
Impact of the Five-Year Intervention of an Antimicrobial Stewardship Program on the Optimal Selection of Surgical Prophylaxis in a Hospital without Antibiotic Prescription Restrictions in Costa Rica: A Retrospective Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Comparison of the Percentages of Optimal Selection and Duration of the Surgical Prophylactic Scheme, before and after the Implementation of the AMS
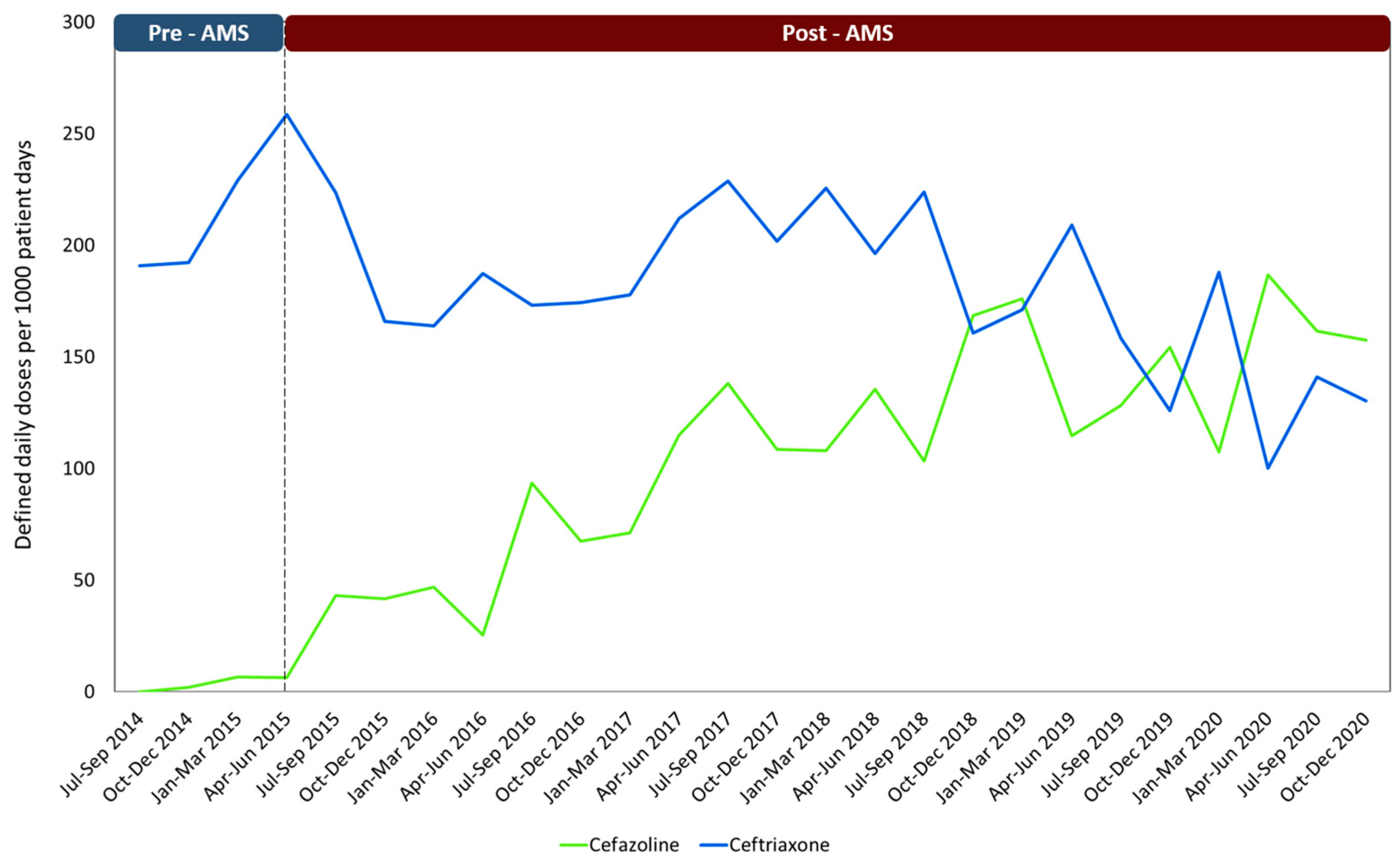
2.2. Changes in the Consumption of Antimicrobials from the Implementation of the AMS
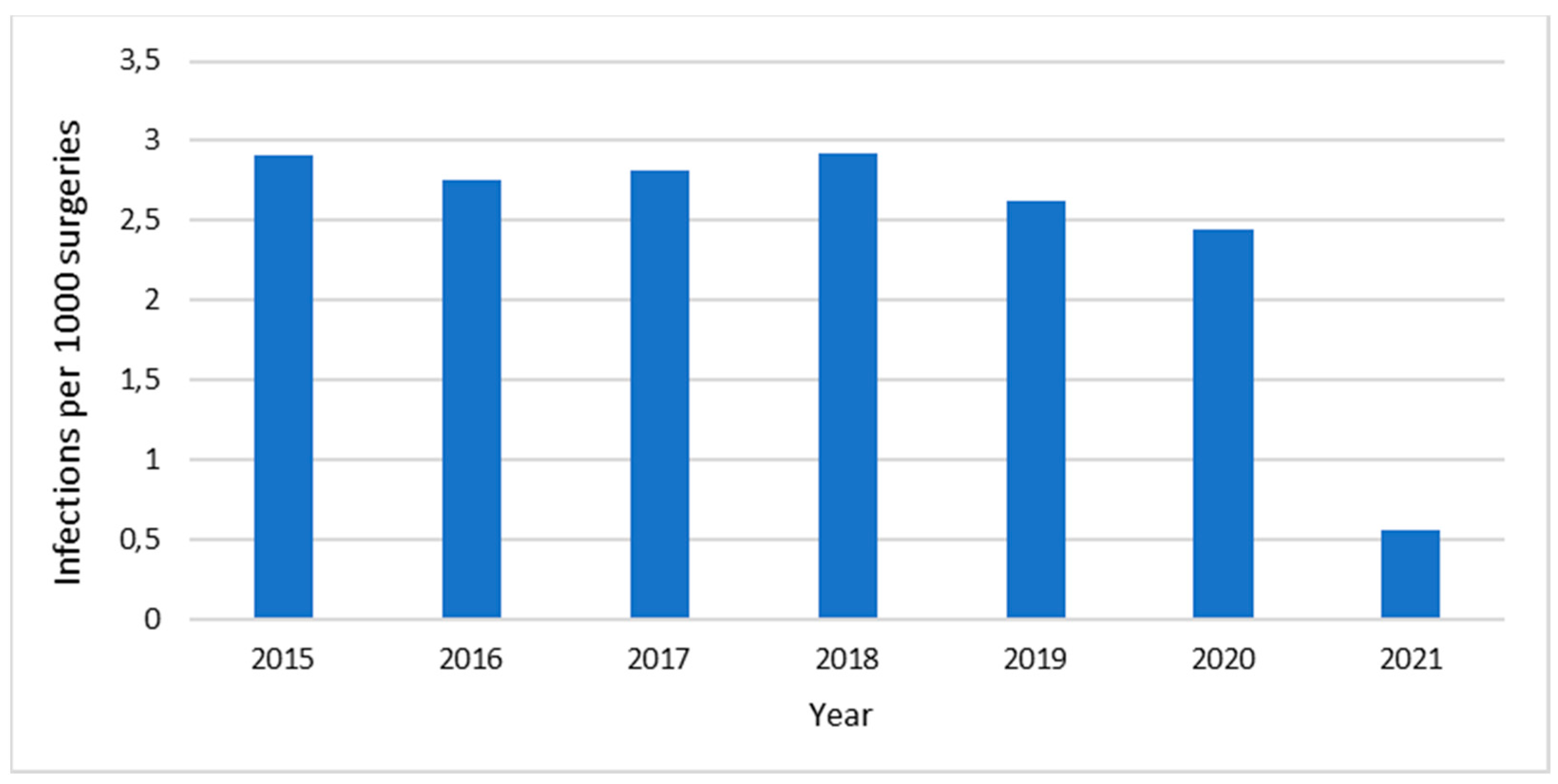
2.3. Adverse Effects Associated with Medications and Surgical Wound Infections
3. Discussion
4. Materials and Methods
4.1. Setting and Study Design
4.2. Data Collection
4.3. Outcome Measures
4.4. Statistical Analysis
4.5. Ethics Approval and Consent to Participate
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flasche, S.; Atkins, K.E. Balancing benefits and risks of antibiotic use. J. Infect. Dis. 2018, 218, 1351–1353. [Google Scholar] [CrossRef] [PubMed]
- Anesi, J.A.; Blumberg, E.A.; Han, J.H.; Lee, D.H.; Clauss, H.; Climaco, A.; Hasz, R.; Molnar, E.; Alimenti, D.; West, S.; et al. Risk factors for multidrug-resistant organisms among deceased organ donors. Am. J. Transplant. 2019, 19, 2468–2478. [Google Scholar] [PubMed]
- Thomas, G.R.; Corso, A.; Pasterán, F.; Shal, J.; Sosa, A.; Pillonetto, M.; Peral, R.T.d.S.; Hormazábal, J.C.; Araya, P.; Saavedra, S.Y.; et al. Increased Detection of Carbapenemase-Producing Enterobacterales Bacteria in Latin America and the Caribbean during the COVID-19 Pandemic. Emerg. Infect. Dis. J. 2022, 28, e220415. [Google Scholar] [CrossRef] [PubMed]
- García-Betancur, J.C.; Appel, T.M.; Esparza, G.; Gales, A.C.; Levy-Hara, G.; Cornistein, W.; Vega, S.; Nuñez, D.; Cuellar, L.; Bavestrello, L.; et al. Update on the epidemiology of carbapenemases in Latin America and the Caribbean. Expert Rev. Anti-Infect. Ther. 2021, 19, 197–213. [Google Scholar] [CrossRef]
- Martinez-Sobalvarro, J.V.; Júnior, A.A.P.; Pereira, L.B.; Baldoni, A.O.; Ceron, C.S.; Dos Reis, T.M. Antimicrobial stewardship for surgical antibiotic prophylaxis and surgical site infections: A systematic review. Int. J. Clin. Pharm. 2021, 44, 301–319. [Google Scholar] [CrossRef]
- Sartelli, M.; Duane, T.M.; Catena, F.; Tessier, J.M.; Coccolini, F.; Kao, L.S.; De Simone, B.; Labricciosa, F.M.; May, A.K.; Ansaloni, L.; et al. Antimicrobial Stewardship: A Call to Action for Surgeons. Surg. Infect. 2016, 17, 625–631. [Google Scholar] [CrossRef]
- Çakmakçi, M. Antibiotic stewardship programmes and the surgeon’s role. J. Hosp. Infect. 2015, 89, 264–266. [Google Scholar] [CrossRef]
- Cabral, S.M.; Harris, A.D.; Cosgrove, S.E.; Magder, L.S.; Tamma, P.D.; Goodman, K.E. Adherence to Antimicrobial Prophylaxis Guidelines for Elective Surgeries Across 825 US Hospitals, 2019–2020. Clin. Infect. Dis. 2023, 76, 2106–2115. [Google Scholar] [CrossRef]
- Huerta-Gutiérrez, R.; Braga, L.; Camacho-Ortiz, A.; Díaz-Ponce, H.; García-Mollinedo, L.; Guzmán-Blanco, M.; Valderrama-Beltrán, S.; Landaeta-Nezer, E.; Moreno-Espinosa, S.; Morfín-Otero, R.; et al. One-day point prevalence of healthcare-associated infections and antimicrobial use in four countries in Latin America. Int. J. Infect. Dis. 2019, 86, 157–166. [Google Scholar] [CrossRef]
- Hara, G.L.; Rojas-Cortés, R.; León, H.F.M.; Mansilla, A.D.; Orta, I.A.; Rizo-Amezquita, J.N.; Herrera, R.G.S.; de Ayala, S.M.; Villalobos, M.A.; Ponte, H.M.; et al. Point prevalence survey of antibiotic use in hospitals in Latin American countries. J. Antimicrob. Chemother. 2021, 77, 807–815. [Google Scholar] [CrossRef]
- Pierce, J.; Apisarnthanarak, A.; Schellack, N.; Cornistein, W.; Al Maani, A.; Adnan, S.; Stevens, M.P. Global Antimicrobial Stewardship with a Focus on Low-and Middle-Income Countries: A position statement for the international society for infectious diseases. Int. J. Infect. Dis. 2020, 96, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Branch-Elliman, W.; O’Brien, W.; Strymish, J.; Itani, K.; Wyatt, C.; Gupta, K. Association of Duration and Type of Surgical Prophylaxis with Antimicrobial-Associated Adverse Events. JAMA Surg. 2019, 154, 590–598. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Quirós, R.E.; Bardossy, A.C.; Angeleri, P.; Zurita, J.; Espinoza, W.R.A.; Carneiro, M.; Guerra, S.; Medina, J.; Luquerna, X.C.; Guerra, A.; et al. Antimicrobial stewardship programs in adult intensive care units in Latin America: Implementation, assessments, and impact on outcomes. Infect. Control Hosp. Epidemiol. 2022, 43, 181–190. [Google Scholar] [CrossRef]
- Hegewisch-Taylor, J.; Dreser-Mansilla, A.; Romero-Mónico, J.; Levy-Hara, G. Antimicrobial stewardship in hospitals in Latin America and the Caribbean: A scoping review. Rev. Panam. Salud Publica 2020, 44, e68. [Google Scholar] [CrossRef] [PubMed]
- Fabre, V.; Cosgrove, S.E.; Secaira, C.; Torrez, J.C.T.; Lessa, F.C.; Patel, T.S.; Quiros, R. Antimicrobial stewardship in Latin America: Past, present, and future. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e68. [Google Scholar] [CrossRef]
- Quirós, R.E. Programas de Optimización del Uso de Antimicrobianos en Latinoamérica. J. Infect. Control 2019, 8, 41–42. [Google Scholar]
- Campos-Lara, L.; Garro-Zamora, L.D.; Lizano-Barrantes, C. Hospital Mexico’s preoperative antibiotic prophylaxis protocol for orthopedic patients: A compliance analysis. Farm. Hosp. 2021, 45, 61–65. [Google Scholar]
- Restrepo-Arbeláez, N.; Garcia-Betancur, J.C.; Pallares, C.J.; Villegas, M.V. Antimicrobial Stewardship Programs in Latin America and the Caribbean: A Story of Perseverance, Challenges, and Goals. Antibiotics 2023, 12, 1342. [Google Scholar] [CrossRef] [PubMed]
- Hurst, A.L.; Child, J.; Pearce, K.; Palmer, C.; Todd, J.K.; Parker, S.K. Handshake Stewardship: A Highly Effective Rounding-based Antimicrobial Optimization Service. Pediatr. Infect. Dis. J. 2016, 35, 1104–1110. [Google Scholar] [CrossRef]
- Diaz Madriz, J.P.; Muñoz, G.; Zavaleta, E.; Chaverri, J.M.; Herrera, A. Impact of an antimicrobial stewardship program (asp) on the optimal selection of antibiotic prophylaxis in cesarean delivery in a hospital without restrictions on the use of antibiotics: First ASP in Costa Rica. Open Forum Infect. Dis. 2017, 4, S259. [Google Scholar] [CrossRef]
- World Health Organization. Improving the Quality of Health Services: Tools and Resources; WHO: Geneva, Switzerland, 2018.
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Health Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, U.; Sulaiman, S.A.S.; Adesiyun, A.G. Impact of pharmacist-led antibiotic stewardship interventions on compliance with surgical antibiotic prophylaxis in obstetric and gynecologic surgeries in Nigeria. PLoS ONE 2019, 14, e0213395. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; van den Bergh, D.; Netcare Antimicrobial Stewardship Study Alliance. From guidelines to practice: A pharmacist-driven prospective audit and feedback improvement model for peri-operative antibiotic prophylaxis in 34 South African hospitals. J. Antimicrob. Chemother. 2017, 72, 1227–1234. [Google Scholar] [CrossRef]
- Wang, J.; Dong, M.; Lu, Y.; Zhao, X.; Li, X.; Wen, A. Impact of pharmacist interventions on rational prophylactic antibiotic use and cost saving in elective cesarean section. Int. J. Clin. Pharmacol. Ther. 2015, 53, 605–615. [Google Scholar] [CrossRef]
- Zhou, X.; Gong, J.; Su, D.; Wu, Z.; Jia, X.; Wang, Y.; Xu, N.; Shang, J. Effect of pharmacist intervention on antibiotic prophylaxis in orthopedic internal fixation: A retrospective study. Res. Soc. Adm. Pharm. 2023, 19, 301–307. [Google Scholar] [CrossRef]
- Hassan, S.; Chan, V.; Stevens, J.; Stupans, I. Factors that influence adherence to surgical antimicrobial prophylaxis (SAP) guidelines: A systematic review. Syst. Rev. 2021, 10, 29. [Google Scholar] [CrossRef]
- Fuglestad, M.A.; Tracey, E.L.; Leinicke, J.A. Evidence-based prevention of surgical site infection. Surg. Clin. 2021, 101, 951–966. [Google Scholar] [CrossRef] [PubMed]
- MacBrayne, C.E.; Williams, M.C.; Levek, C.; Child, J.; Pearce, K.; Birkholz, M.; Todd, J.K.; Hurst, A.L.; Parker, S.K. Sustainability of Handshake Stewardship: Extending a Hand Is Effective Years Later. Clin. Infect. Dis. 2020, 70, 2325–2332. [Google Scholar] [CrossRef]
- Kim, S.-H.; Yoon, J.G.; Park, H.J.; Won, H.; Ryoo, S.S.; Choi, E.; Park, E.-K.; Huh, K.; Park, C.-M. Effects of a comprehensive antimicrobial stewardship program in a surgical intensive care unit. Int. J. Infect. Dis. 2021, 108, 237–243. [Google Scholar] [CrossRef]
- Meredith, J.; Roshdy, D.; Jaffa, R.K.; Medaris, L.A.; Aviles, C.; Cochran, A.; Fischer, K.; Shastry, V.; Davidson, L. 197. Bridging the Divide Between Antimicrobial Stewardship and Surgical Services: Successful Use of Handshake Stewardship with Hepato-Pancreato-Biliary Surgical Services in Adult Patients at a Large Academic Medical Center. Open Forum Infect. Dis. 2020, 7, S103. [Google Scholar] [CrossRef]
- Searns, J.B.; Williams, M.C.; MacBrayne, C.E.; Wirtz, A.L.; Leonard, J.E.; Boguniewicz, J.; Parker, S.K.; Grubenhoff, J.A. Handshake antimicrobial stewardship as a model to recognize and prevent diagnostic errors. Diagnosis 2021, 8, 347–352. [Google Scholar] [CrossRef]
- Zequinão, T.; Telles, J.P.; Gasparetto, J.; Tuon, F.F. Carbapenem stewardship with ertapenem and antimicrobial resistance—A scoping review. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200413. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Treggiari, M.M.; Michel, G.; Dai, F.; Tickoo, M.; Wai, M.; Schuster, K.; Mathis, M.; Shah, N.; Kheterpal, S.; et al. Adherence to Guidelines for the Administration of Intraoperative Antibiotics in a Nationwide US Sample. JAMA Netw. Open 2021, 4, e2137296. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Madriz, J.P.; Cordero-García, E.; Chaverri-Fernández, J.M.; Zavaleta-Monestel, E.; Murillo-Cubero, J.; Piedra-Navarro, H.; Hernández-Guillén, M.; Jiménez-Méndez, T. Impact of a pharmacist-driven antimicrobial stewardship program in a private hospital in Costa Rica. Rev. Panam. Salud Pública 2020, 44, e57. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2022. 2022. Available online: https://www.whocc.no/ (accessed on 1 March 2023).



{kind=link}
{kind=link}
| Procedure | Pre-AMS (N = 1598) | Post-AMS (N = 841) | p-Value | ||
|---|---|---|---|---|---|
| N (%) | Optimal Selection (%) | N (%) | Optimal Selection (%) | ||
| Cesarean delivery | 571 (35.7) | 1.8 | 247 (29.4) | 95.1 | 0.0001 |
| Orthopedic | 311 (19.5) | 43.4 | 182 (21.6) | 96.2 | 0.0001 |
| Head and neck | 103 (6.4) | 31.1 | 112 (13.3) | 28.6 | 0.6892 |
| Urologic | 107 (6.7) | 32.7 | 46 (5.5) | 93.5 | 0.0001 |
| Hysterectomy | 78 (4.9) | 2.6 | 54 (6.4) | 72.2 | 0.0001 |
| Plastic surgery | 95 (5.9) | 26.3 | 31 (3.7) | 93.5 | 0.0001 |
| Biliary tract | 61 (3.8) | 75.4 | 33 (3.9) | 90.9 | 0.0688 |
| Other procedures * | 272 (17.0) | 18.4 | 136 (16.2) | 64.7 | 0.0001 |
| Procedure | Pre-AMS (N = 1598) | Post-AMS (N = 841) | p-Value | ||
|---|---|---|---|---|---|
| N (%) | Optimal Duration (%) | N (%) | Optimal Duration (%) | ||
| Cesarean delivery | 571 (35.7) | 87.9 | 247 (29.4) | 98.0 | 0.0001 |
| Orthopedic | 311 (19.5) | 49.8 | 182 (21.6) | 65.4 | 0.0008 |
| Head and neck | 103 (6.4) | 60.2 | 112 (13.3) | 64.3 | 0.5353 |
| Urologic | 107 (6.7) | 53.3 | 46 (5.5) | 54.3 | 0.9124 |
| Hysterectomy | 78 (4.9) | 70.5 | 54 (6.4) | 94.4 | 0.0007 |
| Plastic surgery | 95 (5.9) | 66.3 | 31 (3.7) | 77.4 | 0.2460 |
| Biliary tract | 61 (3.8) | 72.1 | 33 (3.9) | 84.8 | 0.1645 |
| Other procedures * | 272 (17.0) | 61.0 | 136 (16.2) | 69.9 | 0.0767 |
| Antibiotics Selected as Surgical Prophylaxis | Pre-AMS N (%) | Post-AMS N (%) | p-Value |
|---|---|---|---|
| Ceftriaxone | 1168 (73.1) | 106 (12.6) | 0.0001 |
| Cefazolin | 0 (0) | 476 (56.6) | - |
| Cephalothin | 129 (8.1) | 20 (2.4) | 0.3628 |
| Ampicillin Sulbactam | 100 (6.3) | 32 (3.4) | 0.5353 |
| Ampicillin | 0 (0) | 28 (3.3) | - |
| Amoxicillin Sulbactam | 0 (0) | 53 (6.3) | - |
| Other antibiotics * | 198 (12.4) | 126 (15.0) | 0.5029 |
| Selected Antibiotic | Pre-AMS (DDD/1000 Patient Days) | Post-AMS (DDD/1000 Patient Days) | Magnitude of Difference | p-Value |
|---|---|---|---|---|
| Ceftriaxone | 217.7 | 139.8 | ▼ 77.9 | 0.0190 |
| Cefazolin | 14.9 | 153.3 | ▲ 149.6 | 0.0210 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Madriz, J.P.; Zavaleta-Monestel, E.; Villalobos-Madriz, J.A.; Rojas-Chinchilla, C.; Castrillo-Portillo, P.; Meléndez-Alfaro, A.; Vásquez-Mendoza, A.F.; Muñoz-Gutiérrez, G.; Arguedas-Chacón, S. Impact of the Five-Year Intervention of an Antimicrobial Stewardship Program on the Optimal Selection of Surgical Prophylaxis in a Hospital without Antibiotic Prescription Restrictions in Costa Rica: A Retrospective Study. Antibiotics 2023, 12, 1572. https://doi.org/10.3390/antibiotics12111572
Díaz-Madriz JP, Zavaleta-Monestel E, Villalobos-Madriz JA, Rojas-Chinchilla C, Castrillo-Portillo P, Meléndez-Alfaro A, Vásquez-Mendoza AF, Muñoz-Gutiérrez G, Arguedas-Chacón S. Impact of the Five-Year Intervention of an Antimicrobial Stewardship Program on the Optimal Selection of Surgical Prophylaxis in a Hospital without Antibiotic Prescription Restrictions in Costa Rica: A Retrospective Study. Antibiotics. 2023; 12(11):1572. https://doi.org/10.3390/antibiotics12111572
Chicago/Turabian StyleDíaz-Madriz, José Pablo, Esteban Zavaleta-Monestel, Jorge Arturo Villalobos-Madriz, Carolina Rojas-Chinchilla, Priscilla Castrillo-Portillo, Alison Meléndez-Alfaro, Ana Fernanda Vásquez-Mendoza, Gabriel Muñoz-Gutiérrez, and Sebastián Arguedas-Chacón. 2023. "Impact of the Five-Year Intervention of an Antimicrobial Stewardship Program on the Optimal Selection of Surgical Prophylaxis in a Hospital without Antibiotic Prescription Restrictions in Costa Rica: A Retrospective Study" Antibiotics 12, no. 11: 1572. https://doi.org/10.3390/antibiotics12111572