479. [Google Scholar] [CrossRef] [Green Version]
- Di Zazzo, A.; Gaudenzi, D.; Yin, J.; Coassin, M.; Fernandes, M.; Dana, R.; Bonini, S. Corneal angiogenic privilege and its failure. Exp. Eye Res. 2021, 204, 108457. [Google Scholar] [CrossRef]
- Adams, J.C.; Lawler, J. The Thrombospondins. Cold Spring Harb. Perspect. Biol. 2011, 3, a009712. [Google Scholar] [CrossRef] [Green Version]
- Dawson, D.W.; Volpert, O.V.; Gillis, P.; Crawford, S.E.; Xu, H.-J.; Benedict, W.; Bouck, N.P. Pigment Epithelium-Derived Factor: A Potent Inhibitor of Angiogenesis. Science 1999, 285, 245–248. [Google Scholar] [CrossRef]
- Mukwaya, A.; Jensen, L.; Lagali, N. Relapse of pathological angiogenesis: Functional role of the basement membrane and potential treatment strategies. Exp. Mol. Med. 2021, 53, 189–201. [Google Scholar] [CrossRef]
- Ellenberg, D.; Azar, D.T.; Hallak, J.A.; Tobaigy, F.; Han, K.Y.; Jain, S.; Zhou, Z.; Chang, J.-H. Novel aspects of corneal angiogenic and lymphangiogenic privilege. Prog. Retin. Eye Res. 2010, 29, 208–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.-H.; Huang, Y.-H.; Cunningham, C.M.; Han, K.-Y.; Chang, M.; Seiki, M.; Zhou, Z.; Azar, D.T. Matrix metalloproteinase 14 modulates signal transduction and angiogenesis in the cornea. Surv. Ophthalmol. 2015, 61, 478–497. [Google Scholar] [CrossRef] [PubMed]
- Sharif, Z.; Sharif, W. Corneal neovascularization: Updates on pathophysiology, investigations & management. Romanian J. Ophthalmol. 2019, 63, 15–22. [Google Scholar] [CrossRef]
- Abdelfattah, N.S.; Amgad, M.; Zayed, A.A. Host immune cellular reactions in corneal neovascularization. Int. J. Ophthalmol. 2016, 9, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Hadrian, K.; Willenborg, S.; Bock, F.; Cursiefen, C.; Eming, S.A.; Hos, D. Macrophage-Mediated Tissue Vascularization: Similarities and Differences Between Cornea and Skin. Front. Immunol. 2021, 12, 667830. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-H.; Garg, N.K.; Lunde, E.; Han, K.-Y.; Jain, S.; Azar, D.T. Corneal Neovascularization: An Anti-VEGF Therapy Review. Surv. Ophthalmol. 2012, 57, 415–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahriary, A.; Sabzevari, M.; Jadidi, K.; Yazdani, F.; Aghamollaei, H. The Role of Inflammatory Cytokines in Neovascularization of Chemical Ocular Injury. Ocul. Immunol. Inflamm. 2021, 30, 1149–1161. [Google Scholar] [CrossRef]
- Lee, H.-K.; Lee, S.-M.; Lee, D.-I. Corneal Lymphangiogenesis: Current Pathophysiological Understandings and Its Functional Role in Ocular Surface Disease. Int. J. Mol. Sci. 2021, 22, 11628. [Google Scholar] [CrossRef]
- Zahir-Jouzdani, F.; Atyabi, F.; Mojtabavi, N. Interleukin-6 participation in pathology of ocular diseases. Pathophysiology 2017, 24, 123–131. [Google Scholar] [CrossRef]
- Zhang, W.; Magadi, S.; Li, Z.; Smith, C.W.; Burns, A.R. IL-20 promotes epithelial healing of the injured mouse cornea. Exp. Eye Res. 2017, 154, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Hanna, C.; O’Brien, J.E. Cell Production and Migration in the Epithelial Layer of the Cornea. Arch. Ophthalmol. 1960, 64, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Mohan, R.R.; Mohan, R.R.; Ambrósio, R.; Hong, J.; Lee, J. The Corneal Wound Healing Response: Cytokine-mediated Interaction of the Epithelium, Stroma, and Inflammatory Cells. Prog. Retin. Eye Res. 2001, 20, 625–637. [Google Scholar] [CrossRef]
- Lu, L.; Reinach, P.S.; Kao, W.W.-Y. Corneal Epithelial Wound Healing. Exp. Biol. Med. 2001, 226, 653–664. [Google Scholar] [CrossRef]
- Amin, S.; Jalilian, E.; Katz, E.; Frank, C.; Yazdanpanah, G.; Guaiquil, V.H.; Rosenblatt, M.I.; Djalilian, A.R. The Limbal Niche and Regenerative Strategies. Vision 2021, 5, 43. [Google Scholar] [CrossRef]
- Sugioka, K.; Fukuda, K.; Nishida, T.; Kusaka, S. The fibrinolytic system in the cornea: A key regulator of corneal wound healing and biological defense. Exp. Eye Res. 2021, 204, 108459. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekher, G.; Ma, X.; Lallier, T.; Bazan, H. Delay of corneal epithelial wound healing and induction of keratocyte apoptosis by platelet-activating factor. Investig. Ophthalmol. V. Sci. 2002, 43, 1422–1428. [Google Scholar]
- Wilson, S.E. Fibrosis Is a Basement Membrane-Related Disease in the Cornea: Injury and Defective Regeneration of Basement Membranes May Underlie Fibrosis in Other Organs. Cells 2022, 11, 309. [Google Scholar] [CrossRef]
- Baratta, R.O.; Schlumpf, E.; Del Buono, B.J.; DeLorey, S.S.; Calkins, D.J. Corneal collagen as a potential therapeutic target in dry eye disease. Surv. Ophthalmol. 2021, 67, 60–67. [Google Scholar] [CrossRef]
- Wilson, S.E. Bowman’s layer in the cornea– structure and function and regeneration. Exp. Eye Res. 2020, 195, 108033. [Google Scholar] [CrossRef]
- Alberto, D.; Garello, R. Corneal Sublayers Thickness Estimation Obtained by High-Resolution FD-OCT. Int. J. Biomed. Imaging 2013, 2013, 11. [Google Scholar] [CrossRef]
- Wilson, S.E. Interleukin-1 and Transforming Growth Factor Beta: Commonly Opposing, but Sometimes Supporting, Master Regulators of the Corneal Wound Healing Response to Injury. Investig. Opthalmol. Vis. Sci. 2021, 62, 8. [Google Scholar] [CrossRef] [PubMed]
- Wagoner, M.D. Chemical injuries of the eye: Current concepts in pathophysiology and therapy. Surv. Ophthalmol. 1997, 41, 275–313. [Google Scholar] [CrossRef]
- Hong, J.; Liu, J.; Lee, J.; Mohan, R.; Mohan, R.; Woods, D.; He, Y.; Wilson, S. Proinflammatory chemokine induction in keratocytes and inflammatory cell infiltration into the cornea. Invest. Ophthalmol. Vis. Sci. 2001, 42, 2795–2803. [Google Scholar] [PubMed]
- Klingberg, F.; Hinz, B.; White, E.S. The myofibroblast matrix: Implications for tissue repair and fibrosis. J. Pathol. 2012, 229, 298–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.; Lewis, P.; Islam, M.M.; Doutch, J.; Sorensen, T.; White, T.; Griffith, M.; Meek, K.M. The structural and optical properties of type III human collagen biosynthetic corneal substitutes. Acta Biomater. 2015, 25, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Massoudi, D.; Malecaze, F.; Galiacy, S.D. Collagens and proteoglycans of the cornea: Importance in transparency and visual disorders. Cell Tissue Res. 2015, 363, 337–349. [Google Scholar] [CrossRef]
- Ishizaki, M.; Shimoda, M.; Wakamatsu, K.; Ogro, T.; Yamanaka, N.; Kao, C.W.-C.; Kao, W.W.-Y. Stromal fibroblasts are associated with collagen IV in scar tissues of alkali-burned and lacerated corneas. Curr. Eye Res. 1997, 16, 339–348. [Google Scholar] [CrossRef]
- Kempuraj, D.; Mohan, R.R. Autophagy in Extracellular Matrix and Wound Healing Modulation in the Cornea. Biomedicines 2022, 10, 339. [Google Scholar] [CrossRef]
- Chameettachal, S.; Prasad, D.; Parekh, Y.; Basu, S.; Singh, V.; Bokara, K.K.; Pati, F. Prevention of Corneal Myofibroblastic Differentiation In Vitro Using a Biomimetic ECM Hydrogel for Corneal Tissue Regeneration. ACS Appl. Bio Mater. 2020, 4, 533–544. [Google Scholar] [CrossRef]
- Chaurasia, S.S.; Lim, R.R.; Lakshminarayanan, R.; Mohan, R.R. Nanomedicine Approaches for Corneal Diseases. J. Funct. Biomater. 2015, 6, 277–298. [Google Scholar] [CrossRef]
- Hussain, N.A.; Figueiredo, F.C.; Connon, C.J. Use of biomaterials in corneal endothelial repair. Ther. Adv. Ophthalmol. 2021, 13, 25158414211058249. [Google Scholar] [CrossRef] [PubMed]
- Kocluk, Y.; Burcu, A.; Sukgen, E.A. Demonstration of cornea Dua’s layer at a deep anterior lamellar keratoplasty surgery. Oman J. Ophthalmol. 2016, 9, 179–181. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, R.C.; Wilson, S.E. Descemet’s membrane development, structure, function and regeneration. Exp. Eye Res. 2020, 197, 108090. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Overmass, M.; Fan, J.; Hodge, C.; Sutton, G.; Lovicu, F.J.; You, J. Application of Collagen I and IV in Bioengineering Transparent Ocular Tissues. Front. Surg. 2021, 8, 639500. [Google Scholar] [CrossRef] [PubMed]
- Vercammen, H.; Miron, A.; Oellerich, S.; Melles, G.R.; Dhubhghaill, S.N.; Koppen, C.; Bogerd, B.V.D. Corneal endothelial wound healing: Understanding the regenerative capacity of the innermost layer of the cornea. Transl. Res. 2022, 248, 111–127. [Google Scholar] [CrossRef]
- Miyamoto, T.; Sumioka, T.; Saika, S. Endothelial Mesenchymal Transition: A Therapeutic Target in Retrocorneal Membrane. Cornea 2010, 29, S52–S56. [Google Scholar] [CrossRef]
- Ishizaki, M.; Zhu, G.; Haseba, T.; Shafer, S.; Kao, W. Expression of collagen I, smooth muscle alpha-actin, and vimentin during the healing of alkali-burned and lacerated corneas. Invest. Ophthalmol. Vis. Sci. 1993, 32, 3320–3328. [Google Scholar]
- Tartaglia, G.; Cao, Q.; Padron, Z.; South, A. Impaired Wound Healing, Fibrosis, and Cancer: The Paradigm of Recessive Dystrophic Epidermolysis Bullosa. Int. J. Mol. Sci. 2021, 22, 5104. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Naomi, R.; Bahari, H.; Ridzuan, P.; Othman, F. Natural-Based Biomaterial for Skin Wound Healing (Gelatin vs. Collagen): Expert Review. Polymers 2021, 13, 2319. [Google Scholar] [CrossRef]
- Chouhan, D.; Mandal, B.B. Silk biomaterials in wound healing and skin regeneration therapeutics: From bench to bedside. Acta Biomater. 2019, 103, 24–51. [Google Scholar] [CrossRef]
- Matai, I.; Kaur, G.; Seyedsalehi, A.; McClinton, A.; Laurencin, C.T. Progress in 3D bioprinting technology for tissue/organ regenerative engineering. Biomaterials 2020, 226, 119536. [Google Scholar] [CrossRef] [PubMed]
- Davison-Kotler, E.; Marshall, W.S.; García-Gareta, E. Sources of Collagen for Biomaterials in Skin Wound Healing. Bioengineering 2019, 6, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew-Steiner, S.; Roy, S.; Sen, C. Collagen in Wound Healing. Bioengineering 2021, 8, 63. [Google Scholar] [CrossRef] [PubMed]
- Araujo, T.A.T.; Almeida, M.C.; Avanzi, I.; Parisi, J.; Sales, A.F.S.; Na, Y.; Renno, A. Collagen membranes for skin wound repair: A systematic review. J. Biomater. Appl. 2020, 36, 95–112. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Raines, R.T. Collagen-based biomaterials for wound healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef] [Green Version]
- Walimbe, T.; Panitch, A. Best of Both Hydrogel Worlds: Harnessing Bioactivity and Tunability by Incorporating Glycosaminoglycans in Collagen Hydrogels. Bioengineering 2020, 7, 156. [Google Scholar] [CrossRef]
- Sharma, S.; Rai, V.K.; Narang, R.K.; Markandeywar, T.S. Collagen-based formulations for wound healing: A literature review. Life Sci. 2021, 290, 120096. [Google Scholar] [CrossRef]
- Cziperle, D. Avitene™ Microfibrillar Collagen Hemostat for Adjunctive Hemostasis in Surgical Procedures: A Systematic Literature Review. Med. Dev. 2021, 14, 155–163. [Google Scholar] [CrossRef]
- Schimmer, C.; Gross, J.; Ramm, E.; Morfeld, B.-C.; Hoffmann, G.; Panholzer, B.; Hedderich, J.; Leyh, R.; Cremer, J.; Petzina, R. Prevention of surgical site sternal infections in cardiac surgery: A two-centre prospective randomized controlled study. Eur. J. Cardio-Thoracic Surg. 2016, 51, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.; Williams, C.; Yuan, T.; Bs, A.M.D.-F.; Bs, R.C.W.; Burton, T.; Hamlin, N.; Martinez, L. Comparative in vitro study of commercially available products for alveolar ridge preservation. J. Periodontol. 2021, 93, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Ruszczak, Z. Effect of collagen matrices on dermal wound healing. Adv. Drug Deliv. Rev. 2003, 55, 1595–1611. [Google Scholar] [CrossRef] [PubMed]
- Chia, C.L.K.; Shelat, V.G.; Low, W.; George, S.; Rao, J. The Use of Collatamp G, Local Gentamicin-Collagen Sponge, in Reducing Wound Infection. Int. Surg. 2014, 99, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Santhanam, R.; Rameli, M.A.P.; Al Jeffri, A.; Ismail, W.I.W. Bovine Based Collagen Dressings in Wound Care Management. J. Pharm. Res. Int. 2020, 32, 48–63. [Google Scholar] [CrossRef]
- Koehler, J.; Brandl, F.P.; Goepferich, A.M. Hydrogel wound dressings for bioactive treatment of acute and chronic wounds. Eur. Polym. J. 2018, 100, 1–11. [Google Scholar] [CrossRef]
- Moura, L.I.F.; Dias, A.M.A.; Carvalho, E.; de Sousa, H.C. Recent advances on the development of wound dressings for diabetic foot ulcer treatment—A review. Acta Biomater. 2013, 9, 7093–7114. [Google Scholar] [CrossRef] [Green Version]
- Karr, J.C.; Taddei, A.R.; Picchietti, S.; Gambellini, G.; Fausto, A.M.; Giorgi, F. A Morphological and Biochemical Analysis Comparative Study of the Collagen Products Biopad, Promogram, Puracol, and Colactive. Adv. Ski. Wound Care 2011, 24, 208–216. [Google Scholar] [CrossRef]
- Lo, S.; Fauzi, M. Current Update of Collagen Nanomaterials—Fabrication, Characterisation and Its Applications: A Review. Pharmaceutics 2021, 13, 316. [Google Scholar] [CrossRef]
- Kaur, J. Osteo-odonto keratoprosthesis: Innovative dental and ophthalmic blending. J. Indian Prosthodont. Soc. 2018, 18, 89–95. [Google Scholar] [CrossRef]
- Matthyssen, S.; Van den Bogerd, B.; Dhubhghaill, S.N.; Koppen, C.; Zakaria, N. Corneal regeneration: A review of stromal replacements. Acta Biomater. 2018, 69, 31–41. [Google Scholar] [CrossRef]
- Polisetti, N.; Islam, M.M.; Griffith, M. The Artificial Cornea. Corneal Regen. Med. 2013, 1014, 45–52. [Google Scholar] [CrossRef]
- Simpson, F.C.; McTiernan, C.D.; Islam, M.M.; Buznyk, O.; Lewis, P.N.; Meek, K.M.; Haagdorens, M.; Audiger, C.; Lesage, S.; Gueriot, F.-X.; et al. Collagen analogs with phosphorylcholine are inflammation-suppressing scaffolds for corneal regeneration from alkali burns in mini-pigs. Commun. Biol. 2021, 4, 608. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, Y.; Yan, Y.; Ji, Q.; Dai, Y.; Jin, S.; Liu, Y.; Chen, J.; Teng, L. A Sponge-Like Double-Layer Wound Dressing with Chitosan and Decellularized Bovine Amniotic Membrane for Promoting Diabetic Wound Healing. Polymers 2020, 12, 535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, X.; Shao, Z.; Li, C.; Yu, L.; Raja, M.A.; Liu, C. Isolation, Characterization and Evaluation of Collagen from Jellyfish Rhopilema esculentum Kishinouye for Use in Hemostatic Applications. PLoS ONE 2017, 12, e0169731. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Wang, J.; Si, Y.; Wang, X.; Deng, H.; Sheng, Z.; Li, Y.; Liu, J.; Zhao, J. A novel gene recombinant collagen hemostatic sponge with excellent biocompatibility and hemostatic effect. Int. J. Biol. Macromol. 2021, 178, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Sorushanova, A.; Skoufos, I.; Tzora, A.; Mullen, A.M.; Zeugolis, D.I. The influence of animal species, gender and tissue on the structural, biophysical, biochemical and biological properties of collagen sponges. J. Mater. Sci. Mater. Med. 2021, 32, 12. [Google Scholar] [CrossRef] [PubMed]
- Boyce, S.T.; Christianson, D.J.; Hansbrough, J.F. Structure of a collagen-GAG dermal skin substitute optimized for cultured human epidermal keratinocytes. J. Biomed. Mater. Res. 1988, 22, 939–957. [Google Scholar] [CrossRef]
- Pozzolini, M.; Gallus, L.; Ghignone, S.; Ferrando, S.; Candiani, S.; Bozzo, M.; Bertolino, M.; Costa, G.; Bavestrello, G.; Scarfì, S. Insights into the evolution of metazoan regenerative mechanisms: TGF superfamily member roles in tissue regeneration of the marine sponge Chondrosia reniformis Nardo, 1847. J. Exp. Biol. 2019, 222. [Google Scholar] [CrossRef] [Green Version]
- Chang, P.; Guo, B.; Hui, Q.; Liu, X.; Tao, K. A bioartificial dermal regeneration template promotes skin cell proliferation in vitro and enhances large skin wound healing in vivo. Oncotarget 2017, 8, 25226–25241. [Google Scholar] [CrossRef] [Green Version]
- Jinno, C.; Morimoto, N.; Ito, R.; Sakamoto, M.; Ogino, S.; Taira, T.; Suzuki, S. A Comparison of Conventional Collagen Sponge and Collagen-Gelatin Sponge in Wound Healing. BioMed Res. Int. 2016, 2016, 4567146. [Google Scholar] [CrossRef] [Green Version]
- Borene, M.L.; Barocas, V.H.; Hubel, A. Mechanical and cellular changes during compaction of a collagen-sponge-based corneal stromal equivalent. Ann. Biomed. Eng. 2004, 32, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Orwin, E.J.; Hubel, A. In Vitro Culture Characteristics of Corneal Epithelial, Endothelial, and Keratocyte Cells in a Native Collagen Matrix. Tissue Eng. 2000, 6, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Aswathy, S.; Narendrakumar, U.; Manjubala, I. Commercial hydrogels for biomedical applications. Heliyon 2020, 6, e03719. [Google Scholar] [CrossRef] [PubMed]
- Correa, S.; Grosskopf, A.K.; Hernandez, H.L.; Chan, D.; Yu, A.C.; Stapleton, L.M.; Appel, E.A. Translational Applications of Hydrogels. Chem. Rev. 2021, 121, 11385–11457. [Google Scholar] [CrossRef] [PubMed]
- Mude, L.; Sanapalli, B.K.R.; Narayanan, A.; Singh, S.K.; Karri, V.V.S.R. Overview of in situ gelling injectable hydrogels for diabetic wounds. Drug Dev. Res. 2021, 82, 503–522. [Google Scholar] [CrossRef] [PubMed]
- Bonnesœur, S.; Morin-Grognet, S.; Thoumire, O.; Le Cerf, D.; Boyer, O.; Vannier, J.; Labat, B. Hyaluronan-based hydrogels as versatile tumor-like models: Tunable ECM and stiffness with genipin-crosslinking. J. Biomed. Mater. Res. Part A 2020, 108, 1256–1268. [Google Scholar] [CrossRef]
- Ying, H.; Zhou, J.; Wang, M.; Su, D.; Ma, Q.; Lv, G.; Chen, J. In situ formed collagen-hyaluronic acid hydrogel as biomimetic dressing for promoting spontaneous wound healing. Mater. Sci. Eng. C 2019, 101, 487–498. [Google Scholar] [CrossRef]
- Tripathi, D.; Sharma, A.; Tyagi, P.; Beniwal, C.S.; Mittal, G.; Jamini, A.; Singh, H.; Tyagi, A. Fabrication of Three-Dimensional Bioactive Composite Scaffolds for Hemostasis and Wound Healing. AAPS PharmSciTech 2021, 22, 138. [Google Scholar] [CrossRef]
- Liu, L.; Wen, H.; Rao, Z.; Zhu, C.; Liu, M.; Min, L.; Fan, L.; Tao, S. Preparation and characterization of chitosan–collagen peptide/oxidized konjac glucomannan hydrogel. Int. J. Biol. Macromol. 2018, 108, 376–382. [Google Scholar] [CrossRef]
- Tripathi, D.; Rastogi, K.; Tyagi, P.; Rawat, H.; Mittal, G.; Jamini, A.; Singh, H.; Tyagi, A. Comparative Analysis of Collagen and Chitosan-based Dressing for Haemostatic and Wound Healing Application. AAPS PharmSciTech 2021, 22, 76. [Google Scholar] [CrossRef]
- Ding, C.; Tian, M.; Feng, R.; Dang, Y.; Zhang, M. Novel Self-Healing Hydrogel with Injectable, pH-Responsive, Strain-Sensitive, Promoting Wound-Healing, and Hemostatic Properties Based on Collagen and Chitosan. ACS Biomater. Sci. Eng. 2020, 6, 3855–3867. [Google Scholar] [CrossRef] [PubMed]
- Deng, A.; Yang, Y.; Du, S.; Yang, X.; Pang, S.; Wang, X.; Yang, S. Preparation of a recombinant collagen-peptide (RHC)-conjugated chitosan thermosensitive hydrogel for wound healing. Mater. Sci. Eng. C 2020, 119, 111555. [Google Scholar] [CrossRef] [PubMed]
- Meuli, M.; Hartmann-Fritsch, F.; Hüging, M.; Marino, D.; Saglini, M.; Hynes, S.; Neuhaus, K.; Manuel, E.; Middelkoop, E.; Reichmann, E.; et al. A Cultured Autologous Dermo-epidermal Skin Substitute for Full-Thickness Skin Defects: A Phase I, Open, Prospective Clinical Trial in Children. Plast. Reconstr. Surg. 2019, 144, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Dearman, B.L.; Boyce, S.T.; Greenwood, J.E. Advances in Skin Tissue Bioengineering and the Challenges of Clinical Translation. Front. Surg. 2021, 8, 640879. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.R.; Kondiah, P.P.D.; Choonara, Y.E.; Du Toit, L.C.; Ally, N.; Pillay, V. Hydrogel Biomaterials for Application in Ocular Drug Delivery. Front. Bioeng. Biotechnol. 2020, 8, 228. [Google Scholar] [CrossRef] [Green Version]
- Xeroudaki, M.; Thangavelu, M.; Lennikov, A.; Ratnayake, A.; Bisevac, J.; Petrovski, G.; Fagerholm, P.; Rafat, M.; Lagali, N. A porous collagen-based hydrogel and implantation method for corneal stromal regeneration and sustained local drug delivery. Sci. Rep. 2020, 10, 16936. [Google Scholar] [CrossRef]
- McCoy, M.G.; Seo, B.R.; Choi, S.; Fischbach, C. Collagen I hydrogel microstructure and composition conjointly regulate vascular network formation. Acta Biomater. 2016, 44, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Goodarzi, H.; Jadidi, K.; Pourmotabed, S.; Sharifi, E.; Aghamollaei, H. Preparation and in vitro characterization of cross-linked collagen–gelatin hydrogel using EDC/NHS for corneal tissue engineering applications. Int. J. Biol. Macromol. 2018, 126, 620–632. [Google Scholar] [CrossRef]
- Chen, Z.; You, J.; Liu, X.; Cooper, S.; Hodge, C.; Sutton, G.; Crook, J.M.; Wallace, G.G. Biomaterials for corneal bioengineering. Biomed. Mater. 2018, 13, 032002. [Google Scholar] [CrossRef] [Green Version]
- Jangamreddy, J.R.; Haagdorens, M.K.; Islam, M.M.; Lewis, P.; Samanta, A.; Fagerholm, P.; Liszka, A.; Ljunggren, M.K.; Buznyk, O.; Alarcon, E.I.; et al. Short peptide analogs as alternatives to collagen in pro-regenerative corneal implants. Acta Biomater. 2018, 69, 120–130. [Google Scholar] [CrossRef]
- Islam, M.M.; Ravichandran, R.; Olsen, D.; Ljunggren, M.K.; Fagerholm, P.; Lee, C.J.; Griffith, M.; Phopase, J. Self-assembled collagen-like-peptide implants as alternatives to human donor corneal transplantation. RSC Adv. 2016, 6, 55745–55749. [Google Scholar] [CrossRef]
- Fernandes-Cunha, G.M.; Chen, K.M.; Chen, F.; Le, P.; Han, J.H.; Mahajan, L.A.; Lee, H.J.; Na, K.S.; Myung, D. In situ-forming collagen hydrogel crosslinked via multi-functional PEG as a matrix therapy for corneal defects. Sci. Rep. 2020, 10, 16671. [Google Scholar] [CrossRef] [PubMed]
- Na, K.-S.; Fernandes-Cunha, G.M.; Varela, I.B.; Lee, H.J.; Seo, Y.A.; Myung, D. Effect of mesenchymal stromal cells encapsulated within polyethylene glycol-collagen hydrogels formed in situ on alkali-burned corneas in an ex vivo organ culture model. Cytotherapy 2021, 23, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Cėpla, V.; He, C.; Edin, J.; Rakickas, T.; Kobuch, K.; Ruželė, Z.; Jackson, W.B.; Rafat, M.; Lohmann, C.P.; et al. Functional fabrication of recombinant human collagen–phosphorylcholine hydrogels for regenerative medicine applications. Acta Biomater. 2015, 12, 70–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullins, R.; Richards, C.; Walker, T. Allergic reactions to oral, surgical and topical bovine collagen: Anaphylactic risk for surgeons. Aust. New Zealand J. Ophthalmol. 1996, 24, 257–260. [Google Scholar] [CrossRef]
- Pekar, J.E.; Magee, A.; Parker, E.; Moshiri, N.; Izhikevich, K.; Havens, J.L.; Gangavarapu, K.; Serrano, L.M.M.; Crits-Christoph, A.; Matteson, N.L.; et al. The molecular epidemiology of multiple zoonotic origins of SARS-CoV-2. Science 2022, 377, 960–966. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Kaczmarek, B.; Mazur, O. Collagen-Based Materials Modified by Phenolic Acids—A Review. Materials 2020, 13, 3641. [Google Scholar] [CrossRef]
- Shah, R.; Stodulka, P.; Skopalova, K.; Saha, P. Dual Crosslinked Collagen/Chitosan Film for Potential Biomedical Applications. Polymers 2019, 11, 2094. [Google Scholar] [CrossRef] [Green Version]
- Socrates, R.; Prymak, O.; Loza, K.; Sakthivel, N.; Rajaram, A.; Epple, M.; Kalkura, S.N. Biomimetic fabrication of mineralized composite films of nanosilver loaded native fibrillar collagen and chitosan. Mater. Sci. Eng. C 2019, 99, 357–366. [Google Scholar] [CrossRef]
Figure 1.
Diagrammatic overview of the extracellular matrix and its major components (e.g., collagens, elastin, proteoglycan complexes, fibronectin, and interacting integrins). Created with BioRender.com (accessed on 1 October 2022).
Figure 1.
Diagrammatic overview of the extracellular matrix and its major components (e.g., collagens, elastin, proteoglycan complexes, fibronectin, and interacting integrins). Created with BioRender.com (accessed on 1 October 2022).

Figure 3.
The main collagen forms used in biomaterials. Created with BioRender.com (accessed on 1 October 2022).
Figure 3.
The main collagen forms used in biomaterials. Created with BioRender.com (accessed on 1 October 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of the overview of commercial collagen materials used for skin healing.
| Wound Dressing Materials/Collagen Form | Product | References |
|---|---|---|
| Collagen sponges | Avitene™ Ultrafoam™ Collagen Sponge | [122,123] |
| GENTA-COLL® resorb | [124] | |
| Helistat® | [122,125] | |
| Microfibrillar Dressing Instat™ Mch Collagen | [122] | |
| Collatamp®-G | [126,127] | |
| Collagen films and membranes | SkinTemp® II | [126,128] |
| Fibracol® | [128,129,130] | |
| Promogran™/Promogran Prisma® | [126,128,130,131] | |
| CollaSorb® | [129,130] | |
| BIOPAD™ | [131] | |
| Puracol® Plus/Puracol® Plus Ag | [128,131] | |
| ColActive® Plus/ColActive® Plus Ag | [131] | |
| DermaCol™ | [128] | |
| Collagen hydrogels | HYCOL® | [128] |
| Collatek® | [128] | |
| CellerateRX® | [128,129] |
Table 2.
Summarizes the overview of currently developed non-commercial collagen materials discussed in this review.
Table 2.
Summarizes the overview of currently developed non-commercial collagen materials discussed in this review.
| Wound Dressing Materials/Collagen Form | Non-Commercial Product | References |
|---|---|---|
| Collagen sponges | Collagen sponge form jellyfish | [138] |
| Recombinant collagen hemostatic sponge | [139] | |
| Collagen sponge form porcine, bovine and human skin | [140] | |
| Platelet-rich plasma–collagen sponge | [143] | |
| Carboxymethyl chitosan–collagen peptides sponge | [144] | |
| Collagen I sponge | [145,146] | |
| Collagen hydrogels | Collagen–hyaluronan hydrogels | [150,151] |
| Collagen–chitosan hydrogels | [152,153,154,155,156] | |
| Collagen hydrogels with incorporated cells | [157,158] | |
| Collagen hydrogels (type I and III) | [159,160,161,162,163] | |
| Collagen-like peptides hydrogels | [136,164,165,166,167] | |
| Recombinant human collagen type III hydrogels | [168] | |
| Collagen hydrogels (form porcine) | [169] | |
| Collagen films and membranes | Collagen membranes | [119,171] |
| Collagen–chitosan films | [172,173,174] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sklenářová, R.; Akla, N.; Latorre, M.J.; Ulrichová, J.; Franková, J. Collagen as a Biomaterial for Skin and Corneal Wound Healing. J. Funct. Biomater. 2022, 13, 249. https://doi.org/10.3390/jfb13040249
AMA Style
Sklenářová R, Akla N, Latorre MJ, Ulrichová J, Franková J. Collagen as a Biomaterial for Skin and Corneal Wound Healing. Journal of Functional Biomaterials. 2022; 13(4):249. https://doi.org/10.3390/jfb13040249
Chicago/Turabian StyleSklenářová, Renáta, Naoufal Akla, Meagan Jade Latorre, Jitka Ulrichová, and Jana Franková. 2022. "Collagen as a Biomaterial for Skin and Corneal Wound Healing" Journal of Functional Biomaterials 13, no. 4: 249. https://doi.org/10.3390/jfb13040249
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.